Meld dich an, um mehr Funktionen freizuschalten
- Speichere dieses Deck in deinem Konto
- Karteikarten mit Spaced Repetition lernen
- Als Anki (.apkg) oder PDF exportieren
- Verarbeite Dokumente mit bis zu 100 Seiten
- Bilder aus PDFs und Dokumenten extrahiert
- Bessere Textextraktion aus deinen PDFs und Dokumenten
- Bessere Karteikarten dank unseres leistungsstärkeren KI‑Modells
Clinical decision: 90-year-old woman with open tibial fracture refuses surgical stabilization but accepts irrigation/debridement and antibiotics. What is the next step?
Definition: What are the four criteria for medical decisional capacity?
Principle: Is decisional capacity global or decision-specific?
Legal distinction: Who determines a patient's global competence?
When is discussing the case with a durable power of attorney (son) appropriate?
When is petitioning the court to appoint a guardian appropriate for a patient with incapacity?
When is proceeding with recommended surgical treatment despite patient refusal justified?
When is using cast immobilization to honor a refusal appropriate for this open tibial fracture?
Practical: How should a clinician assess the 90-year-old patient's decisional capacity for refusing surgery?
Decisional capacity assessment: who must assess it?
Decisional capacity timing: when must assessment occur?
Decisional capacity and demographics: when should assessment be done relative to age or cognitive status?
Decisional capacity: concise rule combining actor, timing, and scope
Anchor: Initial step for asymptomatic elevated blood pressure (140/100) in 21-year-old
Anchor: Why no additional diagnostic studies now for isolated elevated BP in asymptomatic patient
Anchor: Primary determinants of blood pressure (3 systems)
Anchor: Risk factors contributing to primary (essential) hypertension
Anchor: When to measure serum aldosterone:renin ratio (hyperaldosteronism workup)
Anchor: Why aldosterone:renin ratio is unlikely in this patient
Anchor: When to evaluate renal artery stenosis (renal Doppler/arteriography)
Anchor: Why renal artery imaging is inappropriate now for this patient
Anchor: Role of renal CT scan in hypertension evaluation
Anchor: Next steps if hypertension is confirmed
Anchor: Educational point: long-term risks of untreated hypertension
Anchor: Image: slide with highlighted text (supplemental)
Primary hypertension: key risk factors (group 1)?
Primary hypertension: key risk factors (group 2)?
Primary hypertension: major long-term complications if untreated?
Primary hypertension: does a single elevated BP reading establish diagnosis?
Primary hypertension: acceptable methods to confirm elevated BP before diagnosis?
Primary hypertension: recommended timing for serial in-office BP measurements to confirm diagnosis?
Clinical decision: 18-year-old post-blunt chest trauma with left pleural effusion, tachycardia, tachypnea, rising O2 needs — most appropriate immediate management?
Pathophysiology: What causes traumatic hemothorax?
Presentation: Key clinical features of hemothorax?
Definition: When is hemothorax classified as massive?
Management decision: Purpose of initial tube thoracostomy in traumatic hemothorax?
When is video-assisted thoracoscopy (VATS) or thoracotomy indicated in hemothorax?
Ultrasonography role in blunt chest trauma with effusion: when is it appropriate?
CT chest role in traumatic hemothorax: when is CT appropriate?
Thoracentesis in traumatic pleural effusion: when is thoracentesis appropriate?
Comparison: Tube thoracostomy vs thoracentesis in traumatic hemothorax — main distinguishing indication?
Indicators of massive hemothorax (visual aid in answer)
What is hemothorax?
What are chest x-ray and CT features of hemothorax?
Which clinical signs mandate immediate tube thoracostomy for hemothorax?
Why is tube thoracostomy preferred over thoracentesis for large/rapid hemothorax?
When would thoracentesis be appropriate for pleural blood?
What is the primary therapeutic goal of tube thoracostomy in hemothorax?
Name complications of hemothorax (grouped into ≤3 items).
Imaging features of hemothorax (illustration)
Preoperative splenectomy: which vaccines are recommended?
Splenectomy: primary splenic immune functions?
Asplenia: which organisms cause increased severe infection risk?
Splenectomy patients: is antibiotic prophylaxis indicated and which agents?
Why is vaccinating for S. pneumoniae, H. influenzae, and N. meningitidis before splenectomy correct?
Why is answer choice A (only N. meningitidis) incorrect for preoperative splenectomy vaccination?
Why is answer choice B (only H. influenzae) incorrect for preoperative splenectomy vaccination?
Why is answer choice C (H. influenzae + N. meningitidis) incorrect for preoperative splenectomy vaccination?
Why is answer choice D (only S. pneumoniae) incorrect for preoperative splenectomy vaccination?
Why is answer choice E (S. pneumoniae + N. meningitidis) incorrect for preoperative splenectomy vaccination?
Why is answer choice F (S. pneumoniae + H. influenzae) incorrect for preoperative splenectomy vaccination?
Acute pancreatitis: classic presentation and key symptoms
Acute pancreatitis: common etiologies
Traumatic epigastric blow: diagnostic relevance
Acute pancreatitis: major complications
Acute pancreatitis: typical laboratory findings
Acute pancreatitis: initial supportive management
When is surgical intervention indicated in acute pancreatitis?
Esophageal rupture: presentation and causes
Gastric ulcer: symptoms and complications
Gastroenteritis: typical features and etiology
Hepatitis: causes and distinguishing features
Distinguish acute pancreatitis vs gastroenteritis (key differentiators)
Why pancreatitis is the correct diagnosis in a teen with epigastric pain after a kick
What is 'postpartum endometritis' (anchor: diagnosis)?
Pathophysiology of postpartum endometritis (anchor: pathophysiology)?
Key clinical features of postpartum endometritis (anchor: clinical features)?
Risk factors for postpartum endometritis (anchor: risk factors)?
Immediate management of suspected postpartum endometritis (anchor: management)?
Why is antibiotic therapy correct as the next step in this postpartum patient (anchor: answer-choice logic)?
Why is CT abdomen/pelvis not the best next step for suspected endometritis (anchor: answer-choice logic)?
When is CT abdomen/pelvis useful after postpartum fever (anchor: diagnostics)?
Why is culture of the lochia not the most appropriate next step (anchor: answer-choice logic)?
Why are endometrial biopsy and transvaginal ultrasound not the immediate next steps (anchor: answer-choice logic)?
Example presentation anchor: 36 hours postpartum with fever and foul-smelling lochia—most likely diagnosis?
Supplementary: slide illustrating key points about postpartum infection (anchor: visual aid)?
Smoking cessation and pulmonary function in a 37-year-old long-term smoker
Pathophysiology of normal aging lungs
Effect of smoking on age-related pulmonary decline
Diagnosis of chronic obstructive pulmonary disease (COPD)
Medical management for obstructive lung disease in long-term smokers
Oxygen therapy criteria in chronic lung disease
Lung cancer risk after smoking cessation (relation to choices B and D)
Why 'pulmonary function will not decrease further' is incorrect (choice C)
Smoking and risk of myocardial infarction versus cerebral infarction (relation to choice E)
Illustration: highlighted teaching points about smoking and lung aging
What is the diagnosis: multiple small (3–5 mm), bright red, slightly raised dome-shaped papules on trunk in a 38-year-old?
What are the typical clinical locations of cherry angiomas?
What is the histologic appearance of a cherry angioma?
What diagnostic study is most appropriate to confirm cherry angiomas?
When is excisional biopsy appropriate for cherry angiomas?
How should physicians manage patients who develop cherry angiomas?
Gastroenteritis: typical features and relation to blunt abdominal trauma?
When is acute pancreatitis likely and what lab findings support it?
Hepatitis: common causes and typical presentation features?
Visual: example appearance of cherry angiomas (illustration)
Diagnosis: Chronic bacterial prostatitis — key presenting features in this case?
Risk factors: What sexual history findings increase suspicion for chronic bacterial prostatitis?
Diagnostic test: What is the two-glass test for prostatitis?
Diagnostic criterion: How is prostate localization established using post-massage cultures?
Treatment: First-line therapy for chronic bacterial prostatitis?
Prognosis modifiers: Factors affecting cure rates for chronic bacterial prostatitis?
Choice rationale: When is CT pelvis useful instead of two-glass test for prostate-related disease?
Choice rationale: When is abdominal ultrasonography appropriate vs prostatitis testing?
Choice rationale: When is placement of urinary catheter for culture appropriate?
Diagnostic aid: Example of two-glass test visual aid
Chronic bacterial prostatitis: core presenting symptoms?
Chronic bacterial prostatitis: additional possible features?
Risk factors for chronic bacterial prostatitis?
Diagnostic test that establishes chronic bacterial prostatitis?
First-line treatment for chronic bacterial prostatitis?
Prognosis after treatment for chronic bacterial prostatitis?
When is transrectal prostate ultrasonography useful?
Why transrectal prostate ultrasonography is not diagnostic for chronic bacterial prostatitis?
When would transrectal ultrasonography be the correct test in prostatitis-like illness?
Foul-smelling or dark ejaculate: suggests which diagnosis over cystitis?
Diagnosis: Key features supporting cardiogenic shock in a 76-year-old man
Pathophysiology: How cardiogenic shock causes hypotension and pulmonary edema
Management: First-line pharmacologic therapy for cardiogenic shock after MI
Drug: Dobutamine mechanism relevant to cardiogenic shock
Drug: Norepinephrine role in cardiogenic shock
Comparison: Dobutamine vs Norepinephrine in cardiogenic shock
Drug: Why vasopressin (ADH) is not first-line for cardiogenic shock
Drug: Why isoproterenol is harmful after acute MI with cardiogenic shock
Drug: Why phenylephrine is not recommended as first-line in cardiogenic shock
Clinical decision: When to add a vasopressor to dobutamine in cardiogenic shock
Visual aid: Dobutamine mechanism and effect on hemodynamics (image on answer)
Cardiogenic shock: defining clinical presentation?
Cardiogenic shock: first-line therapy?
Dobutamine: role in cardiogenic shock?
Dopamine: role in cardiogenic shock?
Norepinephrine: role in cardiogenic shock?
Cardiogenic shock: summary slide (visual aid)?
Upper-extremity deep venous thrombosis (UEDVT): key pathophysiology
Upper-extremity DVT: typical clinical presentation
Why is venous thrombosis the most likely cause of this patient's unilateral arm swelling?
Diagnosis of upper-extremity DVT: preferred test and finding
Initial management of upper-extremity DVT
Arterial occlusion: when would this explain limb findings?
Compartment syndrome: pathophysiologic mechanism
Hematoma: clinical clues making it the correct cause of limb swelling
Lymphedema: distinguishing features vs venous obstruction
UEDVT epidemiology and typical setting
Bacterial tracheitis: key presenting signs in a child
Bacterial tracheitis: typical causative organisms
Bacterial tracheitis: characteristic chest x-ray finding
Bacterial tracheitis: first-line management
Why is croup (laryngotracheobronchitis) less likely in this child?
When is epiglottitis the correct diagnosis instead of bacterial tracheitis?
When is bronchiolitis the correct diagnosis instead of bacterial tracheitis?
When is peritonsillar abscess the correct diagnosis instead of bacterial tracheitis?
Bacterial tracheitis: diagnosis cues and role of imaging
Bacterial tracheitis: what is the definition?
Bacterial tracheitis: common presenting respiratory signs/symptoms?
Bacterial tracheitis: systemic symptom commonly present?
Bacterial tracheitis: typical chest auscultation findings?
Bacterial tracheitis: chest x-ray finding?
Bacterial tracheitis: first-line management components?
ar abscess unlikely: clinical statement
Bacterial tracheitis: supportive image illustrating tracheal air column (useful but not required to answer)
ECMO decision for a 37-year-old woman with cystic fibrosis, recurrent pulmonary failure, and refusal of lung transplant: what is the appropriate assessment?
Patient competence in treatment decisions: what is the documented status for this patient?
Scope of the patient's living will in this case:
Relevance of the patient's repeated refusal of lung transplant to decision-making:
Current respiratory support status of the patient in the ICU:
Why does the living will not automatically prohibit ECMO in this patient?
When should family members initiate medical treatment plans for a hospitalized patient?
Gastroenteritis: typical features described in the text
Acute pancreatitis: characteristic clinical presentation
Acute pancreatitis: diagnostic laboratory findings
Acute pancreatitis: possible relation to trauma per the text
Hepatitis: typical features and causes mentioned
Chronic transplant nephropathy: key pathophysiologic mechanism?
Chronic transplant nephropathy: typical clinical manifestations?
Chronic transplant nephropathy: diagnostic evaluation?
Chronic transplant rejection: response to standard immunosuppression?
Acute cellular rejection of a renal allograft: immune mediator and timing?
Gastroenteritis: typical features that distinguish it from transplant failure?
Examples of chronic rejection in other transplanted organs
Chronic transplant nephropathy: illustrative biopsy/ultrasound as supplement
Viral hepatitis: key lab pattern suggesting acute viral hepatitis in this case
Viral hepatitis: common causes of acute hepatitis listed
Viral hepatitis: common presenting symptoms
Viral hepatitis: initial serologic tests mentioned
Viral hepatitis: initial management approach
Cholangitis: clinical features and typical labs that distinguish it from viral hepatitis
Cholecystitis: presentation and typical lab expectations
Choledochal cyst: typical age, symptoms, and usual lab findings
Comparison: Why viral hepatitis fits this patient vs cholangitis or cholecystitis
Viral hepatitis: illustrative slide of teaching points (image on answer side)
Acute viral hepatitis: key clinical features?
Acute viral hepatitis: characteristic lab pattern?
Viruses often implicated in acute viral hepatitis (group 1)?
Viruses often implicated in acute viral hepatitis (group 2)?
Acute viral hepatitis: initial management approach?
Complications to manage in acute viral hepatitis?
Pancreatic pseudocyst: patient population and frequency?
Pancreatic pseudocyst: common presenting symptoms when symptomatic?
Acute pancreatitis: typical clinical presentation?
Pancreatitis: most common nontraumatic causes?
Pancreatitis: diagnostic lab marker specificity?
Why acute viral hepatitis is more likely than pancreatitis in a patient with very large ALT/AST rise and no clear pancreatitis history?
When would pancreatitis be the correct diagnosis instead of acute viral hepatitis?
When would pancreatic pseudocyst explain symptoms instead of acute viral hepatitis?
Clinical diagnosis: 9-year-old with 5-month intermittent right flank pain, absent left kidney on ultrasound, severe dilation of right renal pelvis. What is the clinical problem?
Pathophysiology: How does vesicoureteral reflux lead to kidney failure?
Key management: Most appropriate immediate intervention to prevent progression of renal failure from proximal ureteral obstruction in a single kidney?
Rationale: Why is percutaneous nephrostomy preferred here?
When is a urinary catheter the correct immediate intervention for urinary obstruction?
Why is a urinary catheter NOT appropriate for this patient?
When is cystoscopy with bladder outlet dilatation appropriate for urinary obstruction?
Why is cystoscopy with bladder outlet dilatation NOT appropriate for this patient?
When is intravenous furosemide indicated in renal/volume management?
Why is intravenous furosemide inappropriate in obstruction-related hydronephrosis?
When is IV 0.9% saline bolus indicated in acute management?
Why is IV 0.9% saline bolus inappropriate for this patient?
Congenital urinary tract anomalies associated with ureteral obstruction or reflux (examples relevant to single-kidney patients)
Clinical priority in patients with unilateral renal agenesis
Ultrasound finding anchor: Absent left kidney and severe right renal pelvic dilation implies what immediate risk?
Supplement: Illustration of hydronephrosis in single kidney—useful for visualizing severe renal pelvis dilation
Percutaneous nephrostomy tube: primary clinical indication?
Vesicoureteral reflux (VUR) or ureteral obstruction: role of percutaneous nephrostomy?
Percutaneous nephrostomy tube: intended immediate benefit to renal function?
Anchor: Nonadherence in 21-year-old with type 2 diabetes; defining features?
Anchor: Best physician approach for young diabetic nonadherent due to social perception
Anchor: Why multidisciplinary care + peer support is correct for social-perception nonadherence?
Anchor: When is contacting a patient's parent appropriate?
Anchor: When is a mobile glucose app likely effective for nonadherence?
Anchor: When is scare/threatening counseling (eg, 'you will be blind') appropriate?
Anchor: Use of humor with a patient admitting nonadherence due to social stigma
Anchor: Clinical communication principle for nonadherence evaluation
Anchor: Study-note rule: overriding refusals or contacting others
Anchor: Choice E — strengthen physician-patient relationship. Why is this option insufficient for treatment nonadherence?
Anchor: Treatment nonadherence. Common practical reasons (group A)?
Anchor: Treatment nonadherence. Common psychosocial reasons (group B)?
Anchor: Approach to a nonadherent patient. What clinician attitude is recommended?
Anchor: When is peer support indicated for a nonadherent patient?
Anchor: Use of image. What supplementary purpose can a highlighted slide image serve when teaching about nonadherence?
Diagnosis: Tingling in left ring and small fingers + medial forearm sensory loss in a 62-year-old with left arm dialysis fistula — most likely diagnosis?
Pathophysiology: How does an elbow arteriovenous fistula cause neuropathy?
Feature: Sensory distribution of ulnar nerve compression at the elbow?
Feature: Motor findings expected with ulnar nerve compression at the wrist vs elbow?
Diagnostic test to confirm suspected ulnar nerve compression?
Initial management for ulnar nerve compression related to dialysis fistula?
When is surgery indicated for ulnar nerve compression?
Arteriovenous steal syndrome: when would this diagnosis fit in a dialysis patient?
Why is diabetic neuropathy unlikely to explain isolated ring/small finger and medial forearm sensory loss?
Why are central causes (eg, cerebral infarction) unlikely for isolated medial hand and forearm sensory loss?
Use of provided image: What clinical sign near a dialysis fistula suggests local hemodynamic device presence without inflammation?
Essential (pre-existing) hypertension in pregnancy: diagnostic blood pressure criteria and timing?
Why is the 37-year-old patient in the vignette diagnosed with essential hypertension?
Normal urine protein result significance in essential hypertension during pregnancy?
Gestational hypertension: when would this diagnosis apply?
Preeclampsia: defining feature that distinguishes it from essential hypertension?
Superimposed preeclampsia on essential hypertension: when is this diagnosis correct?
Transient hypertension in pregnancy: defining features?
Physiologic blood pressure change in early pregnancy relevant to diagnosis?
Maternal and fetal risks associated with essential hypertension in pregnancy?
Initial management principles for essential hypertension in pregnancy?
Slide image: visual highlight of teaching points (supplementary)
Diagnosis: 42-year-old transplant patient with Ca2+ 11.7 mg/dL and PTH 425 pg/mL; chronic kidney failure history. What is the most likely diagnosis?
Pathophysiology: What causes tertiary hyperparathyroidism in chronic kidney disease?
Lab pattern: What combination of serum calcium and PTH occurs in tertiary hyperparathyroidism?
Treatment: Primary management for tertiary hyperparathyroidism?
Why is hypervitaminosis D (excess vitamin D) an unlikely cause of this patient's labs?
When would hypervitaminosis A be the correct diagnosis instead of tertiary hyperparathyroidism?
Why is parathyroid adenoma (primary hyperparathyroidism) less likely in this patient with CKD history?
Why is thyrotoxicosis an unlikely explanation for this patient's hypercalcemia and PTH elevation?
Clinical features of hyperparathyroidism to recognize in patients:
Distinguishing parathyroid hyperplasia vs adenoma in hyperparathyroidism context:
Define the procedure parathyroidectomy.
Meningococcal disease: key clinical presentation
Neisseria meningitidis: important epidemiologic risk factor
Definition of 'close contacts' for meningococcal prophylaxis
Management anchor: appropriate prophylaxis strategy for hospital personnel exposed to N. meningitidis
Why prophylaxis for close contacts is correct for meningococcal exposure
Why prophylaxis for all ED personnel on arrival (Choice A) is incorrect
Why prophylaxis for immunocompromised personnel only (Choice C) is incorrect
Why no prophylaxis for hospital personnel (Choice D) is incorrect
Preferred chemoprophylactic agents for meningococcal close contacts (set 1)
Preferred chemoprophylactic agent for meningococcal close contacts (set 2)
Diagnosis: What diagnosis is most consistent with acute onset severe dyspnea, hypoxemia (SpO2 88%), sinus tachycardia, 1+ bilateral leg edema, recent long-distance immobility (truck driving), and a chest x-ray shown?
Pathophysiology: What ABG pattern is associated with acute pulmonary embolism?
Risk factors: Which immobility-related risk is highlighted for PE in this case?
Diagnostic test choice: What is the preferred imaging to confirm suspected acute pulmonary embolism?
D-dimer use: When is a serum D-dimer assay appropriate for suspected PE?
BNP use: When is serum BNP measurement indicated instead of primary PE testing?
Cardiac enzymes: When is measurement of cardiac enzymes the appropriate next step?
Chest tube: When is placement of a chest tube indicated in acute respiratory presentation?
Steroids: When is IV hydrocortisone appropriate in acute dyspnea?
ECG/clinical features: What ECG and clinical findings are typical but nonspecific for PE?
Imaging supplement: Show chest x-ray image associated with the case (illustration only).
Pulmonary embolism: typical presenting features?
Pulmonary embolism: clinical risk factors that prompt rapid testing (group 1)?
Pulmonary embolism: additional clinical risk factors (group 2)?
Diagnostic test: preferred method to confirm pulmonary embolism?
D-dimer: limitation when Wells score indicates high pretest probability?
Obstructive shock from massive pulmonary embolism: best immediate management principle?
Hydrocortisone IV: when is it appropriate?
Hydrocortisone IV: why not appropriate for this patient with suspected PE?
Chest tube placement: appropriate indications?
Chest tube placement: why not appropriate for this patient?
Educational rule: when to test rapidly for pulmonary embolism?
Clinical anchor: 82-year-old man with urinary retention (1700 mL turbid urine), hypotension unresponsive to fluids and norepinephrine, leukocytosis, hyponatremia, hyperkalemia, elevated BUN/Cr — what is the most likely endocrine contributor to persistent hypotension?
Clinical anchor: Which laboratory pattern in this patient supports adrenal insufficiency as a contributor to shock?
Clinical anchor: What is the most appropriate immediate therapy for suspected adrenal insufficiency causing refractory septic hypotension?
Clinical anchor: Why is hydrocortisone indicated for vasopressor-refractory septic shock?
Clinical anchor: When would bladder irrigation with amphotericin B be appropriate instead of hydrocortisone?
Clinical anchor: When is intravenous fluconazole appropriate in a septic patient?
Clinical anchor: When is intravenous metronidazole appropriate in an infected patient with hypotension?
Clinical anchor: When is immediate hemodialysis indicated for hypotension with elevated BUN/Cr?
Clinical anchor: What acute urologic finding in this case likely precipitated the sepsis?
Clinical anchor: How does limited vasopressor responsiveness relate to endocrine causes of shock in sepsis?
Supplement: Slide illustrating key teaching (use as summary only)
Acute adrenal insufficiency: next immediate management for persistent hypotension after large-volume IV fluids and vasopressors?
Why is IV glucocorticoid therapy correct for acute adrenal insufficiency with refractory hypotension?
Pathophysiology of acute adrenal insufficiency mentioned in the text?
Indications for immediate hemodialysis per the text (group 1 of examples)?
Indications for immediate hemodialysis per the text (group 2 of examples)?
Why is emergent hemodialysis NOT appropriate for this patient now?
How should hemodynamic instability be managed relative to dialysis initiation?
When should you suspect acute adrenal insufficiency in a hypotensive patient?
Which clinical action is emphasized as more appropriate than starting antibiotics for this patient's hypotension?
Illustration: Slide showing highlighted teaching point about management of refractory hypotension — what does the image supplement?
Hodgkin lymphoma: typical systemic 'B' symptoms?
Hodgkin lymphoma: common patient age peaks?
Hodgkin lymphoma: pathognomonic biopsy finding?
Hodgkin lymphoma: required biopsy type for definitive diagnosis?
Fine-needle aspiration (FNA): when is it appropriate for suspected lymphoma?
After Hodgkin lymphoma confirmation by node biopsy: next best staging test?
Bronchoscopy: when is it indicated in suspected Hodgkin lymphoma?
Laparoscopy: role in Hodgkin lymphoma evaluation?
Pel-Ebstein fever: characteristic pattern in Hodgkin lymphoma?
Alcohol-induced lymph node pain: significance in Hodgkin lymphoma?
Laboratory markers often elevated in Hodgkin lymphoma?
Primary curative treatment approach for Hodgkin lymphoma?
Prognosis and staging uniqueness of Hodgkin lymphoma?
Diagnosis confirmation: what finding on lymph node biopsy confirms the diagnosis?
Clinical features: which systemic and organ findings may be present?
Staging evaluation: which imaging modalities assess extent of disease?
Treatment approach: what therapy is often curative for localized or bulky disease?
Imaging example: what scans are shown for extent evaluation (illustration)?
Diagnosis: 67-year-old with sudden substernal chest pain, troponin ↑, hypotension, ST elevation in II, III, aVF and V4R–V6R. What is the most likely diagnosis?
ECG localization: Which ST-elevation leads indicate an inferior myocardial infarction and which indicate right ventricular involvement?
Hemodynamics: What does a laterally displaced point of maximal impulse and clear lungs suggest in this patient?
Central venous pressure: What CVP value is recorded and is it within normal range?
Management anchor: For right ventricular infarction causing cardiogenic shock, what is the most appropriate initial step?
Why is IV furosemide incorrect as initial therapy for right ventricular infarction with hypotension?
When is IV dobutamine appropriate in cardiogenic shock from right ventricular infarction?
Why is IV propranolol contraindicated acutely in this hypotensive STEMI patient?
Initial STEMI care bundle (besides fluids for RV infarct): Which immediate therapies should be given?
Why is pulmonary artery catheterization listed as an incorrect initial step in this scenario?
Illustration: ECG pattern of inferior STEMI with right ventricular involvement — what leads to check for right ventricular ST elevation? (see image)
ST-elevation myocardial infarction (STEMI): what is its urgency and classic acute presentation?
STEMI: what happens to troponin levels?
STEMI: what ECG finding confirms localization?
STEMI: what is the definitive treatment?
Right ventricular (RV) infarction: what major hemodynamic complication can occur?
Right ventricular infarction: how does preload status affect initial stabilization?
Administration of propranolol in a hypotensive patient: likely effect on cardiac output and blood pressure?
Pulmonary artery catheterization (PAC): when is PAC appropriate in shock?
Pulmonary artery catheterization: why is PAC inappropriate when the shock cause is clear?
Isoimmunization to the Kell erythrocyte antibody: strongest predisposing risk factor in this patient?
Why is prior blood transfusion the strongest risk factor for Kell isoimmunization?
Pathophysiology: how do maternal anti-Kell antibodies affect the fetus?
How to determine fetal risk for Kell-related hemolysis when mother is anti-Kell positive?
When is previous spontaneous abortion a significant risk for RBC isoimmunization?
Why does maternal ABO blood group not increase risk for Kell isoimmunization?
Does Rho(D) immune globulin (RhoGAM) prevent Kell isoimmunization?
Is threatened abortion a strong risk factor for Kell isoimmunization?
Comparison: blood transfusion vs spontaneous abortion as sources of maternal alloimmunization
Clinical step: how to assess fetal Kell antigen status when mother is anti-Kell positive (illustration)?
Rh(D) immune globulin: What is the mechanism preventing maternal alloimmunization?
Rh(D) immune globulin: Does it prevent maternal antibodies to Kell antigens?
Threatened abortion: What is the clinical definition?
Threatened abortion: How does it affect risk of fetal erythrocyte isoimmunization?
Maternal alloimmunization: What exposures can lead to antibody formation?
Alloimmunization risk: What determines likelihood of maternal isoimmunization?
Fetal consequences: What are major risks from maternal red blood cell alloimmunization?
When would threatened abortion be the primary concern for isoimmunization risk?
Alloimmunization overview: What summary rule links exposures and fetal risk?
Illustration: What are the key fetal risks from maternal alloimmunization? (see image)
Clinical decision: Safe discharge planning for a 92-year-old with acute confusion and poor memory — what is the primary priority?
Clinical finding: 92-year-old with zero of three-word recall after 5 minutes — what does this suggest about capacity?
Management decision: When is involving social services indicated in discharge planning?
Correct answer rationale: Why is 'arrange placement in a supervised living facility' appropriate here?
Option 'Bioethics: futile medical treatment' — when would this be appropriate?
Why is 'palliative care to discuss end-of-life planning' NOT appropriate for this patient now?
When would 'psychiatry to address an advance directive' be appropriate?
Why is 'volunteer canine therapy' insufficient as the next step in discharge planning?
Clinical anchor: Features of this patient's acute presentation that indicate delirium rather than chronic dementia
Illustration: Slide showing highlighted discharge-planning teaching point — what role does social services play?
Discharge planning: When are social services likely required for a patient?
Discharge planning: What is the benefit of early social services involvement in the clinical course?
Define amaurosis fugax (clinical anchor).
Describe Hollenhorst plaque appearance and typical location (retinal finding).
Primary source of emboli causing Hollenhorst plaques (diagnostic anchor).
Most appropriate next diagnostic step for amaurosis fugax with Hollenhorst plaque (clinical decision).
When is echocardiography the preferred test for suspected retinal embolic source (choice C context)?
When is cerebral MR angiography or brain MRI useful vs retinal embolic disease (choice B/E context)?
Role of intraocular pressure measurement in acute vision loss workup (choice D context).
How can treating carotid or cardiac valvular disease affect retinal/cerebral outcomes (management anchor)?
Fundus photo: what finding supports carotid-source cholesterol embolus? (use image on answer for illustration)
Amaurosis fugax: defining clinical feature?
Hollenhorst plaque: description
Amaurosis fugax: immediate diagnostic study
Glaucoma: typical clinical course and key sign
Why glaucoma is unlikely for brief transient vision-loss episodes?
Serum antinuclear antibody (ANA) assay: appropriate use
Autoimmune vasculitis causing retinal/ophthalmic ischemia: typical vision-loss pattern
Giant cell arteritis (GCA): relation to amaurosis fugax and testing
Amaurosis fugax management: source most commonly evaluated where?
Fundus finding and embolus correlation (visual aid)
What is the most likely diagnosis for a 47-year-old with 3 months of weight loss, epigastric fullness, painless hyperbilirubinemia, mild ALP/AST/ALT elevation, and 30-year smoking history?
Which imaging is most appropriate to evaluate suspected pancreatic cancer?
Why is CT abdomen with contrast preferred for suspected pancreatic cancer?
What laboratory pattern indicates cholestasis in this case?
Which clinical features are classic for pancreatic head carcinoma?
What is the best curative treatment option for localized pancreatic cancer?
When is a bone scan appropriate in oncology?
When are flat and upright abdominal x-rays useful?
When is a HIDA scan indicated?
Which risk factors for pancreatic cancer are listed in the case text?
Pancreatic cancer: classic clinical presentation?
Pancreatic cancer: characteristic laboratory finding indicating cholestasis?
Pancreatic cancer: common risk factors?
Pancreatic cancer: initial imaging of choice when suspected?
Pancreatic cancer: definitive/curative treatment option?
Right upper quadrant ultrasonography: primary clinical use?
Right upper quadrant ultrasonography: when might it show an enlarged gallbladder in pancreatic disease?
Mild alkaline phosphatase, ALT, AST elevations in suspected pancreatic cancer: next best diagnostic step?
Choice E (RUQ ultrasonography) vs CT abdomen with contrast: when is CT preferred?
Right upper quadrant ultrasonography: when is RUQ US the correct initial test?
Define heat stroke (core features)
Distinguish heat stroke from heat exhaustion
Primary pathophysiology of heat stroke causing organ injury
Laboratory abnormalities associated with heat stroke
Initial management priorities for heat stroke
Why is evaporative cooling the correct immediate therapy for environmental heat stroke?
When is CT scan of the head appropriate in altered mental status?
When is norepinephrine indicated for hypotension in heat stroke?
When is dantrolene the correct therapy (contrast with heat stroke)?
When is lumbar puncture appropriate in altered mental status?
Cooling methods for heat stroke (examples)
Supportive steps during cooling for heat stroke (monitoring)
Illustration: evaporative cooling slide (supplement)
Heat stroke: core definition and immediate pathophysiology?
Heat stroke: cardinal vital-sign and systemic features?
Heat stroke: major complications to anticipate?
Heat stroke: initial management priorities?
Bacterial meningitis: typical presenting symptoms?
Cerebrospinal fluid (CSF) profile in bacterial meningitis?
Lumbar puncture (LP): when is it useful?
Clinical distinction: heat stroke vs bacterial meningitis—key discriminating history?
Why LP is less appropriate for patient with hyperthermia after heat exposure?
Heat stroke: monitoring and support measures during treatment (supplemental image)?
Phentermine: mechanism causing hypertension?
Hypertensive emergency: diagnostic threshold and requirement?
Common presenting symptoms of sympathomimetic-induced hypertensive emergency?
Clinical features in the presented 15-year-old phentermine overdose case?
Sodium nitroprusside: clinical role in sympathomimetic hypertensive emergency?
Sodium nitroprusside: described mechanism of action (as stated)?
Phentolamine: role in sympathomimetic hypertensive emergency?
Intravenous calcium: correct clinical uses?
IV furosemide: when is it appropriate for hypertension?
IV phenytoin: appropriate emergent indications?
IV physostigmine: correct emergent indication?
IV verapamil: contraindication present in this case?
Endotracheal intubation: indications relevant to this patient?
Comparison: sodium nitroprusside versus verapamil in this overdose scenario?
Sodium nitroprusside: illustration of use (slide image)?
Intravenous sodium nitroprusside: primary vascular mechanism?
Phentermine: which vascular effect is counteracted by intravenous sodium nitroprusside?
Atrial septal defect (ASD): key auscultatory findings?
Atrial septal defect (ASD): primary pathophysiology?
Why does ASD cause a fixed, widely split S2?
Uncorrected ASD: most important long-term complication?
Why is pulmonary hypertension the correct long-term risk in ASD?
Cholestasis: typical cause and presentation?
Why is cholestasis unlikely in this young woman with ASD?
Budd-Chiari syndrome (hepatic vein thrombosis): common risk factors?
Why is Budd-Chiari unlikely in this patient despite OCP use?
Hepatitis: common causes and presentation?
Why is acute hepatitis unlikely in this patient?
Renovascular hypertension from fibromuscular dysplasia: typical patient and exam?
Why is renovascular hypertension unlikely in this patient?
Primary (systemic) hypertension: common risk factors?
Why is systemic hypertension unlikely in this 22-year-old woman?
Eisenmenger syndrome: defining features and consequence?
Midsystolic ejection murmur in ASD: mechanism?
ASD subtypes: commonest type and association with ostium primum?
Illustration: ASD pathophysiology and auscultation (supplemental image)
Atrial septal defect (ASD): primary pathophysiologic effect on the pulmonic valve?
Atrial septal defect (ASD): most common anatomic type?
Atrial septal defect (ASD): which defect type is commonly associated with Down syndrome?
Atrial septal defect (ASD): severe complication from long-standing uncorrected defect?
Bacterial vaginosis: defining clinical features in adolescent with vaginal discharge
Bacterial vaginosis: primary pathophysiology and common organism
Clue cells: microscopic definition
Bacterial vaginosis: diagnostic lab findings
Bacterial vaginosis: first-line treatment and routes
Bacterial vaginosis: sexual transmission and partner treatment policy
Antibiotic exposure: role in bacterial vaginosis development
Chemical irritation (bubble baths): typical genital findings vs discharge
Latex allergy (condom): typical genital findings vs vaginal discharge
Physiologic vaginal secretions: distinguishing features from pathologic discharge
Trichomoniasis: typical clinical features differentiating from BV
Comparison: BV versus Trichomonas key distinguishing points
Bacterial vaginosis: supportive image of wet mount (clue cells)
Bacterial vaginosis: what organism causes the condition?
Bacterial vaginosis: describe the typical vaginal discharge.
Bacterial vaginosis: what is the typical vaginal pH?
Bacterial vaginosis: what is the potassium hydroxide (KOH) finding?
Bacterial vaginosis: what microscopic finding confirms the diagnosis?
Bacterial vaginosis: what is the first-line treatment?
Bacterial vaginosis: is it considered a sexually transmitted infection (STI)?
Bacterial vaginosis: are protozoan infections likely causes?
What is pubertal gynecomastia?
What pathophysiologic mechanism causes pubertal gynecomastia?
Typical physical exam features of pubertal gynecomastia?
What is the expected result of laboratory studies in physiologic pubertal gynecomastia?
Management of physiologic pubertal gynecomastia in an otherwise healthy adolescent?
Why is 'Puberty' the most likely cause of the 14-year-old boy's breast swelling?
When would SSRI-associated gynecomastia be the correct diagnosis?
How does male breast cancer usually differ on exam from benign gynecomastia?
When is marijuana a likely cause of gynecomastia and by what proposed mechanism?
Which clinical features suggest Klinefelter syndrome (seminiferous tubule dysgenesis) rather than pubertal gynecomastia?
Physical exam illustration: subareolar tender breast mass — what diagnosis does this support?
Anchor: Initial diagnostic step for 47-year-old with 6-month progressive low back pain without neurologic deficits or red flags?
Anchor: Pathophysiology components of degenerative disc disease?
Anchor: Mechanism causing loss of disc height in degenerative disc disease?
Anchor: How do annulus fibrosus tears develop in degenerative disc disease?
Anchor: Sensory innervation of annulus fibrosus periphery?
Anchor: Typical pain features of degenerative disc disease?
Anchor: Physical exam tests and signs to evaluate for radiculopathy?
Anchor: Red-flag features indicating possible cauda equina or conus medullaris syndrome requiring emergent surgery?
Anchor: Indication for MRI of the lumbar spine in low back pain?
Anchor: Appropriate use of bone scan in back pain?
Anchor: Role of CT myelography versus MRI in spine imaging?
Anchor: Conservative treatments for degenerative disc disease?
Anchor: When to obtain initial imaging for low back pain?
Anchor: Supplementary slide showing recommended initial test for chronic low back pain (image on answer)
Cauda equina compression: core presenting features?
Cauda equina compression: common acute causes?
Initial imaging for suspected lumbar spine problem without neurologic deficits?
Role of MRI in acute lumbosacral compression when initial exam lacks deficits?
Degenerative disc disease: primary pathophysiologic processes?
Degenerative disc disease: how annulus fibrosus tears form?
Degenerative disc disease: typical symptom triggers?
Degenerative disc disease: first-line nonprocedural treatments (group 1)?
Degenerative disc disease: first-line nonprocedural treatments (group 2)?
Imaging workflow for patient with lumbar complaint and no neurologic deficits: concise plan?
Supplemental image: presentation slide relevant to lumbar imaging and degenerative disc disease?
Membranous nephropathy: core nephrotic syndrome features?
Membranous nephropathy: key biopsy/immunofluorescence findings?
Membranous nephropathy: common secondary associations?
Pathophysiology: why hypercholesterolemia occurs in nephrotic syndrome?
ACE inhibitor therapy: mechanism slowing progression of membranous nephropathy?
Why is ACE inhibitor (eg, lisinopril) the correct choice for delaying renal progression in membranous nephropathy?
High-protein diet: when would it be appropriate in kidney disease?
High-potassium diet: when is it indicated in kidney disease?
Beta-blocker therapy (eg, metoprolol): when would it be preferred over ACE inhibitor for renal protection?
Diuretic therapy: appropriate indication in membranous nephropathy?
Membranous nephropathy: summary preventive treatment principle for slowing progression?
Visual: membranous nephropathy features (illustration). What biopsy features are shown?
Osteoporosis trial result: what does a P-value of 0.047 indicate about chance?
Osteoporosis trial: how large was the absolute reduction in hip-fracture rate?
Why is the trial result statistically significant but not clinically significant?
When would 'results likely caused by chance' be a correct conclusion?
Definition: placebo effect as described in the trial explanation
When could the placebo effect explain a trial difference?
Why is 'inadequate power' unlikely for this osteoporosis trial?
What does 'clinical significance' require beyond statistical significance?
Applicability: what does 'applicability' mean for a treatment effect?
Applicability: main factors that can affect whether study results apply to non-study patients?
Applicability example: elderly patient with osteoporosis on calcium and vitamin D — are study results likely applicable?
Statistical power: what does 'power' describe?
Factors that may influence statistical power (small list)?
When is 'inadequate power' a correct explanation for study findings?
Why is 'inadequate power' an incorrect explanation if the study was adequately powered?
What does a conventional P-value cutoff of 0.05 indicate?
How does statistical significance (P≤0.05) differ from clinical significance?
Study statement: Can power change the magnitude of an observed treatment effect?
Visual: slide illustrating highlighted teaching points (useful as summary)
Define 'hematogenous osteomyelitis' in children (anchor: osteomyelitis presentation).
Key clinical features of pediatric hematogenous osteomyelitis (anchor: clinical presentation).
Laboratory and imaging findings supporting osteomyelitis (anchor: diagnostics).
Most likely pathogen for hematogenous osteomyelitis in this 2-year-old (anchor: microbiology).
Gram-stain clue pointing to Staphylococcus aureus (anchor: Gram stain interpretation).
First-line initial antibiotic choice for suspected MRSA/MSSA pediatric osteomyelitis (anchor: initial management).
Why ampicillin is inappropriate as initial monotherapy here (anchor: ampicillin limitation).
When would azithromycin be an appropriate choice (anchor: azithromycin spectrum)?
Rationale for starting broad-spectrum therapy in suspected pediatric osteomyelitis (anchor: treatment principle).
Other common pediatric osteomyelitis pathogens besides S. aureus (anchor: differential microbiology).
Why ceftriaxone/cefepime/rifampin were not chosen as initial therapy in this case (anchor: initial-choice logic).
Osteomyelitis (pediatric): definition
Osteomyelitis (pediatric): most common causative bacterium
Osteomyelitis (pediatric): other common bacteria (group 1)
Osteomyelitis (pediatric): other common bacteria (group 2)
Initial antibiotic choice for suspected pediatric osteomyelitis with possible MRSA
Why ceftriaxone or cefepime alone is NOT initial monotherapy for suspected MRSA osteomyelitis
When is cefepime specifically useful in bone infection coverage?
Role of combining vancomycin with ceftriaxone/cefepime in osteomyelitis
Azithromycin in suspected MRSA osteomyelitis: appropriateness
Rifampin: mechanism and limits relevant to osteomyelitis
Pathogenesis anchor: how pediatric osteomyelitis usually arises
Supplementary: slide image for osteomyelitis teaching (illustration only)
Rheumatic mitral valve disease: what is the pathophysiology linking group A strep to progressive valve damage?
Rheumatic fever: key extra-cardiac clinical findings
Rheumatic mitral valve disease: typical acute vs chronic valve dysfunction
Mitral stenosis: classic auscultatory and complication features
Why rheumatic mitral valve disease best explains this patient: 32-year-old with 6 months dyspnea, irregular tachycardia, holosystolic murmur and diastolic rumble at apex, AF, RVH?
Aortic stenosis from calcified tricuspid aortic valve: when is this the usual cause and typical findings?
Bicuspid aortic valve calcification: typical patient group and mechanism
Atrial septal defect (ASD): hemodynamic effects and auscultatory clues when ASD is the correct diagnosis
Ventricular septal defect (VSD): classic murmur and typical location heard
Infective endocarditis (Staphylococcus aureus or viridans): typical presenting features that support this diagnosis
Slide image: supporting visual summary of exam item (use as reference only)
Diagnosis: Mitral valve calcification — what valvular lesion can this cause?
Mitral stenosis — classic auscultatory findings?
Cause: Long-term complication that classically produces mitral stenosis?
Complications of severe mitral stenosis?
Why is infective endocarditis unlikely for a patient with 6 months of symptoms?
When would endomyocarditis/myocarditis be the correct diagnosis?
Why is pericarditis an unlikely diagnosis for this patient?
Pericarditis — common causes and ECG pattern?
Illustration: slide with highlighted teaching points — what image shows?
Knee injury randomized trial with 500 randomized to operative (400 received) and 500 randomized to conventional (50 received): What is the primary study-design concern?
Definition: What is intention-to-treat (ITT) analysis?
Per-protocol analysis: how does it differ from ITT?
Why is lack of ITT analysis problematic in the knee trial described?
When would 'Inadequate randomization' be the correct concern in a trial?
When is 'Inappropriate control group' (placebo) the correct concern?
When is 'Short follow-up duration' a valid trial concern?
Is 'Small sample size' the primary problem in the described knee trial?
Study design: What is the effect of a 'small sample size' on statistical power?
Clinical trial: Name baseline factors that influence statistical power (grouped).
Clinical trial: Name treatment-related factors that influence statistical power (grouped).
Study planning: Is enrolling 1000 participants generally adequate for statistical power?
Intention-to-treat (ITT): What is the ITT analysis rule for randomized subjects?
ITT rationale: What is the consequence of excluding randomized subjects from analysis?
ITT benefit: What biases does ITT help limit and what integrity does it preserve?
Intention-to-treat (ITT): Illustrative slide (supporting image on answer side).
Anchor: Oncology unit medication errors — what root cause was identified?
Anchor: Correct intervention to prevent look-alike vial errors in oncology unit?
Anchor: Why is repackaging distinct containers the best fix for repeated look-alike medication errors?
Anchor: Root cause analysis (RCA) — concise definition?
Anchor: Staff interviews — role in RCA?
Anchor: Option B ('Remove the antibiotic from formulary') — why is this incorrect here?
Anchor: Option C ('Require continuing education for nurses') — when would this be appropriate?
Anchor: Option D ('Suspend nurses involved') — why is suspension incorrect here?
Anchor: Option E ('No intervention likely helpful') — why is this incorrect here?
Anchor: Common predictable cause of medication errors — what is it?
Anchor: Example of a targeted corrective action for look-alike vials — what might be done by pharmacy?
Squamous cell carcinoma of the lung: key paraneoplastic metabolic abnormality?
Squamous cell carcinoma of the lung: typical gross/clinic location and radiographic feature?
Squamous cell carcinoma histology: characteristic findings?
Clinical presentation common to primary lung cancer?
Diagnosis confirmation for a suspected lung mass?
Why squamous cell carcinoma is the correct diagnosis for a 3-cm central lung mass with hypercalcemia in a long-term smoker?
Adenocarcinoma of the lung: typical patient profile and location?
Adenocarcinoma histology distinguishing feature?
Large cell carcinoma of the lung: defining histology and typical location?
Small cell carcinoma of the lung: cell type and distinguishing paraneoplastic syndromes?
Small cell carcinoma histology distinctive microscopic appearance?
Melanoma: typical primary lesion features and common metastatic sites?
Imaging/biopsy illustration for confirming lung cancer diagnosis (supplementary image)?
Which primary lung cancers are typically centrally located?
Which centrally located lung cancer is the more common subtype?
What paraneoplastic syndrome is associated with squamous cell carcinoma of the lung?
How is diagnosis of a primary lung cancer confirmed?
What determines prognosis in primary lung cancer?
What is the typical timing of detection and its impact on prognosis for primary lung cancer?
Diagnostic illustration for primary lung cancer (supplementary): what imaging and tissue test are used?
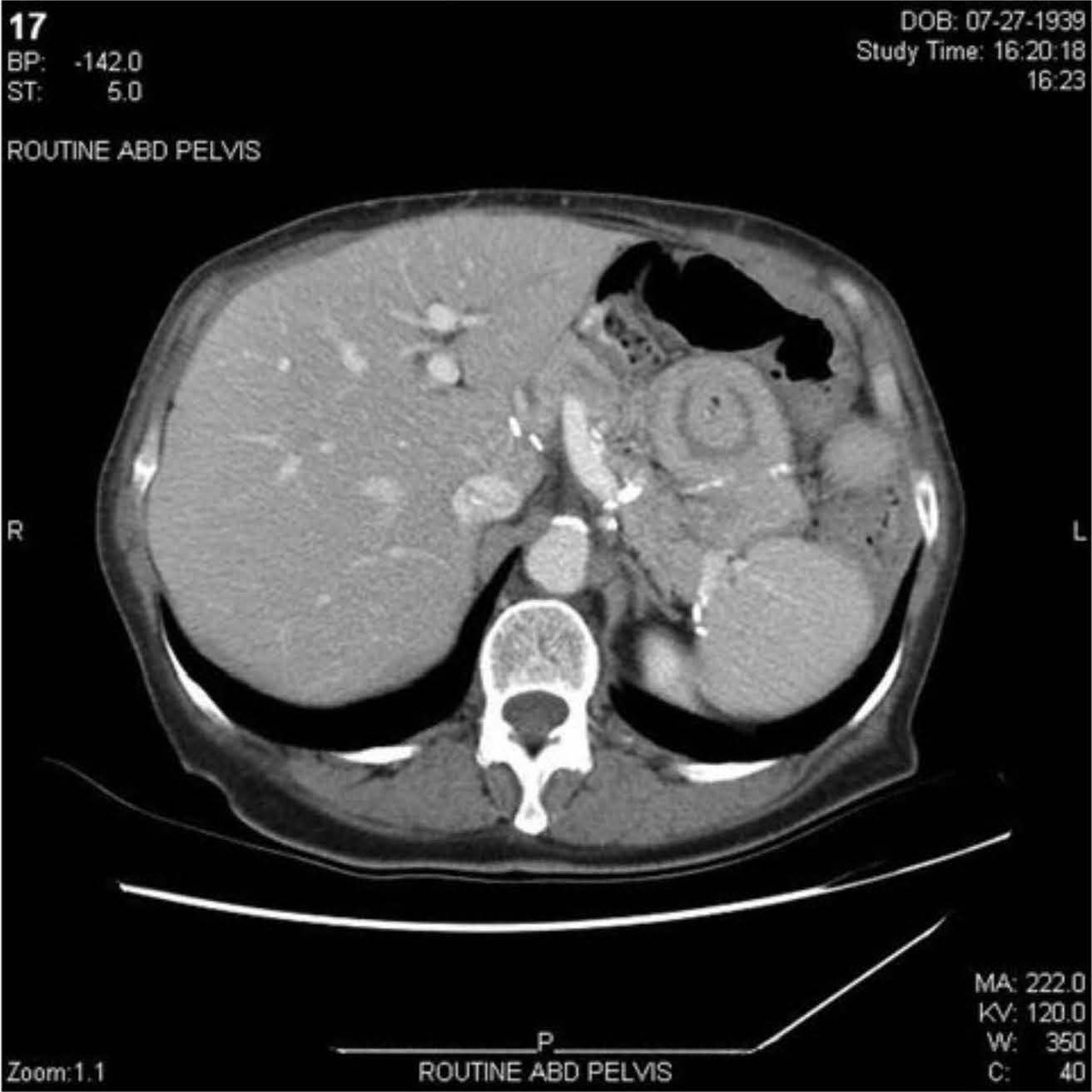
Diagnosis: 62-year-old with 2 days nausea, severe abdominal pain, prior partial gastrectomy; CT shows target sign: what is the most likely diagnosis?
Pathophysiology: What causes intussusception? (anchor: intussusception)
Intussusception lead points: Name common pathologic lead points that precipitate intussusception.
Clinical features: What are typical symptoms of intussusception in adults? (anchor: intussusception symptoms)
Imaging: What CT/US signs confirm intussusception? (anchor: intussusception imaging)
Management: How does adult intussusception treatment differ from pediatric? (anchor: intussusception management)
When is bacterial small-bowel overgrowth the correct diagnosis? (anchor: bacterial overgrowth features)
When is intestinal volvulus the correct diagnosis? (anchor: volvulus features)
When is jejunal enteritis the correct diagnosis? (anchor: jejunal enteritis features)
When are small-bowel adhesions the correct diagnosis? (anchor: small-bowel adhesions features)
Differentiation: How to distinguish intussusception from small-bowel adhesions on CT? (anchor: imaging differentiation)
Clinical context: Why could prior partial gastrectomy predispose an adult to intussusception? (anchor: postop risk)
Small bowel obstruction (SBO): key presenting symptoms?
CT findings that typically indicate SBO?
Why does absence of dilated small bowel loops on CT argue against SBO?
Management of partial uncomplicated SBO?
Management required for complete or complicated SBO?
Intussusception: pathophysiology (anchor: Intussusception)?
Intussusception: classic clinical features?
Imaging signs of intussusception on CT or ultrasound?
Clinical decision: When would exploratory laparotomy be indicated for bowel obstruction?
Interpretation task: Does this CT image support SBO? (anchor: CT abdomen)
CT example (anchor: CT abdomen image): view the image for landmarks relevant to obstruction.
Anaphylaxis: core pathophysiology?
Anaphylaxis: most common triggers mentioned?
Anaphylaxis: organ systems commonly affected?
Anaphylaxis: key presenting symptoms from each system (short)?
Stridor in anaphylaxis: clinical significance?
Initial management of anaphylaxis with hypotension, urticaria, stridor?
Why is epinephrine the first treatment in anaphylaxis?
Role of antihistamines in anaphylaxis?
Role of IV fluids in anaphylaxis?
When is endotracheal intubation indicated in anaphylaxis?
Risks/considerations for intubation in anaphylaxis?
Correct answer justification: why 'administration of epinephrine' is preferred over hospital admission alone?
When would antihistamine alone be appropriate for allergic reaction?
Use of the provided image as illustration for airway edema?
What is the pathophysiology of anaphylaxis?
What are the main respiratory features of anaphylaxis?
What are the main cutaneous/oral features of anaphylaxis?
What are the main gastrointestinal and hemodynamic features of anaphylaxis?
What is the first-line urgent treatment for anaphylaxis?
What are the next immediate adjunct treatments after epinephrine in anaphylaxis (group 1)?
What supportive measure is given after epinephrine and adjunct medications in anaphylaxis (group 2)?
Describe a concise treatment sequence for anaphylaxis.
Diagnosis: Which eating disorder fits a 24-year-old with weekly binge eating and daily laxative purging, BMI 21, no vomiting?
Pathophysiology: How does chronic laxative overuse cause metabolic acidosis?
Pathophysiology: Mechanisms producing hypokalemia with chronic laxative abuse?
Clinical feature: What orthostatic vital sign changes indicate hypovolemia in this patient?
Diagnostics: Which laboratory pattern matches laxative-induced metabolic acidosis with hypokalemia (correct answer choice)?
Why choice A would be correct: When does hyperkalemia with metabolic acidosis and respiratory compensation occur?
Why choice B would be correct: When does hypokalemia with metabolic alkalosis occur?
Why choice D is incorrect: What does normal serum K+ and normal pH indicate?
Why choice E would be correct: When is respiratory alkalosis with near-normal K+ seen?
Management: Immediate treatment priorities for bulimia nervosa with laxative-induced hypovolemia/hypokalemia?
Diagnostic distinction: How to differentiate laxative-induced acid-base disorder from vomiting-induced disorder?
Supplementary: Slide illustrating teaching points about laxative abuse and labs (image on answer side).
Disease: Bulimia nervosa — core behavioral features?
Anchor: Laxative overuse — primary electrolyte losses?
Anchor: Laxative overuse — typical acid–base disturbance?
Anchor: Laxative-induced hypokalemia — link to acid–base status?
Anchor: Laxative overuse — effect on respiration?
Anchor: Laboratory pattern suggesting laxative abuse in bulimia?
Anchor: Vomiting vs laxative overuse — distinguishing acid–base effects?
Anchor: Compensatory purging options in bulimia (three main)?
Anchor: Image — visual slide of highlighted teaching point (supplement)
Gentamicin: primary nephrotoxicity prevention measure when given IV for sepsis/UTI?
Gentamicin: mechanism of synergy with beta-lactams (eg, piperacillin-tazobactam)?
Gentamicin: major toxicities relevant to a 67-year-old with sepsis?
Trough concentration: timing and meaning for aminoglycoside dosing?
Initial management of septic UTI with hypotension and CVA tenderness?
Central venous pressure (CVP) measurement: when is it used clinically?
CVP measurement: when would CVP likely be decreased?
Piperacillin-tazobactam: role in urosepsis and nephrotoxicity risk?
When is discontinuation of piperacillin-tazobactam appropriate in sepsis?
Bicarbonate therapy: appropriate indication in septic patient?
Low-dose dopamine: typical clinical use compared with norepinephrine?
Why measuring gentamicin trough is correct choice to reduce acute renal failure risk?
Image: Urosepsis with right CVA tenderness — which supportive therapy is essential before vasopressors?
Gentamicin: primary serious organ toxicity?
Gentamicin: clinical purpose of measuring trough concentration?
Screening: Which preventive test is most appropriate now for a 47-year-old obese woman (BMI 33) to detect type 2 diabetes?
Rationale: Why screen for diabetes in adults aged 35–70 who are overweight/obese?
Pap smear: When is cervical cancer screening recommended for a 47-year-old woman with prior normal Pap smears?
DEXA scan: When is osteoporosis screening indicated instead of now for this 47-year-old premenopausal woman?
ECG screening: When is a resting ECG the most appropriate screening test in asymptomatic adults like this patient?
Mammography: What is the recommended screening interval relevant to a 47-year-old woman?
Comparison: Why is fasting glucose/A1c preferred now over Pap smear, DEXA, ECG, or mammography for this patient?
Guidelines summary: Which two screening categories encompass most adult preventive recommendations mentioned?
Illustration: Where to find recommended screening example for overweight 35–70-year-olds (image)?
Baseline ECG screening: When is an ECG indicated?
Baseline ECG screening in asymptomatic adults: why is it not recommended?
When is screening mammography routinely recommended by USPSTF?
Breast cancer screening for patients aged 40–49 years: what is the recommendation?
Why is mammography every 3 years incorrect for a 47-year-old patient?
Screening for type 2 diabetes mellitus: which patients should be screened?
Preventive care screening decisions: what factors determine recommendations?
Illustration: Which screening topic is highlighted in the slide?
Restless legs syndrome (RLS): core diagnostic features?
RLS: common associated pathophysiology mentioned?
Role of serum ferritin in RLS diagnosis?
Iron supplementation in RLS: when recommended?
First-line treatments for RLS?
Why measurement of serum ferritin was the most appropriate next diagnostic step in this 47-year-old with bilateral leg restlessness?
When is Doppler ultrasonography of lower extremities appropriate (vs RLS)?
When is EEG appropriate for nocturnal symptoms (vs RLS)?
When is fasting serum glucose useful for leg symptoms (vs RLS)?
Why 'no further testing' is incorrect for this patient?
Distinguishing feature: RLS vs peripheral arterial disease (PAD)?
Distinguishing feature: RLS vs deep vein thrombosis (DVT)?
Distinguishing feature: RLS vs diabetic peripheral neuropathy?
Use of provided image as supplementary material for RLS education
Scaphoid fracture: typical mechanism and common location
Scaphoid fracture: presenting exam findings
Scaphoid blood supply relevance to complications
Most likely complication of scaphoid fracture
Initial imaging and next step if x-ray unremarkable but suspicion remains
Nondisplaced scaphoid fracture: usual management
Displaced scaphoid fracture: management consideration
When is distal fat embolus expected after orthopedic trauma?
Osteomyelitis: diagnostic features distinguishing it from simple fracture
Malunion of scaphoid fracture: expected consequence
Wrist fusion in scaphoid disease: when considered
Use of the provided image for scaphoid fracture learning
Scaphoid fracture: most likely mechanism of injury?
Scaphoid blood supply and clinical consequence?
Scaphoid fracture: management for nondisplaced fractures?
Scaphoid fracture: indications for surgical intervention?
Scaphoid fracture: why proximal pole fractures favor surgery?
Karteikarten in diesem Deck (813)
-
Clinical decision: 90-year-old woman with open tibial fracture refuses surgical stabilization but accepts irrigation/debridement and antibiotics. What is the next step?
- Assess decision-making capacity
internal surgery psychiatry step2. -
Definition: What are the four criteria for medical decisional capacity?
- Consistent choice
- Understanding risks/benefits
- Understanding personal significance
- Reasoning through options
psychiatry internal step2. -
Principle: Is decisional capacity global or decision-specific?
- Decision-specific; capacity must be assessed for each decision
psychiatry internal step2. -
Legal distinction: Who determines a patient's global competence?
- Courts determine competence; physicians assess decision-specific capacity
psychiatry internal step2. -
When is discussing the case with a durable power of attorney (son) appropriate?
- If patient lacks decision-making capacity, then defer decision to durable POA
internal surgery step2. -
When is petitioning the court to appoint a guardian appropriate for a patient with incapacity?
- Only if permanently incapacitated AND no surrogate decision maker (eg, no durable POA or next of kin)
internal psychiatry step2. -
When is proceeding with recommended surgical treatment despite patient refusal justified?
- Not justified here; proceeding would violate autonomy. First assess capacity; if lacks capacity, involve durable POA rather than proceed
surgery internal ethics step2. -
When is using cast immobilization to honor a refusal appropriate for this open tibial fracture?
- Premature; if patient has capacity, abide by her refusal; if lacks capacity, decision goes to durable POA
surgery internal step2. -
Practical: How should a clinician assess the 90-year-old patient's decisional capacity for refusing surgery?
- Discuss fracture care preferences and evaluate the four capacity criteria
Answer includes image:
 internal surgery psychiatry step2.
internal surgery psychiatry step2. -
Decisional capacity assessment: who must assess it?
- Physician must assess patient's decisional capacity
internal step2. -
psychiatry step2.
-
Decisional capacity and demographics: when should assessment be done relative to age or cognitive status?
- Regardless of patient age or cognitive ability, assess capacity
neurology step2. -
Decisional capacity: concise rule combining actor, timing, and scope
- Physician assesses decisional capacity for each specific care decision, regardless of patient age or cognitive ability
internal psychiatry step2. -
Anchor: Initial step for asymptomatic elevated blood pressure (140/100) in 21-year-old
Repeat blood pressure measurements: confirm with in-office and/or at-home serial readings over weeks to months before diagnosing hypertension.
internalmedicine step2. -
Anchor: Why no additional diagnostic studies now for isolated elevated BP in asymptomatic patient
One isolated elevated reading does not diagnose hypertension; confirmation with repeat measurements required before further testing.
internalmedicine step2. -
Anchor: Primary determinants of blood pressure (3 systems)
- Renin-angiotensin-aldosterone system
- Sympathetic nervous system
- Plasma blood volume
internalmedicine step2. -
Anchor: Risk factors contributing to primary (essential) hypertension
- Advancing age
- Obesity / sedentary lifestyle
- Smoking, high-sodium diet, excess alcohol, insufficient sleep, genetics
internalmedicine step2. -
Anchor: When to measure serum aldosterone:renin ratio (hyperaldosteronism workup)
Use when secondary hypertension suspected with hypokalemia or metabolic alkalosis suggesting excess aldosterone.
internalmedicine step2. -
Anchor: Why aldosterone:renin ratio is unlikely in this patient
Patient has normal serum electrolytes (no hypokalemia) making hyperaldosteronism unlikely.
internalmedicine step2. -
Anchor: When to evaluate renal artery stenosis (renal Doppler/arteriography)
Suspect when resistant hypertension requiring multiple agents or abdominal bruit; more common from atherosclerosis (older) or fibromuscular dysplasia (younger).
internalmedicine step2. -
Anchor: Why renal artery imaging is inappropriate now for this patient
No resistant hypertension, no abdominal bruit, and patient is young without features pointing to renal artery stenosis.
internalmedicine step2. -
Anchor: Role of renal CT scan in hypertension evaluation
Not routine; may show atrophic kidneys with renal artery stenosis or used for pyelonephritis/abscess when fever, flank pain, dysuria present.
internalmedicine step2. -
Anchor: Next steps if hypertension is confirmed
Evaluate for end-organ damage and discuss lifestyle modification and antihypertensive therapy with primary care.
internalmedicine step2. -
Anchor: Educational point: long-term risks of untreated hypertension
- Heart failure
- Ischemic/hemorrhagic stroke
- Chronic kidney disease
internalmedicine step2. -
Anchor: Image: slide with highlighted text (supplemental)
Supplementary image:
 Use image only as illustration of exam explanation.internalmedicine step2.
Use image only as illustration of exam explanation.internalmedicine step2. -
internal_medicine step2.
-
internal_medicine step2.
-
Primary hypertension: major long-term complications if untreated?
- Heart failure
- Ischemic and hemorrhagic stroke
- Chronic kidney disease
internal_medicine step2. -
Primary hypertension: does a single elevated BP reading establish diagnosis?
- No. One isolated elevated BP in an asymptomatic patient does not indicate hypertension
internal_medicine step2. -
Primary hypertension: acceptable methods to confirm elevated BP before diagnosis?
- Both in-office and at-home measurements
- Or serial in-office measurements over weeks–months
internal_medicine step2. -
Primary hypertension: recommended timing for serial in-office BP measurements to confirm diagnosis?
- Over a period of weeks to months
internal_medicine step2. -
Clinical decision: 18-year-old post-blunt chest trauma with left pleural effusion, tachycardia, tachypnea, rising O2 needs — most appropriate immediate management?
- Tube thoracostomy
surgery step2. -
Pathophysiology: What causes traumatic hemothorax?
- Blood in pleural space from pulmonary, bronchial, or intercostal vessel injury (eg, rib fractures)
internal_medicine step2. -
Presentation: Key clinical features of hemothorax?
- Chest pain, shortness of breath, dullness to percussion, decreased breath sounds on affected side
emergency step2. -
Definition: When is hemothorax classified as massive?
- Initial chest-tube output >1000–1500 mL or >200 mL/hr for ≥4 hr
surgery step2. -
Management decision: Purpose of initial tube thoracostomy in traumatic hemothorax?
- Promote lung expansion; exclude ongoing hemorrhage; prevent residual pneumothorax, empyema, fibrothorax, fistula
surgery step2. -
When is video-assisted thoracoscopy (VATS) or thoracotomy indicated in hemothorax?
- If massive hemothorax (see criteria) or ongoing high-volume drainage after chest tube
surgery step2. -
Ultrasonography role in blunt chest trauma with effusion: when is it appropriate?
- Useful for initial detection of pleural fluid and to guide thoracentesis, but unnecessary if CXR already shows effusion and urgent tube needed
pediatrics step2. -
CT chest role in traumatic hemothorax: when is CT appropriate?
- Characterizes injuries further (eg, vascular, parenchymal) but defer if patient needs immediate chest-tube intervention
radiology step2. -
Thoracentesis in traumatic pleural effusion: when is thoracentesis appropriate?
- Diagnostic/therapeutic for small, stable effusions or ultrasound-guided sampling; not for initial management of suspected traumatic hemothorax with respiratory compromise
internal_medicine step2. -
Comparison: Tube thoracostomy vs thoracentesis in traumatic hemothorax — main distinguishing indication?
- Tube thoracostomy: active/large hemothorax or respiratory compromise
- Thoracentesis: small, stable effusion for diagnosis/relief
surgery step2. -
Indicators of massive hemothorax (visual aid in answer)
- Massive hemothorax criteria:
- Initial chest-tube output >1000–1500 mL
- Drainage >200 mL/hr for ≥4 hr
 surgery step2.
surgery step2. -
surgery emergency step2.
-
What are chest x-ray and CT features of hemothorax?
- CXR: fluid along diaphragm with blunted costophrenic angle
- CT: hyperdense material between visceral and parietal pleura
surgery emergency step2. -
Which clinical signs mandate immediate tube thoracostomy for hemothorax?
- Tachycardia, tachypnea, increasing O2 requirements
surgery emergency step2. -
Why is tube thoracostomy preferred over thoracentesis for large/rapid hemothorax?
- Removes large blood volume + can be left in place to trend/monitor ongoing bleeding
surgery emergency step2. -
When would thoracentesis be appropriate for pleural blood?
- Diagnostic use for small/stable pleural effusion; not therapeutic for rapidly accumulating hemothorax
surgery emergency step2. -
What is the primary therapeutic goal of tube thoracostomy in hemothorax?
- Evacuate blood, prevent retained hemothorax, allow monitoring of bleeding
surgery emergency step2. -
Name complications of hemothorax (grouped into ≤3 items).
- Infectious: empyema, superimposed infection
- Pulmonary: atelectasis, fibrothorax
- Hemorrhagic: hemorrhagic shock
surgery emergency step2. -
Imaging features of hemothorax (illustration)
- CXR: blunted costophrenic angle; CT: hyperdense pleural material
surgery emergency step2. -
Preoperative splenectomy: which vaccines are recommended?
- Streptococcus pneumoniae
- Haemophilus influenzae type b
- Neisseria meningitidis
 surgery internal_medicine infectious step2.
surgery internal_medicine infectious step2. -
Splenectomy: primary splenic immune functions?
- Mechanical filtration of opsonized pathogens in sinusoids
- Phagocytosis by splenic macrophages
- Houses immunoglobulin-producing B lymphocytes
internal_medicine surgery step2. -
Asplenia: which organisms cause increased severe infection risk?
- Encapsulated bacteria:
- Streptococcus pneumoniae
- Haemophilus influenzae
- Neisseria meningitidis
infectious internal_medicine step2. -
Splenectomy patients: is antibiotic prophylaxis indicated and which agents?
- May require antibiotic prophylaxis
- Typical agents: penicillin or amoxicillin
internal_medicine surgery step2. -
Why is vaccinating for S. pneumoniae, H. influenzae, and N. meningitidis before splenectomy correct?
- Spleen clears encapsulated organisms; vaccinate against the major encapsulated pathogens to reduce post-splenectomy sepsis risk
infectious surgery step2. -
Why is answer choice A (only N. meningitidis) incorrect for preoperative splenectomy vaccination?
- Choice A vaccinates only N. meningitidis; incomplete because S. pneumoniae and H. influenzae also require vaccination
internal_medicine infectious step2. -
Why is answer choice B (only H. influenzae) incorrect for preoperative splenectomy vaccination?
- Choice B vaccinates only H. influenzae; incomplete because S. pneumoniae and N. meningitidis also require vaccination
internal_medicine infectious step2. -
Why is answer choice C (H. influenzae + N. meningitidis) incorrect for preoperative splenectomy vaccination?
- Choice C omits S. pneumoniae; vaccination must include S. pneumoniae, H. influenzae, and N. meningitidis
internal_medicine infectious step2. -
Why is answer choice D (only S. pneumoniae) incorrect for preoperative splenectomy vaccination?
- Choice D vaccinates only S. pneumoniae; incomplete because H. influenzae and N. meningitidis also require vaccination
internal_medicine infectious step2. -
Why is answer choice E (S. pneumoniae + N. meningitidis) incorrect for preoperative splenectomy vaccination?
- Choice E omits H. influenzae; vaccination must include all three encapsulated organisms
internal_medicine infectious step2. -
Why is answer choice F (S. pneumoniae + H. influenzae) incorrect for preoperative splenectomy vaccination?
- Choice F omits N. meningitidis; vaccination must include S. pneumoniae, H. influenzae, and N. meningitidis
internal_medicine infectious step2. -
Acute pancreatitis: classic presentation and key symptoms
- Severe epigastric abdominal pain that radiates to the back
- Nausea and vomiting
internalmedicine pediatrics step2. -
Acute pancreatitis: common etiologies
- Gallstones
- Alcohol use
- Trauma
- Hypertriglyceridemia
- Hypercalcemia
internalmedicine surgery step2. -
Traumatic epigastric blow: diagnostic relevance
Direct blunt trauma to the epigastrium can cause acute pancreatitis
surgery pediatrics step2. -
surgery internalmedicine step2.
-
internalmedicine step2.
-
Acute pancreatitis: initial supportive management
- IV fluids (normal saline or lactated Ringer)
- Bowel rest
- Pain control
internalmedicine surgery step2. -
When is surgical intervention indicated in acute pancreatitis?
Surgery if complications develop (eg, necrosis with infection, hemorrhage, persistent pseudocyst requiring intervention)
surgery internalmedicine step2. -
Esophageal rupture: presentation and causes
- Severe retrosternal pain
- Signs of sepsis (fever, tachycardia, hypotension)
- Causes: trauma, endoscopic instrumentation, violent retching
surgery internalmedicine step2. -
Gastric ulcer: symptoms and complications
- Pain worsens with food
- Complications: perforation, stricture, upper GI bleeding (melena or hematochezia)
- Endoscopy: mucosal discontinuity/erythema
internalmedicine gastroenterology step2. -
Gastroenteritis: typical features and etiology
- Nausea, vomiting, diarrhea
- Mild generalized abdominal discomfort
- Typically infectious (viral or bacterial); not trauma-related
internalmedicine pediatrics step2. -
Hepatitis: causes and distinguishing features
- Causes: viral, autoimmune, alcohol, medications
- Features: hyperbilirubinemia with jaundice; typically chronic and not caused by blunt trauma
internalmedicine step2. -
Distinguish acute pancreatitis vs gastroenteritis (key differentiators)
- Pancreatitis: severe focal epigastric pain, nausea/vomiting, often elevated amylase/lipase
- Gastroenteritis: mild generalized pain with diarrhea, infectious, not trauma-related
internalmedicine pediatrics step2. -
Why pancreatitis is the correct diagnosis in a teen with epigastric pain after a kick
Focal severe epigastric pain after epigastric trauma with nausea/vomiting matches acute pancreatitis; trauma is a recognized cause
pediatrics surgery step2. -
What is 'postpartum endometritis' (anchor: diagnosis)?
Acute infection of the uterine endometrium after delivery, typically polymicrobial involving aerobes and anaerobes from the genital tract.
obgyn internal step2. -
Pathophysiology of postpartum endometritis (anchor: pathophysiology)?
Genital-tract microbes enter the uterine cavity during labor/delivery causing polymicrobial infection of the endometrium.
obgyn internal step2. -
Key clinical features of postpartum endometritis (anchor: clinical features)?
- Fever
- Uterine fundus tenderness
- Mucopurulent or foul-smelling lochia
- Leukocytosis
obgyn internal step2. -
Risk factors for postpartum endometritis (anchor: risk factors)?
- Cesarean delivery
- Prolonged rupture of membranes or prolonged labor
- Bacterial vaginosis
- Group B Streptococcus colonization
- Manual removal of placenta
obgyn internal step2. -
Immediate management of suspected postpartum endometritis (anchor: management)?
Start broad-spectrum IV antibiotics promptly; recommended regimen example: clindamycin plus gentamicin.
obgyn internal step2. -
Why is antibiotic therapy correct as the next step in this postpartum patient (anchor: answer-choice logic)?
Clinical picture (fever, uterine tenderness, foul lochia, leukocytosis) indicates endometritis requiring immediate broad-spectrum antibiotics.
obgyn internal step2. -
Why is CT abdomen/pelvis not the best next step for suspected endometritis (anchor: answer-choice logic)?
CT can identify intra-abdominal sources but does not confirm endometritis; it is not routinely used to diagnose endometritis.
obgyn internal step2. -
When is CT abdomen/pelvis useful after postpartum fever (anchor: diagnostics)?
To identify intra-abdominal causes such as surgical-site abscess, retained products of conception, appendicitis, or colitis.
obgyn surgery step2. -
Why is culture of the lochia not the most appropriate next step (anchor: answer-choice logic)?
Culture is not the immediate management step; treating suspected infection with antibiotics is prioritized.
obgyn internal step2. -
Why are endometrial biopsy and transvaginal ultrasound not the immediate next steps (anchor: answer-choice logic)?
They are not first-line tests to manage suspected postpartum endometritis; immediate empiric antibiotics take priority.
obgyn internal step2. -
Example presentation anchor: 36 hours postpartum with fever and foul-smelling lochia—most likely diagnosis?
Postpartum endometritis given timing, uterine tenderness, foul lochia, fever, and leukocytosis after cesarean delivery.
obgyn internal step2. -
Supplementary: slide illustrating key points about postpartum infection (anchor: visual aid)?
See slide for summarized features and management:
 obgyn internal step2.
obgyn internal step2. -
Smoking cessation and pulmonary function in a 37-year-old long-term smoker
- Smoking cessation slows the accelerated age-related decline in pulmonary function and prevents further accelerated worsening
internalmedicine pulmonary step2. -
Pathophysiology of normal aging lungs
- Loss of parenchymal scaffolding → dilation of air spaces (senile emphysema)
- ↑ alveolar dead space
internalmedicine pulmonary step2. -
Effect of smoking on age-related pulmonary decline
- Smoking increases the rate of age-related decline in pulmonary function
internalmedicine pulmonary step2. -
internalmedicine pulmonary step2.
-
Medical management for obstructive lung disease in long-term smokers
- Inhaled antimuscarinics
- Short and long-acting β-agonists
- Inhaled corticosteroids
internalmedicine pulmonary step2. -
Oxygen therapy criteria in chronic lung disease
- Resting or ambulatory O2 saturation < 88% → candidate for oxygen therapy
internalmedicine pulmonary step2. -
Lung cancer risk after smoking cessation (relation to choices B and D)
- Former smokers retain an increased lung cancer risk vs never-smokers, but risk decreases compared with continued smoking
internalmedicine oncology step2. -
Why 'pulmonary function will not decrease further' is incorrect (choice C)
- Age-related pulmonary decline normally continues from ~age 25; cessation slows but does not stop decline
internalmedicine pulmonary step2. -
Smoking and risk of myocardial infarction versus cerebral infarction (relation to choice E)
- Smoking increases risk of both myocardial and cerebral infarction via atherosclerotic buildup in coronary and intracranial arteries
internalmedicine neurology step2. -
Illustration: highlighted teaching points about smoking and lung aging
- Key points: senile emphysema, ↑ dead space, smoking accelerates decline, cessation prevents worsening
 internalmedicine pulmonary step2.
internalmedicine pulmonary step2. -
What is the diagnosis: multiple small (3–5 mm), bright red, slightly raised dome-shaped papules on trunk in a 38-year-old?
Cherry angiomas - Common benign vascular lesions - Appear after age 30
dermatology internalmedicine step2. -
dermatology internalmedicine step2.
-
What is the histologic appearance of a cherry angioma?
Congested, dilated capillaries and venules within the superficial dermis
pathology internalmedicine step2. -
What diagnostic study is most appropriate to confirm cherry angiomas?
None — no diagnostic studies required; diagnosis is clinical
dermatology internalmedicine step2. -
When is excisional biopsy appropriate for cherry angiomas?
Not required for diagnosis; biopsy/excision only if cosmetic concern or irritation
surgery dermatology step2. -
How should physicians manage patients who develop cherry angiomas?
Provide reassurance; offer removal only if desired for cosmetics/irritation
internalmedicine dermatology step2. -
Gastroenteritis: typical features and relation to blunt abdominal trauma?
Nausea, vomiting, diarrhea, mild generalized abdominal discomfort; usually infectious (viral/bacterial); not associated with abdominal trauma
infectiousdisease internalmedicine step2. -
When is acute pancreatitis likely and what lab findings support it?
Severe epigastric pain radiating to back with nausea/vomiting; can follow direct epigastric trauma; labs show ↑ serum amylase and lipase
gastroenterology internalmedicine step2. -
Hepatitis: common causes and typical presentation features?
Caused by viral infection, autoimmune disease, alcohol, or medications; often with hyperbilirubinemia/jaundice; typically chronic, not usually from blunt trauma
hepatology internalmedicine step2. -
Visual: example appearance of cherry angiomas (illustration)
Small red dome-shaped papules on trunk consistent with cherry angiomas
 dermatology internalmedicine step2.
dermatology internalmedicine step2. -
Diagnosis: Chronic bacterial prostatitis — key presenting features in this case?
- Painful ejaculation, sometimes dark/foul ejaculate
- Chronic pelvic or low back pain (weeks–months)
- **Mildly tender, minimally enlarged prostate on DRE
internalmedicine step2 -
Risk factors: What sexual history findings increase suspicion for chronic bacterial prostatitis?
- Multiple sexual partners
- Inconsistent condom use / unprotected anal sex
- Concomitant STIs
internalmedicine step2 -
Diagnostic test: What is the two-glass test for prostatitis?
- Urine sample before prostatic massage then urine sample after prostatic massage used for microscopy/culture
internalmedicine step2 -
Diagnostic criterion: How is prostate localization established using post-massage cultures?
A ≥10-fold increase in bacterial concentration after prostatic massage localizes infection to the prostate
internalmedicine step2 -
Treatment: First-line therapy for chronic bacterial prostatitis?
- Fluoroquinolone antibiotics (prolonged courses; recurrences common)
internalmedicine step2 -
Prognosis modifiers: Factors affecting cure rates for chronic bacterial prostatitis?
- Higher cure in antibiotic-naive patients
- Lower cure with prostatic calculi
internalmedicine step2 -
Choice rationale: When is CT pelvis useful instead of two-glass test for prostate-related disease?
- CT pelvis: evaluate prostate cancer metastasis or prostatic abscess (abscess usually has systemic symptoms: fever, chills, malaise)
internalmedicine step2 -
Choice rationale: When is abdominal ultrasonography appropriate vs prostatitis testing?
- Abdominal US: evaluate pyelonephritis or kidney stones (flank pain, fever, nausea) — not for uncomplicated prostatitis
internalmedicine step2 -
Choice rationale: When is placement of urinary catheter for culture appropriate?
- Urinary catheter cultures: when patient cannot void or to evaluate suspected bacterial cystitis from obstruction; not for localizing prostate infection
internalmedicine step2 -
Diagnostic aid: Example of two-glass test visual aid
Illustration of pre- and post-prostatic massage urine collection for microscopy and culture
 internalmedicine step2
internalmedicine step2 -
Chronic bacterial prostatitis: core presenting symptoms?
- Recurrent UTI symptoms
- Pelvic/lower abdominal pain
- Dysuria or painful ejaculation
internal step2. -
Chronic bacterial prostatitis: additional possible features?
- Obstructive urinary symptoms
- Sexual dysfunction
urology step2. -
Risk factors for chronic bacterial prostatitis?
- Multiple sexual partners
- Unprotected anal sex
- Concomitant STIs
obgyn step2. -
Diagnostic test that establishes chronic bacterial prostatitis?
- Urine cultures before and after prostatic massage showing a ten-fold increase in bacterial concentration
internal step2. -
pharmacology step2.
-
infectious step2.
-
When is transrectal prostate ultrasonography useful?
- To identify prostatic calculi or prostatic abscesses
surgery step2. -
Why transrectal prostate ultrasonography is not diagnostic for chronic bacterial prostatitis?
- Findings nonspecific and insufficient to establish diagnosis; lacks sensitivity without abscess/calculi
radiology step2. -
When would transrectal ultrasonography be the correct test in prostatitis-like illness?
- Suspected prostatic abscess or suspected prostatic calculi with systemic/abscess signs
internal step2. -
Foul-smelling or dark ejaculate: suggests which diagnosis over cystitis?
- Suggests prostatic or seminal tract involvement; not consistent with isolated cystitis
infectious step2. -
Diagnosis: Key features supporting cardiogenic shock in a 76-year-old man
- Hypotension (BP 84/56 → 78/42)
- Pulmonary edema (diffuse crackles, respiratory distress, low O2 sat)
- Elevated JVD to angle of jaw
- Low EF (10%) after anterior MI
internal_medicine cardiology step2. -
Pathophysiology: How cardiogenic shock causes hypotension and pulmonary edema
- Pump failure → reduced cardiac output → hypotension
- ↑Left-sided end‑diastolic pressure → pulmonary venous congestion → pulmonary edema
internal_medicine cardiology step2. -
Management: First-line pharmacologic therapy for cardiogenic shock after MI
- Dobutamine (inotropic support) often first-line; may combine with vasopressor if needed
internal_medicine cardiology step2. -
Drug: Dobutamine mechanism relevant to cardiogenic shock
- β1 agonist → ↑contractility, ↑HR, ↑cardiac output
- Modest α1 activity → modest ↑peripheral vascular tone to help MAP
internal_medicine cardiology step2. -
Drug: Norepinephrine role in cardiogenic shock
- α‑agonist predominance → strong vasoconstriction to raise MAP
- Minimal inotropy; used alone or with dobutamine if vasoplegia or severe hypotension
internal_medicine cardiology step2. -
Comparison: Dobutamine vs Norepinephrine in cardiogenic shock
- Dobutamine: primary inotrope (↑CO)
- Norepinephrine: primary vasopressor (↑MAP)
- Use dobutamine for pump failure; add norepinephrine if MAP remains low
internal_medicine cardiology step2. -
Drug: Why vasopressin (ADH) is not first-line for cardiogenic shock
- V1 receptor → vasoconstriction ↑MAP
- No inotropy; causes reflex ↓HR and ↓cardiac output → worsens pump failure
internal_medicine pharmacology step2. -
Drug: Why isoproterenol is harmful after acute MI with cardiogenic shock
- Nonselective β agonist → ↑HR and contractility but ↓SVR → ↓coronary perfusion and ↑myocardial O2 demand → worsens ischemia
internal_medicine cardiology step2. -
Drug: Why phenylephrine is not recommended as first-line in cardiogenic shock
- Pure α1 agonist → ↑afterload and peripheral resistance
- No inotropy; ↑afterload may reduce stroke volume and cardiac output in pump failure
internal_medicine pharmacology step2. -
Clinical decision: When to add a vasopressor to dobutamine in cardiogenic shock
- Add vasopressor (eg, norepinephrine) if mean arterial pressure remains low despite inotropic support
internal_medicine cardiology step2. -
Visual aid: Dobutamine mechanism and effect on hemodynamics (image on answer)
- Dobutamine: β1 → ↑contractility and CO; modest α1 → mild ↑SVR
 internal_medicine cardiology step2.
internal_medicine cardiology step2. -
Cardiogenic shock: defining clinical presentation?
- Hypotension
- Evidence of end-organ damage
- Context: acute decompensated heart failure
internalmedicine cardiology step2. -
Cardiogenic shock: first-line therapy?
- Inotropic support (first-line)
- Examples: dobutamine or dopamine
internalmedicine cardiology step2. -
Dobutamine: role in cardiogenic shock?
- Inotropic agent recommended as a first-line option for cardiogenic shock
internalmedicine cardiology step2. -
Dopamine: role in cardiogenic shock?
- Inotropic agent recommended as a first-line option for cardiogenic shock
internalmedicine cardiology step2. -
Norepinephrine: role in cardiogenic shock?
- Vasopressor adjunct: may be used in conjunction with inotropic agents
internalmedicine cardiology step2. -
Cardiogenic shock: summary slide (visual aid)?
Slide shows key points: hypotension, end-organ damage, first-line inotropes (dobutamine, dopamine), norepinephrine adjunct.
internalmedicine cardiology step2. -
Upper-extremity deep venous thrombosis (UEDVT): key pathophysiology
- Thoracic outlet compression injures axillary/subclavian vein with repetitive use
- Repetitive vigorous upper-extremity activity predisposes to thrombosis
internalmedicine step2. -
Upper-extremity DVT: typical clinical presentation
- Young healthy athlete after vigorous upper-body exercise
- Arm/shoulder/neck pain, unilateral swelling, bluish forearm/hand discoloration
- Dilated superficial collateral veins (Urschel sign)
internalmedicine step2. -
Why is venous thrombosis the most likely cause of this patient's unilateral arm swelling?
- Presentation matches UEDVT: recent vigorous upper-body activity, unilateral edema, bluish discoloration, prominent superficial chest/shoulder veins
internalmedicine step2. -
Diagnosis of upper-extremity DVT: preferred test and finding
- Doppler ultrasonography showing a noncompressible vessel with intravascular thrombus
 internalmedicine step2.
internalmedicine step2. -
internalmedicine step2.
-
Arterial occlusion: when would this explain limb findings?
- Acute limb ischemia with severe pain, pallor, paresthesia, pulselessness, poikilothermia (not isolated swelling)
surgery step2. -
Compartment syndrome: pathophysiologic mechanism
- Compartment pressure ≈/> diastolic BP → impaired blood flow → ischemia of compartment and downstream structures
surgery step2. -
Hematoma: clinical clues making it the correct cause of limb swelling
- Focal, palpable collection after trauma or in anticoagulated patients; large hematoma would be evident on exam
surgery step2. -
Lymphedema: distinguishing features vs venous obstruction
- Causes: lymphatic obstruction/excision (eg, node dissection, lymphoma)
- Usually localized to a limb; no dilated superficial veins because venous drainage intact
internalmedicine step2. -
UEDVT epidemiology and typical setting
- UEDVT is rare; often occurs in young healthy patients after vigorous upper-extremity activity and thoracic outlet anatomy abnormalities
internalmedicine step2. -
Bacterial tracheitis: key presenting signs in a child
- Severe cough
- Inspiratory stridor
- High fever
- Intercostal/suprasternal retractions
- Generally clear lung sounds
pediatrics infectious step2. -
Bacterial tracheitis: typical causative organisms
- Streptococcus pneumoniae
- Haemophilus influenzae
- Staphylococcus aureus
pediatrics infectious step2. -
Bacterial tracheitis: characteristic chest x-ray finding
- Tracheal air column with irregular ('shaggy') borders; may have peribronchial cuffing
radiology pediatrics step2. -
Bacterial tracheitis: first-line management
- IV antibiotics plus corticosteroids; admit for monitoring; intubate if respiratory failure
pediatrics internal_medicine step2. -
Why is croup (laryngotracheobronchitis) less likely in this child?
- No improvement after 2 doses of nebulized racemic epinephrine, making bacterial tracheitis more likely
pediatrics infectious step2. -
When is epiglottitis the correct diagnosis instead of bacterial tracheitis?
- Acute severe throat pain, drooling, difficulty swallowing, muffled voice, trismus, visible swollen epiglottis
pediatrics emergency step2. -
When is bronchiolitis the correct diagnosis instead of bacterial tracheitis?
- Infant/young child with runny nose, cough, tachypnea, wheezing, often due to RSV; usually low-grade fever
pediatrics infectious step2. -
When is peritonsillar abscess the correct diagnosis instead of bacterial tracheitis?
- Sore throat, unilateral tonsillar swelling, trismus, drooling, fever, difficulty opening mouth
otolaryngology pediatrics step2. -
Bacterial tracheitis: diagnosis cues and role of imaging
- Diagnosis clinical: severe cough, high fever, stridor, clear lungs; chest x-ray may show 'shaggy' tracheal air column (see image)
 pediatrics radiology step2.
pediatrics radiology step2. -
Bacterial tracheitis: what is the definition?
Potentially serious bacterial upper respiratory infection of the trachea.
pediatrics step2. -
Bacterial tracheitis: common presenting respiratory signs/symptoms?
- Cough
- Increased work of breathing
- Stridor
pediatrics step2. -
internal_medicine step2.
-
internal_medicine step2.
-
Bacterial tracheitis: chest x-ray finding?
Tracheal air column with irregular borders on chest x-ray.
radiology step2. -
Bacterial tracheitis: first-line management components?
- Antibiotics
- Corticosteroids
- Often hospitalization
pediatrics internal_medicine step2. -
surgery step2.
-
Bacterial tracheitis: supportive image illustrating tracheal air column (useful but not required to answer)
Chest x-ray may show a tracheal air column with irregular borders.
radiology step2. -
ECMO decision for a 37-year-old woman with cystic fibrosis, recurrent pulmonary failure, and refusal of lung transplant: what is the appropriate assessment?
- ECMO is unlikely to change the patient's outcome
internalmedicine surgery step2. -
Patient competence in treatment decisions: what is the documented status for this patient?
- Mentally competent per psychologic testing during the past year
psychiatry internalmedicine step2. -
Scope of the patient's living will in this case:
- No cardiopulmonary resuscitation (no CPR) if cardiac arrest while hospitalized
internalmedicine ethics step2. -
Relevance of the patient's repeated refusal of lung transplant to decision-making:
- Patient repeatedly refused consideration for lung transplant
internalmedicine ethics step2. -
Current respiratory support status of the patient in the ICU:
- Heavily sedated, intubated, and mechanically ventilated
criticalcare internalmedicine step2. -
Why does the living will not automatically prohibit ECMO in this patient?
- Living will specifies no CPR only; it does not state refusal of ECMO
internalmedicine ethics step2. -
When should family members initiate medical treatment plans for a hospitalized patient?
- When the patient lacks decision-making capacity; not when patient is documented competent
ethics internalmedicine step2. -
Gastroenteritis: typical features described in the text
- Nausea, vomiting, diarrhea, mild generalized abdominal discomfort; typically infectious and self-limiting
internalmedicine pediatrics step2. -
Acute pancreatitis: characteristic clinical presentation
- Severe epigastric pain radiating to the back with nausea and emesis
internalmedicine surgery step2. -
internalmedicine surgery step2.
-
Acute pancreatitis: possible relation to trauma per the text
- Can occur after direct abdominal trauma to the epigastric region
surgery trauma step2. -
Hepatitis: typical features and causes mentioned
- Causes: viral, autoimmune, alcohol, medications; feature: hyperbilirubinemia with jaundice; typically chronic
internalmedicine infectiousdisease step2. -
Chronic transplant nephropathy: key pathophysiologic mechanism?
- CD4+ T cell response to donor peptides (eg, MHC) → cytokines → humoral (type II) + cellular (type IV) injury → vascular arteriosclerosis, smooth muscle proliferation → parenchymal fibrosis and atrophy
internal_medicine step2. -
Chronic transplant nephropathy: typical clinical manifestations?
- Progressive transplant dysfunction over months–years → fatigue, anorexia, edema; rising BUN/creatinine and anemia as in this patient (BUN 50 mg/dL, Cr 5.3 mg/dL, Hb 8 g/dL)
internal_medicine step2. -
Chronic transplant nephropathy: diagnostic evaluation?
- Serum/urine tests, kidney ultrasonography, biopsy showing arteriosclerosis, fibrosis, atrophy
internal_medicine step2. -
Chronic transplant rejection: response to standard immunosuppression?
- Not adequately prevented by immunosuppressive therapy; leads to organ failure and may require dialysis or repeat transplant
internal_medicine step2. -
Acute cellular rejection of a renal allograft: immune mediator and timing?
- CD8+ T lymphocytes recognizing donor class I MHC on graft cells; occurs within 6–12 months posttransplant and responds to increased immunosuppression
internal_medicine step2. -
Gastroenteritis: typical features that distinguish it from transplant failure?
- Nausea, vomiting, diarrhea, mild generalized abdominal discomfort; usually viral or bacterial and self-limited, not linked to progressive renal dysfunction
internal_medicine step2. -
Examples of chronic rejection in other transplanted organs
- Liver: vanishing bile duct syndrome
- Lung: bronchiolitis obliterans
- Heart: accelerated atherosclerosis
internal_medicine step2. -
Chronic transplant nephropathy: illustrative biopsy/ultrasound as supplement
Image: chronic transplant changes (arteriosclerosis, fibrosis, atrophy) shown for illustration
 internal_medicine step2.
internal_medicine step2. -
Viral hepatitis: key lab pattern suggesting acute viral hepatitis in this case
- Markedly ↑ AST/ALT (AST 1095, ALT 1300 U/L)
- Hyperbilirubinemia (total 11 mg/dL, direct 2.2 mg/dL)
- Normal leukocyte count (5800/mm3)
internal_medicine step2. -
Viral hepatitis: common causes of acute hepatitis listed
- Viral infections
- Alcohol, medications
- Autoimmune disease, ischemic injury
internal_medicine step2. -
Viral hepatitis: common presenting symptoms
- Fatigue, nausea, vomiting
- Right upper quadrant pain, jaundice, pruritus, abdominal distension
internal_medicine step2. -
Viral hepatitis: initial serologic tests mentioned
- Anti-hepatitis A IgM and IgG
- Anti-hepatitis C IgM and IgG
- Multiple anti-HBV antibodies and antigens
infectious_disease internal_medicine step2. -
Viral hepatitis: initial management approach
- Supportive care
- Treat complications (metabolic abnormalities, hepatic encephalopathy)
- Pursue specific therapy after identifying cause
internal_medicine step2. -
Cholangitis: clinical features and typical labs that distinguish it from viral hepatitis
- Features: fever, jaundice, RUQ pain (Charcot triad)
- Labs: leukocytosis, ↑ALP, ↑GGT, ↑bilirubin; transaminase rise usually milder than hepatitis
surgery internal_medicine step2. -
Cholecystitis: presentation and typical lab expectations
- Presentation: RUQ pain, fever, leukocytosis; usually due to cystic duct obstruction (gallstone)
- Labs: bile duct usually patent → ALT/AST and bilirubin often not elevated unless concomitant cholangitis/choledocholithiasis
surgery internal_medicine step2. -
Choledochal cyst: typical age, symptoms, and usual lab findings
- Age: often <10 years but can present in adults
- Symptoms: abdominal pain, jaundice, palpable mass, nausea/vomiting
- Labs: usually normal liver enzymes (biliary duct often not obstructed)
pediatrics surgery step2. -
Comparison: Why viral hepatitis fits this patient vs cholangitis or cholecystitis
- Viral hepatitis fits: marked ALT/AST rise + normal leukocytes
- Cholangitis expects: leukocytosis + cholestatic pattern (↑ALP/GGT)
- Cholecystitis expects: leukocytosis and localized gallbladder disease without major transaminase rise
internal_medicine surgery step2. -
Viral hepatitis: illustrative slide of teaching points (image on answer side)
Key tests and features summarized below.
- Marked ↑ AST/ALT; hyperbilirubinemia; normal WBC
internal_medicine infectious_disease step2. -
Acute viral hepatitis: key clinical features?
- Fatigue
- Nausea/vomiting
- RUQ pain
- Jaundice
- Pruritus
- Abdominal distension
internal_medicine step2. -
internal_medicine step2.
-
Viruses often implicated in acute viral hepatitis (group 1)?
- Hepatitis A virus (HAV)
- Hepatitis B virus (HBV)
- Hepatitis C virus (HCV)
internal_medicine infectious_disease step2. -
Viruses often implicated in acute viral hepatitis (group 2)?
- Varicella zoster virus (VZV)
- Cytomegalovirus (CMV)
- Epstein-Barr virus (EBV)
- Herpes simplex virus 1/2 (HSV-1/2)
internal_medicine infectious_disease step2. -
Acute viral hepatitis: initial management approach?
Supportive care; treat complications until specific antiviral chosen after virus ID
internal_medicine step2. -
internal_medicine step2.
-
Pancreatic pseudocyst: patient population and frequency?
Occurs in about 10% of patients with chronic pancreatitis
surgery internal_medicine step2. -
Pancreatic pseudocyst: common presenting symptoms when symptomatic?
- Abdominal pain
- Early satiety
- Weight loss (from mass effect)
surgery internal_medicine step2. -
Acute pancreatitis: typical clinical presentation?
- Epigastric pain
- Nausea/vomiting
- Often with gallstones, alcohol, or trauma
surgery internal_medicine step2. -
surgery internal_medicine step2.
-
Pancreatitis: diagnostic lab marker specificity?
Elevated lipase is a specific indicator of pancreatitis
internal_medicine step2. -
Why acute viral hepatitis is more likely than pancreatitis in a patient with very large ALT/AST rise and no clear pancreatitis history?
Because acute viral hepatitis produces large acute ALT/AST increases; pancreatitis usually causes prominent abdominal pain and elevated lipase
internal_medicine step2. -
When would pancreatitis be the correct diagnosis instead of acute viral hepatitis?
When patient has epigastric pain, nausea/vomiting, risk factors (gallstones, alcohol), and elevated lipase
surgery internal_medicine step2. -
When would pancreatic pseudocyst explain symptoms instead of acute viral hepatitis?
When chronic pancreatitis history plus mass symptoms (early satiety, weight loss, abdominal pain) suggest a pseudocyst
surgery internal_medicine step2. -
Clinical diagnosis: 9-year-old with 5-month intermittent right flank pain, absent left kidney on ultrasound, severe dilation of right renal pelvis. What is the clinical problem?
- Single functioning kidney with hydronephrosis
pediatrics surgery step2. -
Pathophysiology: How does vesicoureteral reflux lead to kidney failure?
- Reflux → hydroureter/hydronephrosis → compression atrophy (reflux nephropathy) → progressive renal parenchymal loss
pediatrics internalmedicine step2. -
Key management: Most appropriate immediate intervention to prevent progression of renal failure from proximal ureteral obstruction in a single kidney?
- Insert percutaneous nephrostomy tube (temporary decompression)
surgery pediatrics step2. -
Rationale: Why is percutaneous nephrostomy preferred here?
- Directly decompresses proximal obstruction/hydronephrosis to preserve renal parenchyma before definitive repair
surgery pediatrics step2. -
When is a urinary catheter the correct immediate intervention for urinary obstruction?
- Bladder outlet obstruction (eg, urethral stricture/retention) with overflow incontinence or palpable suprapubic mass
urology pediatrics step2. -
Why is a urinary catheter NOT appropriate for this patient?
- Obstruction is proximal (ureteral), not bladder outlet; catheter won't decompress hydronephrosis
surgery pediatrics step2. -
When is cystoscopy with bladder outlet dilatation appropriate for urinary obstruction?
- Distal bladder outlet obstruction amenable to endoscopic dilation (eg, urethral stricture, posterior urethral valves)
urology pediatrics step2. -
Why is cystoscopy with bladder outlet dilatation NOT appropriate for this patient?
- No bladder outlet obstruction signs; imaging shows proximal ureteral/renal pelvis dilation
surgery pediatrics step2. -
When is intravenous furosemide indicated in renal/volume management?
- Acute hypervolemia (eg, pulmonary edema from heart failure) to increase diuresis
internalmedicine pediatrics step2. -
Why is intravenous furosemide inappropriate in obstruction-related hydronephrosis?
- Increasing urine production with outflow obstruction can worsen postrenal azotemia and hydronephrosis
internalmedicine pediatrics step2. -
When is IV 0.9% saline bolus indicated in acute management?
- Hypovolemia or distributive shock with signs of volume depletion (eg, hypotension, dry mucous membranes)
internalmedicine pediatrics step2. -
Why is IV 0.9% saline bolus inappropriate for this patient?
- No hypovolemia signs; extra intravascular volume may worsen hydronephrosis and renal injury
internalmedicine pediatrics step2. -
Congenital urinary tract anomalies associated with ureteral obstruction or reflux (examples relevant to single-kidney patients)
- Unilateral renal agenesis,
- Duplex collecting system,
- Ureteral stricture/stenosis
pediatrics surgery step2. -
Clinical priority in patients with unilateral renal agenesis
- Preserve function of the solitary kidney (prevent obstruction/reflux injury)
pediatrics internalmedicine step2. -
Ultrasound finding anchor: Absent left kidney and severe right renal pelvic dilation implies what immediate risk?
- High risk of progressive renal parenchymal loss and kidney failure from obstruction
radiology pediatrics step2. -
Supplement: Illustration of hydronephrosis in single kidney—useful for visualizing severe renal pelvis dilation
- See image for renal pelvic dilation:
- Image is illustrative only; diagnosis based on ultrasound and clinical features above
radiology pediatrics step2. - See image for renal pelvic dilation:
-
Percutaneous nephrostomy tube: primary clinical indication?
- Temporary drainage to prevent progression of kidney failure
- When definitive management of vesicoureteral reflux or ureteral obstruction is pending
surgery pediatrics internal_medicine step2. -
Vesicoureteral reflux (VUR) or ureteral obstruction: role of percutaneous nephrostomy?
- Bridge therapy: provides temporary urinary diversion before definitive repair of VUR or relief of obstruction
urology surgery step2. -
Percutaneous nephrostomy tube: intended immediate benefit to renal function?
- Prevents progression of kidney failure by decompressing obstructed urinary tract
nephrology internal_medicine step2. -
Anchor: Nonadherence in 21-year-old with type 2 diabetes; defining features?
- Age 21, type 2 diabetes, A1c 9%, admits not checking glucose to be 'like everyone else', on metformin + glipizide
internal_medicine step2 -
Anchor: Best physician approach for young diabetic nonadherent due to social perception
- Organize multidisciplinary care + peer support group for young patients with diabetes
internal_medicine psychiatry step2 -
Anchor: Why multidisciplinary care + peer support is correct for social-perception nonadherence?
- Addresses emotional/social causes, connects patient with similar peers, improves disease perception and adherence
psychiatry internal_medicine step2 -
Anchor: When is contacting a patient's parent appropriate?
- Appropriate when patient lacks decision-making capacity; otherwise contacting parent breaches trust and HIPAA
internal_medicine ethics step2 -
Anchor: When is a mobile glucose app likely effective for nonadherence?
- Effective when barrier = difficulty/complexity of monitoring; not effective when barrier = social desire to fit in
internal_medicine step2 -
Anchor: When is scare/threatening counseling (eg, 'you will be blind') appropriate?
- Scare tactics are inappropriate; education about complications should be empathetic and nonthreatening
internal_medicine psychiatry step2 -
Anchor: Use of humor with a patient admitting nonadherence due to social stigma
- Humor may damage rapport here; prefer empathetic, nonjudgmental, open-ended inquiry
psychiatry internal_medicine step2 -
Anchor: Clinical communication principle for nonadherence evaluation
- Use open-ended, curious, nonjudgmental questions to identify root cause before planning interventions
psychiatry internal_medicine step2 -
Anchor: Study-note rule: overriding refusals or contacting others
- Assess decision-making capacity before overriding refusals or notifying others
internal_medicine ethics step2 -
Anchor: Choice E — strengthen physician-patient relationship. Why is this option insufficient for treatment nonadherence?
Strengthening relationship is humanistic but does not address underlying nonadherence drivers; the patient needs multi‑front support to realize others share his experience.
internalmedicine step2. -
Anchor: Treatment nonadherence. Common practical reasons (group A)?
- Financial strains
- Treatment side effects
- Poor health literacy causing misunderstanding
internalmedicine step2. -
Anchor: Treatment nonadherence. Common psychosocial reasons (group B)?
- Social perception or judgment
- Mental/emotional strain from adjustment
psychiatry step2. -
Anchor: Approach to a nonadherent patient. What clinician attitude is recommended?
Use an open‑ended, curious, nonjudgmental approach to explore reasons for nonadherence.
internalmedicine step2. -
Anchor: When is peer support indicated for a nonadherent patient?
When the patient needs reassurance that many others share his experience and multi‑front support beyond the clinician relationship.
psychiatry step2. -
Anchor: Use of image. What supplementary purpose can a highlighted slide image serve when teaching about nonadherence?
Illustrate emphasized teaching points; image as supplement only, not as sole source of the answer.
 internalmedicine step2.
internalmedicine step2. -
Diagnosis: Tingling in left ring and small fingers + medial forearm sensory loss in a 62-year-old with left arm dialysis fistula — most likely diagnosis?
- Ulnar nerve compression
neurology internal_medicine step2. -
Pathophysiology: How does an elbow arteriovenous fistula cause neuropathy?
- AV fistula at elbow → local compression/traction of ulnar nerve
neurology surgery step2. -
Feature: Sensory distribution of ulnar nerve compression at the elbow?
- Numbness/paresthesia: ring and small fingers; medial hand; medial forearm to elbow
neurology step2. -
Feature: Motor findings expected with ulnar nerve compression at the wrist vs elbow?
- Wrist compression → hand weakness and intrinsic atrophy; Elbow compression → sensory ± weakness
neurology step2. -
Diagnostic test to confirm suspected ulnar nerve compression?
- Electrodiagnostic testing (nerve conduction/EMG)
neurology internal_medicine step2. -
Initial management for ulnar nerve compression related to dialysis fistula?
- Behavior modification and ergonomic measures
neurology surgery step2. -
When is surgery indicated for ulnar nerve compression?
- Severe or refractory symptoms after conservative measures
surgery neurology step2. -
Arteriovenous steal syndrome: when would this diagnosis fit in a dialysis patient?
- Ischemic distal limb signs: pallor, pain during dialysis, pain at rest; uncommon to localize only to ring/small fingers
internal_medicine nephrology step2. -
Why is diabetic neuropathy unlikely to explain isolated ring/small finger and medial forearm sensory loss?
- Diabetic neuropathy causes symmetric distal polyneuropathy, not focal ulnar distribution
neurology internal_medicine step2. -
Why are central causes (eg, cerebral infarction) unlikely for isolated medial hand and forearm sensory loss?
- Cerebral infarction causes contralateral cortical or hemispheric deficits, not focal peripheral nerve distribution to ring/small fingers and medial forearm
neurology internal_medicine step2. -
Use of provided image: What clinical sign near a dialysis fistula suggests local hemodynamic device presence without inflammation?
- Palpable thrill at fistula site
 internal_medicine surgery step2.
internal_medicine surgery step2. -
Essential (pre-existing) hypertension in pregnancy: diagnostic blood pressure criteria and timing?
- Systolic > 140 mm Hg or diastolic > 90 mm Hg
- On ≥2 measurements ≥4 hours apart
- Before 20 weeks' gestation
obgyn internal step2. -
Why is the 37-year-old patient in the vignette diagnosed with essential hypertension?
- BP 150/100 and 150/98 at 18 wk (before 20 wk) with trace urine protein → meets pre-existing HTN criteria; urine protein can be normal in essential HTN
obgyn internal step2. -
Normal urine protein result significance in essential hypertension during pregnancy?
- Urine protein often normal in essential (pre-existing) hypertension
obgyn internal step2. -
Gestational hypertension: when would this diagnosis apply?
- New hypertension after 20 weeks' gestation without proteinuria
obgyn internal step2. -
Preeclampsia: defining feature that distinguishes it from essential hypertension?
- Hypertension with new proteinuria or end-organ dysfunction after 20 weeks' gestation
obgyn internal step2. -
Superimposed preeclampsia on essential hypertension: when is this diagnosis correct?
- Patient has pre-existing hypertension before 20 wk and then develops new proteinuria or worsening HTN/end-organ signs
obgyn internal step2. -
Transient hypertension in pregnancy: defining features?
- Temporary BP elevation without persistent hypertension and no proteinuria, typically resolves
obgyn internal step2. -
Physiologic blood pressure change in early pregnancy relevant to diagnosis?
- BP decreases between 12 and 19 weeks' gestation, which can mask pre-existing HTN
obgyn internal step2. -
Maternal and fetal risks associated with essential hypertension in pregnancy?
- Mother: superimposed preeclampsia, postpartum hemorrhage
- Fetus: fetal growth restriction, preterm birth, placental abruption
obgyn internal step2. -
Initial management principles for essential hypertension in pregnancy?
- Oral antihypertensives and increased maternal-fetal monitoring
obgyn internal step2. -
Slide image: visual highlight of teaching points (supplementary)
- Supplementary image:
- Image illustrates highlighted teaching points; question answers must be known without the image
obgyn internal step2. - Supplementary image:
-
Diagnosis: 42-year-old transplant patient with Ca2+ 11.7 mg/dL and PTH 425 pg/mL; chronic kidney failure history. What is the most likely diagnosis?
- Tertiary hyperparathyroidism
internal_medicine surgery step2. -
Pathophysiology: What causes tertiary hyperparathyroidism in chronic kidney disease?
- Long-term secondary hyperparathyroidism → parathyroid hyperplasia → autonomous PTH secretion → persistent hypercalcemia
internal_medicine surgery step2. -
Lab pattern: What combination of serum calcium and PTH occurs in tertiary hyperparathyroidism?
- Elevated serum Ca2+ with persistently elevated PTH
internal_medicine step2. -
Treatment: Primary management for tertiary hyperparathyroidism?
- Surgical removal of one or more hyperplastic parathyroid glands
 surgery internal_medicine step2.
surgery internal_medicine step2. -
Why is hypervitaminosis D (excess vitamin D) an unlikely cause of this patient's labs?
- Hypervitaminosis D → hypercalcemia but causes suppressed PTH via negative feedback
internal_medicine step2. -
When would hypervitaminosis A be the correct diagnosis instead of tertiary hyperparathyroidism?
- Excess vitamin A with symptoms: dry/itchy skin, hair loss, headaches, nausea/vomiting, fatigue, irritability, joint pain
internal_medicine step2. -
Why is parathyroid adenoma (primary hyperparathyroidism) less likely in this patient with CKD history?
- CKD history more consistent with tertiary hyperparathyroidism from hyperplasia; text states parathyroid adenoma would present with decreased PTH concentrations
internal_medicine step2. -
Why is thyrotoxicosis an unlikely explanation for this patient's hypercalcemia and PTH elevation?
- Thyrotoxicosis causes hyperthyroid symptoms (palpitations, tremor, weight loss) and involves thyroid hormones, not autonomous PTH secretion
internal_medicine step2. -
Clinical features of hyperparathyroidism to recognize in patients:
- Fatigue; muscle weakness; bone pain; kidney stones
internal_medicine step2. -
Distinguishing parathyroid hyperplasia vs adenoma in hyperparathyroidism context:
- Hyperplasia: multiple glands enlarged, occurs in long-term secondary → tertiary; Adenoma: single gland, primary disease
internal_medicine surgery step2. -
Define the procedure parathyroidectomy.
- Parathyroidectomy: operation to remove one or more hyperplastic parathyroid glands.
surgery step2. -
Meningococcal disease: key clinical presentation
- Fever
- Headache
- Nuchal rigidity
- Altered mental status
- Often preceded by upper respiratory prodrome
internalmedicine step2. -
Neisseria meningitidis: important epidemiologic risk factor
- Communal living (eg, homeless shelters) increases risk of meningococcal disease
infectiousdisease internalmedicine step2. -
Definition of 'close contacts' for meningococcal prophylaxis
- Close contact = proximity within feet for >8 hours or direct exposure to oral secretions
infectiousdisease internalmedicine step2. -
Management anchor: appropriate prophylaxis strategy for hospital personnel exposed to N. meningitidis
- Chemoprophylaxis for close contacts only
internalmedicine step2. -
Why prophylaxis for close contacts is correct for meningococcal exposure
- Chemoprophylaxis decreases spread; close contacts (prolonged proximity or oral secretions) are highest risk
infectiousdisease internalmedicine step2. -
Why prophylaxis for all ED personnel on arrival (Choice A) is incorrect
- Not necessary: personnel not in vicinity for prolonged time are low risk; avoid unnecessary antibiotics and resistance
internalmedicine infectiousdisease step2. -
Why prophylaxis for immunocompromised personnel only (Choice C) is incorrect
- Not inclusive: immunocompetent close contacts are also at risk and should receive prophylaxis
internalmedicine infectiousdisease step2. -
Why no prophylaxis for hospital personnel (Choice D) is incorrect
- Not appropriate: chemoprophylaxis has been shown to decrease transmission among close contacts
infectiousdisease internalmedicine step2. -
pharmacology internalmedicine step2.
-
pharmacology internalmedicine step2.
-
Diagnosis: What diagnosis is most consistent with acute onset severe dyspnea, hypoxemia (SpO2 88%), sinus tachycardia, 1+ bilateral leg edema, recent long-distance immobility (truck driving), and a chest x-ray shown?
- Acute pulmonary embolism (PE)
internal_medicine step2 -
Pathophysiology: What ABG pattern is associated with acute pulmonary embolism?
- Acute respiratory alkalosis with hypoxemia and increased A–a gradient
internal_medicine step2 -
Risk factors: Which immobility-related risk is highlighted for PE in this case?
- Prolonged sitting (long-distance truck driving)
internal_medicine step2 -
Diagnostic test choice: What is the preferred imaging to confirm suspected acute pulmonary embolism?
- Spiral CT scan of the chest (CT pulmonary angiography)
internal_medicine step2 -
D-dimer use: When is a serum D-dimer assay appropriate for suspected PE?
- When clinical suspicion is low but PE cannot be excluded
internal_medicine step2 -
BNP use: When is serum BNP measurement indicated instead of primary PE testing?
- When concern is for congestive heart failure/cardiogenic pulmonary edema
internal_medicine step2 -
Cardiac enzymes: When is measurement of cardiac enzymes the appropriate next step?
- When acute coronary syndrome is suspected (eg, ischemic ECG changes)
internal_medicine step2 -
Chest tube: When is placement of a chest tube indicated in acute respiratory presentation?
- For large pneumothorax or sustained pleural fluid causing respiratory compromise, not for PE
surgery internal_medicine step2 -
Steroids: When is IV hydrocortisone appropriate in acute dyspnea?
- For severe bronchospasm/asthma or adrenal crisis, not for PE without those features
internal_medicine pulmonology step2 -
ECG/clinical features: What ECG and clinical findings are typical but nonspecific for PE?
- Sinus tachycardia and acute dyspnea; ECG often otherwise nonspecific
internal_medicine step2 -
Imaging supplement: Show chest x-ray image associated with the case (illustration only).
 - Chest x-ray provided as supportive image; chest x-ray alone does not confirm PEinternal_medicine radiology step2
- Chest x-ray provided as supportive image; chest x-ray alone does not confirm PEinternal_medicine radiology step2 -
internal_medicine step2
-
Pulmonary embolism: clinical risk factors that prompt rapid testing (group 1)?
- Immobility
- Recent surgery
- Trauma / long-bone fracture
internal_medicine step2 -
Pulmonary embolism: additional clinical risk factors (group 2)?
- Obesity
- Malignancy
- Pregnancy or OCP use
internal_medicine step2 -
Diagnostic test: preferred method to confirm pulmonary embolism?
- Spiral CT scan of the chest (CT pulmonary angiography)
internal_medicine step2 -
D-dimer: limitation when Wells score indicates high pretest probability?
- Negative D-dimer may be false negative; CT angio required
internal_medicine step2 -
Obstructive shock from massive pulmonary embolism: best immediate management principle?
- Remove obstruction: thrombectomy or thrombolysis
internal_medicine step2 -
Hydrocortisone IV: when is it appropriate?
- COPD exacerbation causing SOB
- Hypotension refractory to fluids + vasopressors (suspect adrenal insufficiency)
internal_medicine step2 -
Hydrocortisone IV: why not appropriate for this patient with suspected PE?
- Patient lacks adrenal insufficiency or fluid-refractory hypotension; PE causes obstructive shock not responsive to vasopressors alone
internal_medicine step2 -
internal_medicine step2
-
Chest tube placement: why not appropriate for this patient?
- Patient chest x-ray lacks pleural effusion, hemothorax, pneumothorax
internal_medicine step2 -
Educational rule: when to test rapidly for pulmonary embolism?
- Sudden SOB with risk factors (immobility, surgery, malignancy, pregnancy/OCP, trauma/fracture, thrombophilia) → rapid diagnostic testing
internal_medicine step2 -
Clinical anchor: 82-year-old man with urinary retention (1700 mL turbid urine), hypotension unresponsive to fluids and norepinephrine, leukocytosis, hyponatremia, hyperkalemia, elevated BUN/Cr — what is the most likely endocrine contributor to persistent hypotension?
Adrenal insufficiency
internalmedicine step2. -
Clinical anchor: Which laboratory pattern in this patient supports adrenal insufficiency as a contributor to shock?
- Hyponatremia
- Hyperkalemia (borderline)
- Elevated BUN/Cr
internalmedicine step2. -
Clinical anchor: What is the most appropriate immediate therapy for suspected adrenal insufficiency causing refractory septic hypotension?
Intravenous hydrocortisone (glucocorticoid) supplementation
internalmedicine step2. -
Clinical anchor: Why is hydrocortisone indicated for vasopressor-refractory septic shock?
Glucocorticoid supplementation restores adrenal hormones and improves vasopressor responsiveness in refractory septic hypotension
internalmedicine step2. -
Clinical anchor: When would bladder irrigation with amphotericin B be appropriate instead of hydrocortisone?
Localized urogenital fungal infection requiring topical therapy; not for septic shock or hypotension
internalmedicine step2. -
Clinical anchor: When is intravenous fluconazole appropriate in a septic patient?
Documented or strongly suspected systemic fungal infection sensitive to fluconazole; not for immediate reversal of hypotension
internalmedicine step2. -
Clinical anchor: When is intravenous metronidazole appropriate in an infected patient with hypotension?
For infections by anaerobic bacteria (eg, intra-abdominal, pelvic) as antimicrobial therapy; not a vasopressor or shock reversal agent
internalmedicine step2. -
Clinical anchor: When is immediate hemodialysis indicated for hypotension with elevated BUN/Cr?
Indications: refractory hyperkalemia, volume overload unresponsive to diuretics, or severe uremic complications; mild creatinine rise alone does not mandate emergent dialysis
internalmedicine nephrology step2. -
Clinical anchor: What acute urologic finding in this case likely precipitated the sepsis?
Urinary retention with 1700 mL turbid urine indicating obstructive retention and likely infected bladder/UTI
internalmedicine surgery step2. -
Clinical anchor: How does limited vasopressor responsiveness relate to endocrine causes of shock in sepsis?
Limited vasopressor response is a hallmark of endocrine contributions (eg, adrenal insufficiency) to septic shock
internalmedicine criticalcare step2. -
internalmedicine step2.
-
Acute adrenal insufficiency: next immediate management for persistent hypotension after large-volume IV fluids and vasopressors?
IV glucocorticoids (eg, IV hydrocortisone)
internal_medicine step2. -
Why is IV glucocorticoid therapy correct for acute adrenal insufficiency with refractory hypotension?
Restores cortisol effect when production or responsiveness is insufficient, reversing vasopressor-refractory hypotension
internal_medicine step2. -
Pathophysiology of acute adrenal insufficiency mentioned in the text?
Insufficient adrenal hormone production or reduced responsiveness to adrenal hormones
internal_medicine step2. -
Indications for immediate hemodialysis per the text (group 1 of examples)?
- Life-threatening acidosis (eg, pH <6.9)
- Severe electrolyte derangement (eg, K+ >6.5 mEq/L)
internal_medicine step2. -
Indications for immediate hemodialysis per the text (group 2 of examples)?
- BUN >100 mg/dL with symptoms (pericarditis/encephalopathy)
- Dialyzable toxic ingestion (eg, aspirin)
internal_medicine step2. -
Why is emergent hemodialysis NOT appropriate for this patient now?
Patient is producing urine and does not meet emergent dialysis criteria
internal_medicine step2. -
How should hemodynamic instability be managed relative to dialysis initiation?
Address hemodynamics first or in parallel with dialysis to avoid circulatory collapse
internal_medicine step2. -
When should you suspect acute adrenal insufficiency in a hypotensive patient?
When hypotension persists despite large-volume IV fluids and vasopressors
internal_medicine step2. -
Which clinical action is emphasized as more appropriate than starting antibiotics for this patient's hypotension?
Treat suspected acute adrenal insufficiency with IV glucocorticoids rather than prioritizing empiric antibiotics
internal_medicine step2. -
Illustration: Slide showing highlighted teaching point about management of refractory hypotension — what does the image supplement?
Visual emphasis that IV glucocorticoids are the immediate step for adrenal insufficiency; image:
 internal_medicine step2.
internal_medicine step2. -
internalmedicine oncology step2.
-
internalmedicine oncology step2.
-
internalmedicine pathology step2.
-
Hodgkin lymphoma: required biopsy type for definitive diagnosis?
- Core-needle or excisional lymph node biopsy
internalmedicine surgery step2. -
Fine-needle aspiration (FNA): when is it appropriate for suspected lymphoma?
- Not appropriate for initial lymphoma diagnosis; use core/excisional when architecture needed
internalmedicine oncology step2. -
After Hodgkin lymphoma confirmation by node biopsy: next best staging test?
- PET scan (or contrast CT) to evaluate disease extent
internalmedicine oncology step2. -
Bronchoscopy: when is it indicated in suspected Hodgkin lymphoma?
- Indicated to biopsy intrathoracic pulmonary lesions seen on imaging, not for staging after node diagnosis
internalmedicine pulmonology step2. -
Laparoscopy: role in Hodgkin lymphoma evaluation?
- Not routine; consider only if liver biopsy required and no accessible lymph nodes
internalmedicine surgery step2. -
Pel-Ebstein fever: characteristic pattern in Hodgkin lymphoma?
- Recurrent high fevers 1–2 wk on, 1–2 wk off
internalmedicine infectiousdisease step2. -
Alcohol-induced lymph node pain: significance in Hodgkin lymphoma?
- Specific sign of Hodgkin disease-associated lymphadenopathy
internalmedicine oncology step2. -
internalmedicine laboratory step2.
-
Primary curative treatment approach for Hodgkin lymphoma?
- Chemotherapy often with concurrent radiation depending on location/bulk
internalmedicine oncology step2. -
Prognosis and staging uniqueness of Hodgkin lymphoma?
- Staged differently than other lymphomas and typically favorable prognosis
internalmedicine oncology step2. -
Diagnosis confirmation: what finding on lymph node biopsy confirms the diagnosis?
- Reed-Sternberg cells on core needle or excisional lymph node biopsy
internal_medicine step2 -
internal_medicine step2
-
internal_medicine step2
-
Treatment approach: what therapy is often curative for localized or bulky disease?
- Chemotherapy with concurrent radiation therapy depending on location and bulkiness
internal_medicine step2 -
Imaging example: what scans are shown for extent evaluation (illustration)?
- CT with contrast or PET scan illustrated
 internal_medicine step2
internal_medicine step2 -
Diagnosis: 67-year-old with sudden substernal chest pain, troponin ↑, hypotension, ST elevation in II, III, aVF and V4R–V6R. What is the most likely diagnosis?
- Inferior STEMI with right ventricular infarction
internal step2. -
ECG localization: Which ST-elevation leads indicate an inferior myocardial infarction and which indicate right ventricular involvement?
- Inferior MI: leads II, III, aVF
- Right ventricular infarct: leads V4R–V6R
internal step2. -
Hemodynamics: What does a laterally displaced point of maximal impulse and clear lungs suggest in this patient?
- Left ventricular enlargement/dysfunction with absence of pulmonary edema
internal step2. -
Central venous pressure: What CVP value is recorded and is it within normal range?
- CVP = 6 cm H2O; normal range 5–8 cm H2O
internal step2. -
Management anchor: For right ventricular infarction causing cardiogenic shock, what is the most appropriate initial step?
- IV crystalloid bolus (eg, 0.9% saline) to increase preload
internal step2. -
Why is IV furosemide incorrect as initial therapy for right ventricular infarction with hypotension?
- Diuretics decrease preload; right ventricular infarct patients are preload-dependent → worsens hypotension
internal step2. -
When is IV dobutamine appropriate in cardiogenic shock from right ventricular infarction?
- If shock persists after adequate fluid resuscitation; dobutamine increases contractility
internal step2. -
Why is IV propranolol contraindicated acutely in this hypotensive STEMI patient?
- Nonselective β-blocker (β1/β2) decreases contractility and heart rate → worsens hemodynamic instability
internal step2. -
Initial STEMI care bundle (besides fluids for RV infarct): Which immediate therapies should be given?
- Antiplatelet agents (eg, aspirin, clopidogrel)
- Anticoagulant (eg, heparin)
- Pain control + urgent coronary revascularization
internal step2. -
Why is pulmonary artery catheterization listed as an incorrect initial step in this scenario?
- PA catheterization is not the immediate stabilization step; initial management prioritizes fluids and urgent reperfusion
internal step2. -
Illustration: ECG pattern of inferior STEMI with right ventricular involvement — what leads to check for right ventricular ST elevation? (see image)
- Check right-sided precordial leads V4R–V6R for right ventricular ST elevation
 internal step2.
internal step2. -
ST-elevation myocardial infarction (STEMI): what is its urgency and classic acute presentation?
- True emergency
- Exertional substernal chest pressure
- Dyspnea, diaphoresis, nausea
- Typical patient has risk factors
internal_medicine cardiology step2. -
internal_medicine cardiology step2.
-
STEMI: what ECG finding confirms localization?
- ST-segment elevation in a specific vascular distribution
internal_medicine cardiology step2. -
internal_medicine cardiology step2.
-
internal_medicine cardiology step2.
-
Right ventricular infarction: how does preload status affect initial stabilization?
- Preload-dependent → give intravenous crystalloids (eg, saline) as part of initial stabilization
internal_medicine cardiology step2. -
Administration of propranolol in a hypotensive patient: likely effect on cardiac output and blood pressure?
- Propranolol would decrease cardiac output and worsen hypotension
internal_medicine pharmacology step2. -
Pulmonary artery catheterization (PAC): when is PAC appropriate in shock?
- Useful for undifferentiated shock to assess hemodynamics
internal_medicine criticalcare step2. -
Pulmonary artery catheterization: why is PAC inappropriate when the shock cause is clear?
- Delaying treatment for PAC is inappropriate and potentially harmful when cause of shock is evident
internal_medicine criticalcare step2. -
Isoimmunization to the Kell erythrocyte antibody: strongest predisposing risk factor in this patient?
- History of blood transfusion
obgyn internal_medicine step2. -
Why is prior blood transfusion the strongest risk factor for Kell isoimmunization?
- Greater exposure to foreign RBC antigens; likelihood of isoimmunization rises with amount of blood exposed
obgyn internal_medicine step2. -
Pathophysiology: how do maternal anti-Kell antibodies affect the fetus?
- Maternal IgG antibodies cross placenta → hemolysis of fetal RBCs → fetal hemolytic anemia (eg, erythroblastosis fetalis)
pediatrics obgyn step2. -
How to determine fetal risk for Kell-related hemolysis when mother is anti-Kell positive?
- Determine paternal Kell antigen status; if father Kell-negative → fetus Kell-negative → no risk
obgyn internal_medicine step2. -
When is previous spontaneous abortion a significant risk for RBC isoimmunization?
- When fetal blood exposure occurred during passage of products of conception; it can cause alloimmunization but less than major transfusion exposure
obgyn internal_medicine step2. -
Why does maternal ABO blood group not increase risk for Kell isoimmunization?
- ABO type does not predispose to formation of anti-Kell antibodies
obgyn internal_medicine step2. -
Does Rho(D) immune globulin (RhoGAM) prevent Kell isoimmunization?
- No; RhoGAM decreases Rh(D) isoimmunization but does not prevent anti-Kell formation
obgyn internal_medicine step2. -
Is threatened abortion a strong risk factor for Kell isoimmunization?
- No; threatened abortion (scant bleeding with closed os) is less likely to cause significant fetal blood exposure compared with transfusion or completed abortion
obgyn internal_medicine step2. -
Comparison: blood transfusion vs spontaneous abortion as sources of maternal alloimmunization
- Transfusion: large antigen exposure → higher risk
- Spontaneous abortion: smaller exposure → lower risk (but still possible)
obgyn internal_medicine step2. -
Clinical step: how to assess fetal Kell antigen status when mother is anti-Kell positive (illustration)?
- Check paternal Kell status; if father Kell-positive → fetus may be Kell-positive → risk
obgyn pediatrics step2. - Check paternal Kell status; if father Kell-positive → fetus may be Kell-positive → risk
-
Rh(D) immune globulin: What is the mechanism preventing maternal alloimmunization?
Binds to Rh(D)-positive fetal cells in maternal circulation, preventing maternal immune system from forming anti-Rh(D) antibodies.
obgyn step2. -
Rh(D) immune globulin: Does it prevent maternal antibodies to Kell antigens?
No. Rh(D) immune globulin has no role against Kell antigens and does not change risk of Kell isoimmunization.
obgyn step2. -
Threatened abortion: What is the clinical definition?
Vaginal bleeding before 20 weeks with fetal cardiac activity present and closed cervical os.
obgyn step2. -
Threatened abortion: How does it affect risk of fetal erythrocyte isoimmunization?
It is a risk factor due to fetal–maternal blood mixing but exposes mother to a smaller blood volume than transfusion, so risk is less significant.
obgyn step2. -
Maternal alloimmunization: What exposures can lead to antibody formation?
- Blood transfusion
- Exposure to fetal blood antigens during delivery
internal_medicine step2. -
Alloimmunization risk: What determines likelihood of maternal isoimmunization?
Directly related to the amount of foreign blood exposure (greater exposure → higher likelihood).
internal_medicine step2. -
Fetal consequences: What are major risks from maternal red blood cell alloimmunization?
- Hemolytic anemia
- Erythroblastosis fetalis
- Death
pediatrics obgyn step2. -
When would threatened abortion be the primary concern for isoimmunization risk?
When fetal–maternal bleeding occurs before 20 weeks with fetal cardiac activity and closed os; it raises risk but is less significant than transfusion-level exposure.
obgyn step2. -
Alloimmunization overview: What summary rule links exposures and fetal risk?
Maternal antibodies form after transfusion or fetal blood exposure; magnitude of exposure predicts isoimmunization risk and fetal hemolytic complications.
internal_medicine obgyn step2. -
Illustration: What are the key fetal risks from maternal alloimmunization? (see image)
Key fetal risks: - Hemolytic anemia - Erythroblastosis fetalis - Death
pediatrics obgyn step2. -
Clinical decision: Safe discharge planning for a 92-year-old with acute confusion and poor memory — what is the primary priority?
- Patient safety: ensure safe living environment before discharge
internal_medicine step2. -
Clinical finding: 92-year-old with zero of three-word recall after 5 minutes — what does this suggest about capacity?
- Significant cognitive deficit: likely impaired capacity for independent living
neurology step2. -
Management decision: When is involving social services indicated in discharge planning?
- When patient lacks cognitive ability for self-care; arrange supervised living placement
internal_medicine step2. -
Correct answer rationale: Why is 'arrange placement in a supervised living facility' appropriate here?
- Patient has infections treated, hallucinations resolved, but persistent memory impairment → unsafe to live alone → social services to arrange supervised care
psychiatry step2. -
Option 'Bioethics: futile medical treatment' — when would this be appropriate?
- Appropriate when ongoing treatments provide no meaningful benefit or are medically futile
internal_medicine step2. -
Why is 'palliative care to discuss end-of-life planning' NOT appropriate for this patient now?
- No evidence of terminal/futile illness; current infections improving; immediate need is safe discharge planning, not end-of-life care
palliative step2. -
When would 'psychiatry to address an advance directive' be appropriate?
- Appropriate when assessing decision-making capacity for advance directives or identifying a medical power of attorney
psychiatry step2. -
Why is 'volunteer canine therapy' insufficient as the next step in discharge planning?
- Canine therapy may comfort the patient but does not address unsafe home environment or need for supervised placement
internal_medicine step2. -
Clinical anchor: Features of this patient's acute presentation that indicate delirium rather than chronic dementia
- Acute onset: found lethargic, new agitation/confusion, visual hallucinations that later resolved after treatment
neurology step2. -
Illustration: Slide showing highlighted discharge-planning teaching point — what role does social services play?
- Arrange supervised living for patients with cognitive deficits; see image for emphasis
 internal_medicine step2.
internal_medicine step2. -
Discharge planning: When are social services likely required for a patient?
- When a patient is unable to care for self, especially with no family involvement or help
internalmed step2. -
Discharge planning: What is the benefit of early social services involvement in the clinical course?
- Helps establish an optimum safe-discharge plan
internalmed step2. -
Define amaurosis fugax (clinical anchor).
Brief, transient, unilateral, painless vision loss due to retinal ischemia from microembolization of the ophthalmic artery.
neurology internalmedicine step2 -
Describe Hollenhorst plaque appearance and typical location (retinal finding).
- Yellow, refractile cholesterol embolus
- Located within retinal arterioles, often at arteriolar bifurcations
neurology internalmedicine step2 -
Primary source of emboli causing Hollenhorst plaques (diagnostic anchor).
Ipsilateral carotid arteries are the majority source of emboli causing retinal cholesterol plaques.
neurology internalmedicine step2 -
Most appropriate next diagnostic step for amaurosis fugax with Hollenhorst plaque (clinical decision).
Carotid duplex ultrasonography to evaluate for carotid atherosclerotic/ulcerative plaque.
neurology internalmedicine step2 -
When is echocardiography the preferred test for suspected retinal embolic source (choice C context)?
When emboli originate from calcific valvular plaques or intracardiac thrombus; calcific retinal emboli are chalky white and nonrefractile.
cardiology internalmedicine step2 -
When is cerebral MR angiography or brain MRI useful vs retinal embolic disease (choice B/E context)?
Useful to diagnose ischemic stroke or intracranial vascular lesions but unlikely to find the extracranial carotid source of retinal emboli.
neurology internalmedicine step2 -
Role of intraocular pressure measurement in acute vision loss workup (choice D context).
Measurement of intraocular pressure is important for glaucoma evaluation, not for diagnosing embolic retinal ischemia causing amaurosis fugax.
ophthalmology internalmedicine step2 -
How can treating carotid or cardiac valvular disease affect retinal/cerebral outcomes (management anchor)?
Treatment of carotid vascular or cardiac valvular disease can prevent central retinal artery occlusion and stroke.
neurology internalmedicine step2 -
Fundus photo: what finding supports carotid-source cholesterol embolus? (use image on answer for illustration)
Yellow, refractile plaques in retinal arterioles (Hollenhorst plaques) suggest carotid atheroembolism.
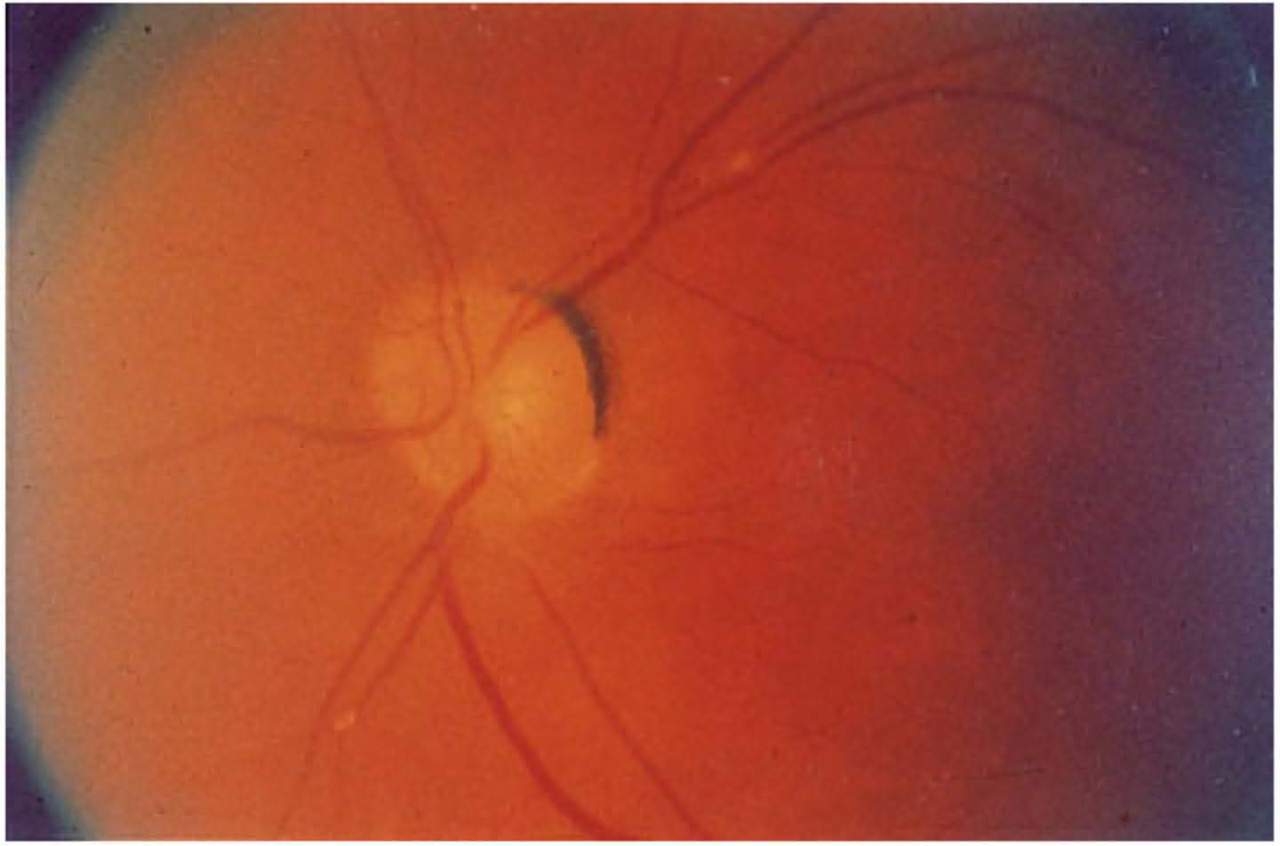 neurology internalmedicine step2
neurology internalmedicine step2 -
Amaurosis fugax: defining clinical feature?
- Brief, transient, unilateral vision loss
- Indicative of retinal ischemia from emboli
neurology internalmedicine step2. -
Hollenhorst plaque: description
- Yellow, refractile, cholesterol embolus visible in retinal arterioles
ophthalmology internalmedicine step2. -
Amaurosis fugax: immediate diagnostic study
- Emergent carotid duplex ultrasonography to evaluate source (usually ipsilateral carotid artery)
surgery internalmedicine step2. -
Glaucoma: typical clinical course and key sign
- Insidious, chronic course with progressive peripheral vision loss
- Hallmark: cupping of the optic disc
ophthalmology internalmedicine step2. -
Why glaucoma is unlikely for brief transient vision-loss episodes?
- Glaucoma causes chronic progressive peripheral loss, not brief transient episodes (amaurosis fugax)
ophthalmology internalmedicine step2. -
Serum antinuclear antibody (ANA) assay: appropriate use
- Useful to evaluate systemic autoimmune disorders (eg, systemic lupus erythematosus)
rheumatology internalmedicine step2. -
Autoimmune vasculitis causing retinal/ophthalmic ischemia: typical vision-loss pattern
- Vision loss is acute or subacute and progressive, not transient/episodic
rheumatology internalmedicine step2. -
Giant cell arteritis (GCA): relation to amaurosis fugax and testing
- GCA may present with amaurosis fugax
- ANA assay is insufficient; erythrocyte sedimentation rate (ESR) is commonly associated biomarker
rheumatology internalmedicine step2. -
Amaurosis fugax management: source most commonly evaluated where?
- Evaluate ipsilateral carotid artery as most common embolic source
surgery internalmedicine step2. -
Fundus finding and embolus correlation (visual aid)
- Fundus exam may show retinal embolus (Hollenhorst plaque)
ophthalmology neurology step2. -
What is the most likely diagnosis for a 47-year-old with 3 months of weight loss, epigastric fullness, painless hyperbilirubinemia, mild ALP/AST/ALT elevation, and 30-year smoking history?
Pancreatic cancer
internal_medicine surgery step2. -
internal_medicine surgery step2.
-
Why is CT abdomen with contrast preferred for suspected pancreatic cancer?
CT with contrast best evaluates pancreatic mass extent and metastases to guide resectability
internal_medicine surgery step2. -
What laboratory pattern indicates cholestasis in this case?
Elevated total bilirubin (6 mg/dL) with increased alkaline phosphatase
internal_medicine step2. -
Which clinical features are classic for pancreatic head carcinoma?
- Painless jaundice
- Unintended weight loss
- Epigastric fullness/mass
internal_medicine surgery step2. -
surgery internal_medicine step2.
-
When is a bone scan appropriate in oncology?
Bone scan for osteoblastic bone metastases (eg, prostate, breast)
internal_medicine step2. -
When are flat and upright abdominal x-rays useful?
Detect bowel obstruction (air-fluid levels) or free air from perforation
internal_medicine step2. -
When is a HIDA scan indicated?
HIDA scan for acute cholecystitis, gallbladder emptying dysfunction, cholelithiasis with cystic duct obstruction
internal_medicine step2. -
Which risk factors for pancreatic cancer are listed in the case text?
- Smoking
- Obesity
- Chronic pancreatitis
internal_medicine step2. -
internal_medicine surgery step2
-
internal_medicine step2
-
internal_medicine step2
-
radiology internal_medicine step2
-
surgery internal_medicine step2
-
Right upper quadrant ultrasonography: primary clinical use?
- Evaluate liver and gallbladder pathologies
radiology internal_medicine step2 -
Right upper quadrant ultrasonography: when might it show an enlarged gallbladder in pancreatic disease?
- If a pancreatic head mass restricts biliary outflow
radiology surgery step2 -
Mild alkaline phosphatase, ALT, AST elevations in suspected pancreatic cancer: next best diagnostic step?
- CT scan of the abdomen with contrast
internal_medicine radiology step2 -
Choice E (RUQ ultrasonography) vs CT abdomen with contrast: when is CT preferred?
- CT abdomen with contrast preferred for evaluating suspected pancreatic cancer
internal_medicine radiology step2 -
Right upper quadrant ultrasonography: when is RUQ US the correct initial test?
- When evaluating liver or gallbladder pathology (eg, cholecystitis, gallstones)
internal_medicine step2 -
Define heat stroke (core features)
- Hyperthermia with environmental heat exposure
- Neurologic dysfunction (eg, altered mental status to obtundation)
- Cardiovascular instability (eg, tachypnea, hypotension)
internal_medicine neurology step2. -
Distinguish heat stroke from heat exhaustion
- Heat stroke: neurologic symptoms present
- Heat exhaustion: similar signs but neurologic exam intact
internal_medicine step2. -
Primary pathophysiology of heat stroke causing organ injury
- Excessive core temperature → cardiovascular and neurologic dysfunction → peripheral vasodilation → tissue ischemia and multi-organ failure
internal_medicine step2. -
Laboratory abnormalities associated with heat stroke
- Hypernatremia, hyperchloremia, hyperkalemia
- ↑ BUN, creatinine, creatine kinase
internal_medicine step2. -
Initial management priorities for heat stroke
- Rapid cooling (fans or ice water) and continuous core temperature monitoring
- Support airway, breathing, circulation
internal_medicine emergency step2. -
Why is evaporative cooling the correct immediate therapy for environmental heat stroke?
- Directly reduces core temperature quickly and addresses underlying hyperthermia; paired with ABCs and core temp monitoring
internal_medicine step2. -
When is CT scan of the head appropriate in altered mental status?
- For suspected ischemic or hemorrhagic stroke to guide interventions (eg, tPA) or structural causes
neurology internal_medicine step2. -
When is norepinephrine indicated for hypotension in heat stroke?
- After fluid resuscitation if hypotension persists; vasopressors support BP but do not treat hyperthermia
internal_medicine step2. -
When is dantrolene the correct therapy (contrast with heat stroke)?
- Treats neuroleptic malignant syndrome or malignant hyperthermia from drugs/anesthesia; not indicated for environmental heat stroke
psychiatry internal_medicine step2. -
When is lumbar puncture appropriate in altered mental status?
- When central nervous system infection (eg, meningitis) is suspected and imaging allows safe LP; not for isolated heat stroke
internal_medicine neurology step2. -
emergency internal_medicine step2.
-
Supportive steps during cooling for heat stroke (monitoring)
- Continuous core temperature monitoring
- Airway management and circulatory support (IV fluids first for hypovolemia)
internal_medicine step2. -
Illustration: evaporative cooling slide (supplement)
See image for a slide illustration of cooling measures:
 internal_medicine emergency step2.
internal_medicine emergency step2. -
Heat stroke: core definition and immediate pathophysiology?
- Heat stroke: failure of thermoregulation due to high environmental heat/humidity causing uncontrolled hyperthermia and multi-organ dysfunction
internalmedicine emergency step2. -
Heat stroke: cardinal vital-sign and systemic features?
- Features: hyperthermia, tachycardia, tachypnea, hypotension, neurologic dysfunction
emergency internalmedicine step2. -
Heat stroke: major complications to anticipate?
- Complications: shock; rhabdomyolysis; disseminated intravascular coagulation (DIC)
internalmedicine emergency step2. -
Heat stroke: initial management priorities?
- Treatment: active cooling (fans or ice-water), continuous core-temperature monitoring, support airway/breathing/circulation
emergency internalmedicine step2. -
Bacterial meningitis: typical presenting symptoms?
- Symptoms: fever; severe headache; neck stiffness; altered mental status or obtundation
neurology infectiousdisease step2. -
Cerebrospinal fluid (CSF) profile in bacterial meningitis?
- CSF: ↑ leukocytes with neutrophil predominance; ↑ protein; ↓ glucose
neurology infectiousdisease step2. -
Lumbar puncture (LP): when is it useful?
- LP: useful for diagnosing meningitis and other infectious/inflammatory CNS disorders
neurology internalmedicine step2. -
Clinical distinction: heat stroke vs bacterial meningitis—key discriminating history?
- Distinguishing feature: recent exposure to extreme environmental heat favors heat stroke over meningitis
emergency internalmedicine step2. -
Why LP is less appropriate for patient with hyperthermia after heat exposure?
- Reason: hyperthermia from extreme environmental heat provides a more likely cause than meningitis, so LP is less indicated
internalmedicine emergency step2. -
Heat stroke: monitoring and support measures during treatment (supplemental image)?
- Monitor/support: continuous core-temperature monitoring; airway/breathing/circulation support
emergency internalmedicine step2. -
Phentermine: mechanism causing hypertension?
- Increases norepinephrine release → α-adrenergic vasoconstriction
psychiatry pediatrics step2. -
Hypertensive emergency: diagnostic threshold and requirement?
- BP > 180/120 mm Hg plus end-organ damage
internal_medicine neurology step2. -
Common presenting symptoms of sympathomimetic-induced hypertensive emergency?
- Headache
- Epistaxis
- Neurologic deficits
neurology pediatrics step2. -
Clinical features in the presented 15-year-old phentermine overdose case?
- Severe headache, chest pain
- BP 220/125 mm Hg, pulse 55/min, generalized hyperreflexia
pediatrics internal_medicine step2. -
Sodium nitroprusside: clinical role in sympathomimetic hypertensive emergency?
- Immediate IV vasodilator to reverse α-mediated vasoconstriction and lower BP
internal_medicine emergency step2. -
Sodium nitroprusside: described mechanism of action (as stated)?
- Releases nitrous oxide and acts as arterial and venodilator
internal_medicine step2. -
Phentolamine: role in sympathomimetic hypertensive emergency?
- α-adrenergic blocker option to treat catecholamine-mediated hypertension
internal_medicine step2. -
internal_medicine step2.
-
IV furosemide: when is it appropriate for hypertension?
- Diuresis for heart failure, cirrhosis, kidney disease; not for acute sympathomimetic vasoconstriction
internal_medicine step2. -
IV phenytoin: appropriate emergent indications?
- Status epilepticus and other seizures via Na+ channel blockade; not for hypertension
neurology step2. -
IV physostigmine: correct emergent indication?
- Anticholinergic toxicity reversal; not used for hypertensive emergency
psychiatry internal_medicine step2. -
IV verapamil: contraindication present in this case?
- Bradycardia present (pulse 55/min) → verapamil contraindicated due to AV conduction worsening
cardiology internal_medicine step2. -
Endotracheal intubation: indications relevant to this patient?
- Indicated for airway protection, apnea, hypoxemia, hypercarbia; not indicated here (no respiratory failure)
surgery pediatrics step2. -
Comparison: sodium nitroprusside versus verapamil in this overdose scenario?
- SNP: immediate arterial + venous vasodilation for severe hypertension
- Verapamil: slows AV node, contraindicated with bradycardia
cardiology internal_medicine step2. -
Sodium nitroprusside: illustration of use (slide image)?
- Use in sympathomimetic hypertensive emergency
 internal_medicine step2.
internal_medicine step2. -
internal_medicine step2
-
Phentermine: which vascular effect is counteracted by intravenous sodium nitroprusside?
- Vasoconstriction
internal_medicine step2 -
Atrial septal defect (ASD): key auscultatory findings?
- Fixed, widely split S2
- Grade 3/6 midsystolic murmur at 2nd left intercostal space
internal_medicine step2. -
Atrial septal defect (ASD): primary pathophysiology?
- Left-to-right atrial shunt → RA/RV volume overload → increased RV stroke volume
internal_medicine cardiology step2. -
Why does ASD cause a fixed, widely split S2?
- RV volume overload → delayed pulmonic valve closure → persistent wide split S2
internal_medicine cardiology step2. -
Uncorrected ASD: most important long-term complication?
- Pulmonary arterial hypertension from pulmonary vascular remodeling → possible shunt reversal (Eisenmenger) and cyanosis
internal_medicine cardiology step2. -
Why is pulmonary hypertension the correct long-term risk in ASD?
- Chronic left-to-right shunt increases pulmonary flow/pressure → pulmonary vascular remodeling → pulmonary arterial hypertension
internal_medicine cardiology step2. -
Cholestasis: typical cause and presentation?
- Cause: biliary obstruction (eg, pancreatic head tumor)
- Presentation: painless jaundice, anorexia
internal_medicine gastroenterology step2. -
Why is cholestasis unlikely in this young woman with ASD?
- No evidence of intra-abdominal mass or painless jaundice; clinical exam normal
internal_medicine step2. -
Budd-Chiari syndrome (hepatic vein thrombosis): common risk factors?
- Hypercoagulable states: pregnancy, antiphospholipid syndrome, protein C deficiency, malignancy
internal_medicine hepatology step2. -
Why is Budd-Chiari unlikely in this patient despite OCP use?
- OCPs increase clot risk but patient lacks other hypercoagulable signs; no hepatic symptoms given
internal_medicine step2. -
Hepatitis: common causes and presentation?
- Causes: viral, medication-induced, autoimmune, alcoholic
- Presentation: transaminitis, jaundice, RUQ pain
internal_medicine infectious_disease step2. -
Why is acute hepatitis unlikely in this patient?
- No heavy alcohol use, no offending medications, and no high-risk behaviors or hepatic symptoms
internal_medicine step2. -
Renovascular hypertension from fibromuscular dysplasia: typical patient and exam?
- Young female; renal artery beading on angiography; possible abdominal bruit
internal_medicine nephrology step2. -
Why is renovascular hypertension unlikely in this patient?
- No abdominal bruit and no other signs suggesting renal artery stenosis or fibromuscular dysplasia
internal_medicine nephrology step2. -
internal_medicine cardiology step2.
-
Why is systemic hypertension unlikely in this 22-year-old woman?
- Lacks typical risk factors (young age, no heavy alcohol use, no high-sodium diet noted); BP normal at 100/70 mm Hg
internal_medicine cardiology step2. -
Eisenmenger syndrome: defining features and consequence?
- Shunt reversal from long-standing pulmonary hypertension → cyanosis and right-to-left shunt physiology
internal_medicine cardiology step2. -
Midsystolic ejection murmur in ASD: mechanism?
- Increased RV stroke volume across pulmonary valve → physiologic ejection murmur
internal_medicine cardiology step2. -
ASD subtypes: commonest type and association with ostium primum?
- Ostium secundum = most common
- Ostium primum associated with Down syndrome
pediatrics internal_medicine step2. -
Illustration: ASD pathophysiology and auscultation (supplemental image)
See illustration:
 — image supplements ASD flow and auscultatory findingsinternal_medicine cardiology step2.
— image supplements ASD flow and auscultatory findingsinternal_medicine cardiology step2. -
Atrial septal defect (ASD): primary pathophysiologic effect on the pulmonic valve?
Increased blood flow through the pulmonic valve
pediatrics internalmedicine step2. -
pediatrics internalmedicine step2.
-
Atrial septal defect (ASD): which defect type is commonly associated with Down syndrome?
Ostium primum defect
pediatrics internalmedicine step2. -
Atrial septal defect (ASD): severe complication from long-standing uncorrected defect?
- Pulmonary hypertension
- Eisenmenger syndrome with reversal of the left-to-right shunt
pediatrics internalmedicine step2. -
Bacterial vaginosis: defining clinical features in adolescent with vaginal discharge
- Gray, thin, malodorous vaginal discharge
- Mild pruritus
- Recent antibiotic use
obgyn pediatrics step2. -
Bacterial vaginosis: primary pathophysiology and common organism
- Shift in vaginal flora → bacterial overgrowth
- Most common: Gardnerella vaginalis (gram-variable coccobacilli)
obgyn internalmedicine step2. -
Clue cells: microscopic definition
- Epithelial cells coated with bacteria
- Appear granular with irregular margins on wet mount
obgyn pediatrics step2. -
Bacterial vaginosis: diagnostic lab findings
- Vaginal pH > 4.5
- Fishy odor on KOH (whiff) test
- Clue cells on wet mount
obgyn internalmedicine step2. -
obgyn internalmedicine step2.
-
Bacterial vaginosis: sexual transmission and partner treatment policy
- Not considered an STI
- Do not treat asymptomatic sexual partners
obgyn pediatrics step2. -
Antibiotic exposure: role in bacterial vaginosis development
- Antibiotics disrupt normal lactobacilli → predispose to BV
obgyn internalmedicine step2. -
Chemical irritation (bubble baths): typical genital findings vs discharge
- External vulvar erythema, dryness, pruritus, possible excoriations
- Unlikely to cause gray malodorous vaginal discharge or clue cells
obgyn pediatrics step2. -
Latex allergy (condom): typical genital findings vs vaginal discharge
- Vulvar erythema, itching, dermatitis
- Unlikely to produce internal gray malodorous discharge or clue cells
obgyn pediatrics step2. -
Physiologic vaginal secretions: distinguishing features from pathologic discharge
- Small amounts, clear or white, variable with cycle
- Not malodorous; no clue cells
obgyn pediatrics step2. -
Trichomoniasis: typical clinical features differentiating from BV
- Green, frothy, malodorous discharge
- Pruritus, dysuria, dyspareunia, cervical erythema (strawberry cervix)
obgyn infectiousdisease step2. -
Comparison: BV versus Trichomonas key distinguishing points
- BV: gray thin discharge, clue cells, pH >4.5, fishy KOH
- Trichomonas: green frothy discharge, dysuria, cervical erythema
obgyn internalmedicine step2. -
Bacterial vaginosis: supportive image of wet mount (clue cells)
- Clue cells on wet mount: epithelial cells coated with bacteria
 obgyn pediatrics step2.
obgyn pediatrics step2. -
Bacterial vaginosis: what organism causes the condition?
- Gardnerella vaginalis (gram-variable, facultative anaerobic coccobacilli)
obgyn internal step2 -
Bacterial vaginosis: describe the typical vaginal discharge.
- Gray, thin, malodorous vaginal discharge
obgyn internal step2 -
obgyn internal step2
-
Bacterial vaginosis: what is the potassium hydroxide (KOH) finding?
- Fish-like odor on KOH (positive whiff test)
obgyn internal step2 -
obgyn internal step2
-
obgyn internal step2
-
Bacterial vaginosis: is it considered a sexually transmitted infection (STI)?
- No; bacterial vaginosis is not considered an STI
obgyn internal step2 -
obgyn internal step2
-
What is pubertal gynecomastia?
- Benign proliferation of glandular breast tissue in boys aged 12–14, often SMR stage 3
pediatrics step2. -
What pathophysiologic mechanism causes pubertal gynecomastia?
- Relative androgen/estrogen imbalance from peripheral conversion of androstenedione and testosterone to estrone/estradiol
internal_medicine step2. -
Typical physical exam features of pubertal gynecomastia?
- Tender, firm, mobile subareolar mass (~1 cm)
pediatrics step2. -
What is the expected result of laboratory studies in physiologic pubertal gynecomastia?
- Normal laboratory studies
internal_medicine step2. -
Management of physiologic pubertal gynecomastia in an otherwise healthy adolescent?
- Reassurance; most self-resolve; medical/surgical options (eg, aromatase inhibitors, liposuction) for symptoms
pediatrics surgery step2. -
Why is 'Puberty' the most likely cause of the 14-year-old boy's breast swelling?
- Age 12–14 and SMR stage 3 correspond to physiologic gynecomastia from increased estrogen via peripheral aromatization
pediatrics step2. -
When would SSRI-associated gynecomastia be the correct diagnosis?
- If gynecomastia appears after SSRI use and alternative causes excluded; note SSRIs are not generally associated with gynecomastia
psychiatry step2. -
How does male breast cancer usually differ on exam from benign gynecomastia?
- Malignancy tends to be fixed (not mobile) due to invasive growth; less likely in adolescent boys
surgery step2. -
When is marijuana a likely cause of gynecomastia and by what proposed mechanism?
- With recurrent use; proposed disruption of hepatic estrogen metabolism by THC causing increased estrogen
internal_medicine step2. -
Which clinical features suggest Klinefelter syndrome (seminiferous tubule dysgenesis) rather than pubertal gynecomastia?
- Learning disabilities, testicular atrophy, tall stature with long extremities
pediatrics step2. -
Physical exam illustration: subareolar tender breast mass — what diagnosis does this support?
- **Supports pubertal gynecomastia when age/SMR fit; exam: tender, firm, mobile subareolar mass
 **pediatrics step2.
**pediatrics step2. -
Anchor: Initial diagnostic step for 47-year-old with 6-month progressive low back pain without neurologic deficits or red flags?
- X-ray series of the lumbar spine
internal step2. -
Anchor: Pathophysiology components of degenerative disc disease?
- Cartilaginous endplates
- Annulus fibrosus
- Nucleus pulposus
neurology step2. -
Anchor: Mechanism causing loss of disc height in degenerative disc disease?
- Decreased nutrient diffusion from endplates + decreased nucleus pulposus water content → loss of disc height
neurology step2. -
Anchor: How do annulus fibrosus tears develop in degenerative disc disease?
- Repetitive axial forces on dehydrated disc → annular tears
orthopedics step2. -
neurology step2.
-
Anchor: Typical pain features of degenerative disc disease?
- Worse with flexion, Valsalva, coughing, or sneezing
internal step2. -
Anchor: Physical exam tests and signs to evaluate for radiculopathy?
- Straight-leg raise (positive = reproduction of leg pain)
- Sensory deficits, DTR changes, muscle weakness
neurology step2. -
Anchor: Red-flag features indicating possible cauda equina or conus medullaris syndrome requiring emergent surgery?
- Saddle anesthesia
- Bowel/bladder incontinence
- Lower extremity weakness
surgery step2. -
Anchor: Indication for MRI of the lumbar spine in low back pain?
- Acute neurologic deterioration or signs of myelopathy (eg, cauda equina/conus medullaris)
neurology step2. -
Anchor: Appropriate use of bone scan in back pain?
- Characterize concerning osseous lesion or detect osteoblastic metastases (eg, prostate, breast)
oncology step2. -
Anchor: Role of CT myelography versus MRI in spine imaging?
- CT myelography used historically for spinal cord evaluation after intrathecal contrast; largely replaced by MRI (better accuracy, noninvasive, no radiation)
radiology step2. -
Anchor: Conservative treatments for degenerative disc disease?
- NSAIDs
- Hot/cold compress, weight loss, activity modification, physical therapy
internal step2. -
Anchor: When to obtain initial imaging for low back pain?
- Initial imaging (x-ray) indicated for chronic pain without neurologic deficits or trauma to evaluate degenerative changes
internal step2. -
Anchor: Supplementary slide showing recommended initial test for chronic low back pain (image on answer)
Initial test: X-ray series of the lumbar spine
 internal step2.
internal step2. -
Cauda equina compression: core presenting features?
- Bilateral lower extremity weakness
- Abnormal deep tendon reflexes
- Bowel or bladder dysfunction
- Saddle anesthesia
neurology surgery step2. -
Cauda equina compression: common acute causes?
- Acute disc herniation
- Traumatic vertebral column fracture
- Pathologic vertebral fracture
neurology surgery step2. -
Initial imaging for suspected lumbar spine problem without neurologic deficits?
- Plain x-ray series of the lumbar spine
internal_medicine surgery step2. -
Role of MRI in acute lumbosacral compression when initial exam lacks deficits?
- MRI may be required later to guide therapy after plain x-rays
neurology radiology step2. -
Degenerative disc disease: primary pathophysiologic processes?
- Repetitive axial forces
- Decreased nutrient gradient
- Declining nucleus pulposus water content with aging
orthopedics internal_medicine step2. -
Degenerative disc disease: how annulus fibrosus tears form?
- Result from repetitive axial forces + declining nucleus pulposus hydration and nutrients
orthopedics surgery step2. -
Degenerative disc disease: typical symptom triggers?
- Pain worsens with flexion
- Pain with Valsalva, cough, or sneezing
internal_medicine neurology step2. -
Degenerative disc disease: first-line nonprocedural treatments (group 1)?
- NSAIDs
- Hot or cold compresses
internal_medicine pain step2. -
Degenerative disc disease: first-line nonprocedural treatments (group 2)?
- Weight loss
- Activity modification
- Physical therapy
internal_medicine rehabilitation step2. -
Imaging workflow for patient with lumbar complaint and no neurologic deficits: concise plan?
- Obtain plain x-rays first; consider MRI later if therapy guidance needed
radiology surgery step2. -
Supplemental image: presentation slide relevant to lumbar imaging and degenerative disc disease?
Slide image for review:
radiology internal_medicine step2. -
Membranous nephropathy: core nephrotic syndrome features?
- Proteinuria >3 g/day
- Edema
- Hypoalbuminemia
internal_medicine step2. -
Membranous nephropathy: key biopsy/immunofluorescence findings?
- Diffuse GBM thickening
- IgG along GBM (IF)
- Subepithelial electron-dense deposits
internal_medicine step2. -
internal_medicine step2.
-
Pathophysiology: why hypercholesterolemia occurs in nephrotic syndrome?
Liver increases lipoprotein synthesis to compensate for low serum oncotic pressure from urinary albumin losses
internal_medicine step2. -
ACE inhibitor therapy: mechanism slowing progression of membranous nephropathy?
ACE inhibitors ↓ angiotensin II → relative efferent arteriole dilation → ↓ glomerular filtration pressure → ↓ hyperfiltration injury
internal_medicine step2. -
Why is ACE inhibitor (eg, lisinopril) the correct choice for delaying renal progression in membranous nephropathy?
ACE inhibitor reduces intraglomerular pressure and hyperfiltration, delaying nephropathy progression
internal_medicine step2. -
High-protein diet: when would it be appropriate in kidney disease?
High-protein diet is not appropriate; kidney disease patients should generally avoid high protein to reduce glomerular injury
internal_medicine step2. -
High-potassium diet: when is it indicated in kidney disease?
High-potassium diet is inappropriate; patients with kidney disease generally should limit potassium
internal_medicine step2. -
Beta-blocker therapy (eg, metoprolol): when would it be preferred over ACE inhibitor for renal protection?
Beta-blockers treat arrhythmia/hypertension/CHF but do not reduce intraglomerular hyperfiltration and are not used to slow nephropathy progression
internal_medicine step2. -
Diuretic therapy: appropriate indication in membranous nephropathy?
Diuretics treat hypervolemia/edema; avoid if patient lacks volume overload because diuretics can reduce renal perfusion and worsen function
internal_medicine step2. -
Membranous nephropathy: summary preventive treatment principle for slowing progression?
Reduce intraglomerular pressure (eg, ACE inhibitors) to limit hyperfiltration injury
internal_medicine step2. -
Visual: membranous nephropathy features (illustration). What biopsy features are shown?
- Diffuse GBM thickening
- Subepithelial deposits (electron microscopy)
 internal_medicine step2.
internal_medicine step2. -
Osteoporosis trial result: what does a P-value of 0.047 indicate about chance?
P-value < 0.05 → result unlikely due to random chance
internal_medicine step2. -
Osteoporosis trial: how large was the absolute reduction in hip-fracture rate?
- 0.044 − 0.042 = 0.002 (0.2% absolute reduction)
internal_medicine step2. -
Why is the trial result statistically significant but not clinically significant?
Statistically significant (P<0.05) but absolute benefit only 0.2% → minimal individual benefit; NNT exceedingly high; unlikely to change practice or justify costs/risks
internal_medicine step2. -
When would 'results likely caused by chance' be a correct conclusion?
If P-value ≥ 0.05 (no statistical significance) → cannot exclude random chance
internal_medicine step2. -
Definition: placebo effect as described in the trial explanation
Beneficial effect from placebo due to patient belief, not from placebo's properties
internal_medicine step2. -
When could the placebo effect explain a trial difference?
When outcomes are subjective and patient belief can alter perceived benefit; not likely to explain objective fracture-rate reductions
internal_medicine step2. -
Why is 'inadequate power' unlikely for this osteoporosis trial?
Large sample: 19,916 participants over 3 years → study likely well powered to detect small differences
internal_medicine step2. -
What does 'clinical significance' require beyond statistical significance?
Benefit magnitude that alters practice and outweighs risks/costs
internal_medicine step2. -
Applicability: what does 'applicability' mean for a treatment effect?
Extent to which a study's observed treatment effect will reflect the effect in actual patients outside the study.
internalmedicine step2. -
Applicability: main factors that can affect whether study results apply to non-study patients?
- Similarity of baseline characteristics
- Demographics
- Clinical scenario and treatment
internalmedicine step2. -
Applicability example: elderly patient with osteoporosis on calcium and vitamin D — are study results likely applicable?
Yes; this patient closely reflects the elderly osteoporotic study population treated with calcium and vitamin D, so study results reasonably apply.
internalmedicine step2. -
Statistical power: what does 'power' describe?
Ability of a study to detect a difference between groups if one exists.
internalmedicine step2. -
Factors that may influence statistical power (small list)?
- Baseline incidence of outcome
- Population variance
- Magnitude of treatment effect
internalmedicine step2. -
When is 'inadequate power' a correct explanation for study findings?
When the study lacks ability to detect an existing difference (underpowered), making a true effect statistically undetected.
internalmedicine step2. -
Why is 'inadequate power' an incorrect explanation if the study was adequately powered?
Adequate power means the study could detect a difference; if a small-magnitude difference was found, inadequate power is not the cause.
internalmedicine step2. -
What does a conventional P-value cutoff of 0.05 indicate?
Result was unlikely to occur due to random chance (statistical significance threshold).
internalmedicine step2. -
How does statistical significance (P≤0.05) differ from clinical significance?
Statistical significance ≠ clinical significance; clinical significance requires likely change in practice and benefits that outweigh risks and costs.
internalmedicine step2. -
Study statement: Can power change the magnitude of an observed treatment effect?
No; power affects ability to detect a difference, not the magnitude of the detected difference.
internalmedicine step2. -
Visual: slide illustrating highlighted teaching points (useful as summary)
Illustration of applicability, power, and P-value concepts:
 internalmedicine step2.
internalmedicine step2. -
Define 'hematogenous osteomyelitis' in children (anchor: osteomyelitis presentation).
- Infection of bone/bone marrow from bloodstream causing pain, fever, inability to bear weight
pediatrics internalmedicine step2. -
Key clinical features of pediatric hematogenous osteomyelitis (anchor: clinical presentation).
- Fever
- Localized pain/tenderness
- Difficulty bearing weight or refusal to walk
pediatrics internalmedicine step2. -
Laboratory and imaging findings supporting osteomyelitis (anchor: diagnostics).
- Leukocytosis, elevated CRP
- MRI showing marrow edema
pediatrics internalmedicine step2. -
Most likely pathogen for hematogenous osteomyelitis in this 2-year-old (anchor: microbiology).
Staphylococcus aureus (most common cause in this age)
pediatrics infectiousdisease step2. -
Gram-stain clue pointing to Staphylococcus aureus (anchor: Gram stain interpretation).
Gram-positive cocci in clusters on blood culture Gram stain
pediatrics internalmedicine step2. -
First-line initial antibiotic choice for suspected MRSA/MSSA pediatric osteomyelitis (anchor: initial management).
Vancomycin (covers MRSA and MSSA pending sensitivities)
pediatrics infectiousdisease step2. -
Why ampicillin is inappropriate as initial monotherapy here (anchor: ampicillin limitation).
Ampicillin active vs some gram-positive/gram-negative but is not effective against MRSA
pediatrics internalmedicine step2. -
When would azithromycin be an appropriate choice (anchor: azithromycin spectrum)?
Macrolide primarily effective against some gram-positive organisms; not reliable for MRSA empiric therapy
pediatrics internalmedicine step2. -
Rationale for starting broad-spectrum therapy in suspected pediatric osteomyelitis (anchor: treatment principle).
Prompt broad antibiotics needed because hematogenous seeding can cause bacteremia and distant bone infection; tailor after culture sensitivities
pediatrics infectiousdisease step2. -
Other common pediatric osteomyelitis pathogens besides S. aureus (anchor: differential microbiology).
- Group A streptococci
- Streptococcus pneumoniae
- Haemophilus influenzae
pediatrics infectiousdisease step2. -
Why ceftriaxone/cefepime/rifampin were not chosen as initial therapy in this case (anchor: initial-choice logic).
Initial therapy must reliably cover MRSA; these agents do not reliably provide empiric MRSA coverage pending culture results
pediatrics internalmedicine step2. -
Osteomyelitis (pediatric): definition
Infection of bone and bone marrow; typically develops from hematogenous spread in children.
pediatrics infectious step2. -
pediatrics infectious step2.
-
Osteomyelitis (pediatric): other common bacteria (group 1)
- Streptococcus pyogenes (Group A streptococci)
- Streptococcus pneumoniae
pediatrics infectious step2. -
pediatrics infectious step2.
-
Initial antibiotic choice for suspected pediatric osteomyelitis with possible MRSA
Vancomycin — effective against MRSA and MSSA; appropriate initial therapy.
pediatrics internalmedicine step2. -
Why ceftriaxone or cefepime alone is NOT initial monotherapy for suspected MRSA osteomyelitis
Ceftriaxone/cefepime cover gram-positive and gram-negative bacteria but are not effective against MRSA.
pediatrics infectious step2. -
When is cefepime specifically useful in bone infection coverage?
Cefepime adds Pseudomonas coverage (unlike ceftriaxone).
pediatrics infectious step2. -
Role of combining vancomycin with ceftriaxone/cefepime in osteomyelitis
Combination may be used to broaden coverage (vancomycin for MRSA plus ceftriaxone/cefepime for gram-negatives).
pediatrics internalmedicine step2. -
Azithromycin in suspected MRSA osteomyelitis: appropriateness
Azithromycin is not effective against MRSA and is not appropriate as initial therapy for suspected MRSA osteomyelitis.
pediatrics infectious step2. -
Rifampin: mechanism and limits relevant to osteomyelitis
Rifampin inhibits bacterial RNA polymerase; active vs mycobacteria and some gram-positives but not effective as sole initial therapy for MRSA.
pediatrics infectious step2. -
Pathogenesis anchor: how pediatric osteomyelitis usually arises
Hematogenous seeding of bone and marrow in pediatric patients.
pediatrics surgery step2. -
Supplementary: slide image for osteomyelitis teaching (illustration only)
Supplementary figure illustrating teaching points.
 pediatrics internalmedicine step2.
pediatrics internalmedicine step2. -
Rheumatic mitral valve disease: what is the pathophysiology linking group A strep to progressive valve damage?
- Molecular mimicry after group A streptococcal infection → progressive inflammatory damage to valves → fibrosis and calcification
internal_medicine step2. cardiology -
Rheumatic fever: key extra-cardiac clinical findings
- Joint inflammation
- Subcutaneous nodules
- Erythema marginatum
- Sydenham chorea
internal_medicine step2. infectious -
Rheumatic mitral valve disease: typical acute vs chronic valve dysfunction
- Acute: mitral insufficiency
- Chronic (later): mitral stenosis
internal_medicine step2. cardiology -
Mitral stenosis: classic auscultatory and complication features
- Diastolic rumble at apex radiating to axilla
- Can cause left atrial enlargement, pulmonary edema, atrial fibrillation/flutter
internal_medicine step2. cardiology -
Why rheumatic mitral valve disease best explains this patient: 32-year-old with 6 months dyspnea, irregular tachycardia, holosystolic murmur and diastolic rumble at apex, AF, RVH?
- Mitral valve disease from rheumatic damage causes diastolic murmur at apex, LA enlargement → AF and pulmonary congestion; fits progressive rheumatic mitral stenosis
internal_medicine step2. cardiology -
Aortic stenosis from calcified tricuspid aortic valve: when is this the usual cause and typical findings?
- Common in elderly due to trileaflet calcification
- Symptoms: exertional syncope, angina, dyspnea
- Murmur: crescendo-decrescendo systolic at right upper sternal border
internal_medicine step2. surgery -
Bicuspid aortic valve calcification: typical patient group and mechanism
- Younger patients (than tricuspid) due to abnormal leaflet geometry → turbulent shear, earlier calcification
internal_medicine step2. pediatrics -
Atrial septal defect (ASD): hemodynamic effects and auscultatory clues when ASD is the correct diagnosis
- Left→right shunt → RA/RV volume overload, delayed pulmonic valve closure → fixed split S2 and low-grade ejection murmur
- Chronic → pulmonary HTN, possible Eisenmenger with cyanosis
internal_medicine step2. cardiology -
Ventricular septal defect (VSD): classic murmur and typical location heard
- Holosystolic murmur best heard at left lower sternal border
internal_medicine step2. pediatrics -
Infective endocarditis (Staphylococcus aureus or viridans): typical presenting features that support this diagnosis
- Fever
- New cardiac murmur
- Fatigue
- Septic embolic phenomena
internal_medicine step2. infectious -
Slide image: supporting visual summary of exam item (use as reference only)
 - Visual summary of rheumatic mitral disease, murmurs, ASD/VSD, aortic stenosis, and endocarditis featuresinternal_medicine step2. cardiology
- Visual summary of rheumatic mitral disease, murmurs, ASD/VSD, aortic stenosis, and endocarditis featuresinternal_medicine step2. cardiology -
internalmedicine cardiology step2
-
Mitral stenosis — classic auscultatory findings?
- Opening snap
- Diastolic rumble loudest at cardiac apex
internalmedicine cardiology step2 -
Cause: Long-term complication that classically produces mitral stenosis?
Rheumatic heart disease from group A streptococcal infections
internalmedicine infectiousdisease step2 -
Complications of severe mitral stenosis?
- Left atrial enlargement
- Cardiogenic pulmonary edema
- Atrial fibrillation/flutter
internalmedicine cardiology step2 -
Why is infective endocarditis unlikely for a patient with 6 months of symptoms?
Endocarditis usually presents acutely/subacutely; 6 months untreated would likely be fatal
internalmedicine infectiousdisease step2 -
When would endomyocarditis/myocarditis be the correct diagnosis?
In inflammatory or postviral syndromes with raised troponin, ECG changes, and possible heart-failure symptoms; presentation is typically acute
internalmedicine cardiology step2 -
Why is pericarditis an unlikely diagnosis for this patient?
Pericarditis causes sharp chest pain worse when supine, better sitting up; ECG shows diffuse ST elevation and PR depression; patient lacks these features and murmur/ECG are inconsistent
internalmedicine cardiology step2 -
Pericarditis — common causes and ECG pattern?
Causes: viral infection, SLE, tuberculosis, lymphoma, post-MI ECG: diffuse ST elevation and PR depression
internalmedicine rheumatology step2 -
Illustration: slide with highlighted teaching points — what image shows?
Image: presentation slide with highlighted clinical teaching pointsinternalmedicine education step2 -
Knee injury randomized trial with 500 randomized to operative (400 received) and 500 randomized to conventional (50 received): What is the primary study-design concern?
- Lack of intention-to-treat (ITT) analysis
surgery internalmedicine step2. -
Definition: What is intention-to-treat (ITT) analysis?
- Include all randomized subjects in the group originally assigned regardless of treatment actually received
internalmedicine surgery step2. -
Per-protocol analysis: how does it differ from ITT?
- Analyzes subjects according to the treatment actually received rather than original randomization
internalmedicine surgery step2. -
Why is lack of ITT analysis problematic in the knee trial described?
- Excluding randomized subjects introduces bias and reduces benefits of randomization, risking erroneous conclusions
surgery internalmedicine step2. -
When would 'Inadequate randomization' be the correct concern in a trial?
- When randomization method fails to account for or balance important factors/comorbidities that affect outcome
internalmedicine surgery step2. -
When is 'Inappropriate control group' (placebo) the correct concern?
- When an effective treatment exists or placebo use could cause harm; use standard-of-care control instead
internalmedicine surgery step2. -
When is 'Short follow-up duration' a valid trial concern?
- When short follow-up may miss late complications or fail to show durability of benefits; appropriateness depends on condition
internalmedicine surgery step2. -
Is 'Small sample size' the primary problem in the described knee trial?
- No. The trial enrolled 1000 patients, so small sample size is not the main concern
internalmedicine surgery step2. -
Study design: What is the effect of a 'small sample size' on statistical power?
- 'Small sample size' reduces statistical power, lowering ability to detect true differences between groups
internal step2. -
Clinical trial: Name baseline factors that influence statistical power (grouped).
- Baseline incidence of outcome
- Population variance
internal step2. -
Clinical trial: Name treatment-related factors that influence statistical power (grouped).
- Magnitude of treatment effect
- Likelihood of type I and type II errors
internal step2. -
Study planning: Is enrolling 1000 participants generally adequate for statistical power?
- Yes; in most instances enrollment of 1000 provides adequate statistical power
internal step2. -
Intention-to-treat (ITT): What is the ITT analysis rule for randomized subjects?
- Include all randomized subjects in analysis in the group to which they were originally randomized regardless of received treatment
internal step2. -
ITT rationale: What is the consequence of excluding randomized subjects from analysis?
- Excluding randomized subjects introduces bias and reduces prognostic benefit of randomization
internal step2. -
ITT benefit: What biases does ITT help limit and what integrity does it preserve?
- Preserves randomization integrity
- Limits attrition bias
internal step2. -
Intention-to-treat (ITT): Illustrative slide (supporting image on answer side).
- ITT = include all randomized by original group; preserves randomization and limits attrition bias
 internal step2.
internal step2. -
Anchor: Oncology unit medication errors — what root cause was identified?
- Look-alike medication packaging causing inadvertent antibiotic/chemotherapy swaps
internal_medicine step2. -
Anchor: Correct intervention to prevent look-alike vial errors in oncology unit?
- Repackage medications so containers are distinct (pharmacy-level packaging change)
internal_medicine step2. -
Anchor: Why is repackaging distinct containers the best fix for repeated look-alike medication errors?
- Targets systems-level cause identified by RCA; removes visual similarity that led to errors
internal_medicine step2. -
Anchor: Root cause analysis (RCA) — concise definition?
- Multidisciplinary process to define/analyze problems and design corrective actions based on analysis
internal_medicine step2. -
Anchor: Staff interviews — role in RCA?
- Staff interviews are a common RCA strategy to identify causes of adverse events
internal_medicine step2. -
Anchor: Option B ('Remove the antibiotic from formulary') — why is this incorrect here?
- Unnecessary and restricts effective antibiotic choices; repackaging suffices
internal_medicine step2. -
Anchor: Option C ('Require continuing education for nurses') — when would this be appropriate?
- Appropriate if errors result from knowledge/skill deficits rather than systems-level packaging similarity
internal_medicine step2. -
Anchor: Option D ('Suspend nurses involved') — why is suspension incorrect here?
- Blames individuals for system error; discourages reporting and hides problems
internal_medicine step2. -
Anchor: Option E ('No intervention likely helpful') — why is this incorrect here?
- RCA identified a modifiable cause (packaging); targeted repackaging is likely to prevent future errors
internal_medicine step2. -
Anchor: Common predictable cause of medication errors — what is it?
- Different medications appearing similar (look-alike packaging)
internal_medicine step2. -
Anchor: Example of a targeted corrective action for look-alike vials — what might be done by pharmacy?
- Repackage or relabel vials so appearance and containers are distinct
 internal_medicine step2.
internal_medicine step2. -
Squamous cell carcinoma of the lung: key paraneoplastic metabolic abnormality?
Hypercalcemia due to paraneoplastic parathyroid hormone-related peptide (PTHrP) production.
internal_medicine step2. -
Squamous cell carcinoma of the lung: typical gross/clinic location and radiographic feature?
Central location with pulmonary cavitations.
internal_medicine step2. -
Squamous cell carcinoma histology: characteristic findings?
- Polygonal cells with intercellular bridges
- Eosinophilic cytoplasm
- Keratin pearls
- Extensive necrosis
internal_medicine step2. -
internal_medicine step2.
-
internal_medicine step2.
-
Why squamous cell carcinoma is the correct diagnosis for a 3-cm central lung mass with hypercalcemia in a long-term smoker?
Smoking risk + central mass + hypercalcemia from PTHrP + squamous histologic features point to squamous cell carcinoma.
internal_medicine step2. -
Adenocarcinoma of the lung: typical patient profile and location?
More common in nonsmokers and females; peripheral lung location.
internal_medicine step2. -
internal_medicine step2.
-
Large cell carcinoma of the lung: defining histology and typical location?
Highly anaplastic, lacks glandular/squamous/neuroendocrine features; most often peripheral.
internal_medicine step2. -
Small cell carcinoma of the lung: cell type and distinguishing paraneoplastic syndromes?
- Neuroendocrine tumor of small dark blue cells
- Paraneoplastic: Cushing (ACTH), SIADH, Lambert-Eaton
internal_medicine step2. -
Small cell carcinoma histology distinctive microscopic appearance?
Small dark blue tumor cells with high nuclear-to-cytoplasm ratio and lacking nucleoli.
internal_medicine step2. -
Melanoma: typical primary lesion features and common metastatic sites?
- Primary: asymmetric, irregular borders, variable color, >6 mm, rapid change
- Metastases commonly to lung, brain, liver, skin
internal_medicine step2. -
Imaging/biopsy illustration for confirming lung cancer diagnosis (supplementary image)?
Diagnosis by chest x-ray and biopsy. Image:
 internal_medicine step2.
internal_medicine step2. -
Which primary lung cancers are typically centrally located?
- Squamous cell carcinoma of the lung
- Small cell carcinoma of the lung
internalmedicine step2 -
internalmedicine step2
-
What paraneoplastic syndrome is associated with squamous cell carcinoma of the lung?
- Hypercalcemia from parathyroid hormone-related peptide (PTHrP) production
internalmedicine step2 -
internalmedicine step2
-
internalmedicine step2
-
What is the typical timing of detection and its impact on prognosis for primary lung cancer?
- Often detected once metastatic → prognosis poor
internalmedicine step2 -
Diagnostic illustration for primary lung cancer (supplementary): what imaging and tissue test are used?
- Imaging: chest x-ray
- Tissue: biopsy
internalmedicine step2 -
Diagnosis: 62-year-old with 2 days nausea, severe abdominal pain, prior partial gastrectomy; CT shows target sign: what is the most likely diagnosis?
Intussusception
surgery internal_medicine step2. -
Pathophysiology: What causes intussusception? (anchor: intussusception)
Telescoping of one bowel segment into adjacent segment causing traction on mesenteric vessels → hypoperfusion, inflammation, hemorrhage, obstruction
surgery step2. -
Intussusception lead points: Name common pathologic lead points that precipitate intussusception.
- Lymphoid hyperplasia / lymphadenopathy
- Meckel diverticulum
- Adhesion, stricture, or malignancy
pediatrics surgery step2. -
Clinical features: What are typical symptoms of intussusception in adults? (anchor: intussusception symptoms)
- Colicky abdominal pain
- Nausea/vomiting
- Possible bloody mucoid stools
internal_medicine surgery step2. -
Imaging: What CT/US signs confirm intussusception? (anchor: intussusception imaging)
- Target sign on transverse imaging
- Telescoping bowel segments on longitudinal views
radiology surgery step2. -
Management: How does adult intussusception treatment differ from pediatric? (anchor: intussusception management)
- Adults: usually require surgical intervention
- Children: often treated with air or contrast enema
surgery pediatrics step2. -
When is bacterial small-bowel overgrowth the correct diagnosis? (anchor: bacterial overgrowth features)
Chronic impaired peristalsis → bacterial proliferation causing malabsorption, diarrhea, bloating, chronic pain; diagnosis via hydrogen breath test; responds to antibiotics
internal_medicine infectious_disease step2. -
When is intestinal volvulus the correct diagnosis? (anchor: volvulus features)
Twisting of bowel mesentery causing large-bowel obstruction; classic coffee-bean appearance on x-ray and marked bowel distension; risk of necrosis if untreated
surgery internal_medicine step2. -
When is jejunal enteritis the correct diagnosis? (anchor: jejunal enteritis features)
Mucosal infection/inflammation producing nausea, vomiting, cramping, diarrhea; may have fever or bloody stools; CT shows mucosal inflammatory changes but not target sign
infectious_disease internal_medicine step2. -
When are small-bowel adhesions the correct diagnosis? (anchor: small-bowel adhesions features)
History of prior intra-abdominal surgery → adhesions causing small-bowel obstruction (partial or complete) with bowel dilatation; most common SBO cause postop
surgery internal_medicine step2. -
Differentiation: How to distinguish intussusception from small-bowel adhesions on CT? (anchor: imaging differentiation)
- Intussusception: target sign, telescoping segments
- Adhesions: SBO pattern with transition point and dilated proximal bowel but no target sign
radiology surgery step2. -
Clinical context: Why could prior partial gastrectomy predispose an adult to intussusception? (anchor: postop risk)
Prior abdominal surgery can create lead points (adhesions/structural changes) that trigger bowel telescoping during peristalsis
surgery internal_medicine step2. -
surgery internalmedicine step2.
-
surgery radiology step2.
-
Why does absence of dilated small bowel loops on CT argue against SBO?
- Lack of dilated loops + air-fluid levels makes classic SBO imaging absent, reducing likelihood of SBO
surgery internalmedicine step2. -
surgery internalmedicine step2.
-
surgery internalmedicine step2.
-
Intussusception: pathophysiology (anchor: Intussusception)?
- One bowel segment telescopes into adjacent segment
pediatrics surgery step2. -
Intussusception: classic clinical features?
- Colicky abdominal pain, nausea/vomiting, possible bloody mucoid stools
pediatrics internalmedicine step2. -
Imaging signs of intussusception on CT or ultrasound?
- Longitudinal: telescoping bowel segments
- Transverse: 'target sign'
radiology pediatrics step2. -
Clinical decision: When would exploratory laparotomy be indicated for bowel obstruction?
- Complete obstruction or complicated partial obstruction
surgery internalmedicine step2. -
Interpretation task: Does this CT image support SBO? (anchor: CT abdomen)
Review for dilated small bowel loops and multiple air-fluid levels; absence of these findings argues against SBO
radiology surgery step2. -
CT example (anchor: CT abdomen image): view the image for landmarks relevant to obstruction.
- Use image to assess loop dilation and air-fluid levelsradiology surgery step2. -
Anaphylaxis: core pathophysiology?
- IgE-mediated mast cell/basophil activation → histamine and cytokine release → acute inflammation and widespread vasodilation
pediatrics step2. -
internal_medicine step2.
-
Anaphylaxis: organ systems commonly affected?
- Cardiovascular
- Respiratory
- Gastrointestinal
- Integumentary
emergency step2. -
Anaphylaxis: key presenting symptoms from each system (short)?
- Respiratory: bronchospasm, dyspnea, wheeze, stridor
- Skin: urticaria, flushing
- Cardiovascular: hypotension, tachycardia
- GI: nausea, vomiting
pediatrics step2. -
Stridor in anaphylaxis: clinical significance?
Stridor indicates glottic/subglottic angioedema and warns of impending airway loss
surgery step2. -
Initial management of anaphylaxis with hypotension, urticaria, stridor?
Urgent administration of epinephrine first
emergency step2. -
Why is epinephrine the first treatment in anaphylaxis?
Epinephrine causes vasoconstriction and reduces airway edema, reversing hypotension and airway obstruction
internal_medicine step2. -
Role of antihistamines in anaphylaxis?
Antihistamines are adjunctive therapy but should follow epinephrine
internal_medicine step2. -
Role of IV fluids in anaphylaxis?
IV fluids support intravascular volume for perfusion but follow epinephrine
internal_medicine step2. -
When is endotracheal intubation indicated in anaphylaxis?
If stridor or airway edema persists or worsens despite epinephrine, perform urgent intubation by most experienced provider
anesthesia step2. -
Risks/considerations for intubation in anaphylaxis?
Upper airway edema makes intubation difficult; may require surgical airway if intubation fails
surgery step2. -
Correct answer justification: why 'administration of epinephrine' is preferred over hospital admission alone?
Admission alone delays urgent reversal of vasodilation and airway edema; epinephrine must be given immediately to prevent shock and airway obstruction
pediatrics step2. -
When would antihistamine alone be appropriate for allergic reaction?
Antihistamine alone is only for mild, non-anaphylactic urticaria without respiratory or cardiovascular compromise
internal_medicine step2. -
Use of the provided image as illustration for airway edema?
Image: presentation slide (illustration only)
 emergency step2.
emergency step2. -
What is the pathophysiology of anaphylaxis?
Mast cell and basophil degranulation → acute multisystem inflammation and vasodilation
internal_medicine step2. -
pediatrics step2.
-
What are the main cutaneous/oral features of anaphylaxis?
- Urticaria
- Flushing
- Edematous lips and tongue
allergy step2. -
What are the main gastrointestinal and hemodynamic features of anaphylaxis?
- Nausea and emesis
- Hypotension with tachycardia
emergency step2. -
internal_medicine step2.
-
What are the next immediate adjunct treatments after epinephrine in anaphylaxis (group 1)?
- Antihistamines
- Bronchodilators
- Glucocorticoids
internal_medicine step2. -
What supportive measure is given after epinephrine and adjunct medications in anaphylaxis (group 2)?
- Fluids (intravenous) for hypotension
critical_care step2. -
Describe a concise treatment sequence for anaphylaxis.
- Epinephrine (urgent)
- Antihistamines, bronchodilators, glucocorticoids
- IV fluids
emergency step2. -
Diagnosis: Which eating disorder fits a 24-year-old with weekly binge eating and daily laxative purging, BMI 21, no vomiting?
- Bulimia nervosa (binge-eating with purging)
psychiatry step2. -
Pathophysiology: How does chronic laxative overuse cause metabolic acidosis?
- Loss of bicarbonate in stool → non-anion gap metabolic acidosis
internalmedicine step2. -
Pathophysiology: Mechanisms producing hypokalemia with chronic laxative abuse?
- Direct K+ loss in stool
- Hypovolemia → ↑aldosterone → renal K+ secretion
nephrology step2. -
Clinical feature: What orthostatic vital sign changes indicate hypovolemia in this patient?
- Supine 80/min → standing 90/min; BP supine 120/80 → standing 80/55; light-headedness on standing
internalmedicine step2. -
Diagnostics: Which laboratory pattern matches laxative-induced metabolic acidosis with hypokalemia (correct answer choice)?
- Serum K+ 3 mEq/L; ABG: pH 7.3, PCO2 30 mm Hg, HCO3- 14 mEq/L, PO2 90 mm Hg
internalmedicine step2. -
Why choice A would be correct: When does hyperkalemia with metabolic acidosis and respiratory compensation occur?
- Renal failure or acute acid load causing decreased K+ excretion → hyperkalemia + metabolic acidosis with respiratory compensation
nephrology step2. -
Why choice B would be correct: When does hypokalemia with metabolic alkalosis occur?
- Prolonged vomiting or diuretic use → loss of H+ and volume → metabolic alkalosis with hypokalemia via aldosterone
internalmedicine step2. -
Why choice D is incorrect: What does normal serum K+ and normal pH indicate?
- Normal electrolyte/acid-base status; not consistent with chronic laxative-induced stool losses causing pH/K+ abnormalities
internalmedicine step2. -
Why choice E would be correct: When is respiratory alkalosis with near-normal K+ seen?
- Hyperventilation (eg, anxiety, pain) → low PCO2 → respiratory alkalosis; K+ often near normal
pulmonology step2. -
Management: Immediate treatment priorities for bulimia nervosa with laxative-induced hypovolemia/hypokalemia?
- Correct volume depletion and electrolytes
- Start combined medical + psychiatric therapy (behavioral + pharmacologic)
psychiatry internalmedicine step2. -
Diagnostic distinction: How to differentiate laxative-induced acid-base disorder from vomiting-induced disorder?
- Laxatives → non-anion gap metabolic acidosis (low HCO3-)
- Vomiting → metabolic alkalosis (high HCO3-)
internalmedicine step2. -
Supplementary: Slide illustrating teaching points about laxative abuse and labs (image on answer side).
- Illustration:
- Content: laxative overuse → HCO3- loss, hypokalemia, hypovolemia signs, treat fluids/electrolytes + psychiatric care
psychiatry step2. - Illustration:
-
Disease: Bulimia nervosa — core behavioral features?
- Recurrent uncontrolled binge eating
- Compensatory purging (vomiting, laxatives, diuretics)
psychiatry step2 -
internal step2
-
Anchor: Laxative overuse — typical acid–base disturbance?
Metabolic acidosis due to stool bicarbonate loss
internal step2 -
Anchor: Laxative-induced hypokalemia — link to acid–base status?
Potassium wasting in stool occurs together with bicarbonate loss → hypokalemia + metabolic acidosis
internal step2 -
Anchor: Laxative overuse — effect on respiration?
Does NOT directly alter respiration; causes metabolic pH derangements instead
internal step2 -
internal psychiatry step2
-
Anchor: Vomiting vs laxative overuse — distinguishing acid–base effects?
- Vomiting → metabolic alkalosis (loss of acid)
- Laxatives → metabolic acidosis (loss of bicarbonate)
internal step2 -
Anchor: Compensatory purging options in bulimia (three main)?
- Self-induced vomiting
- Laxative overuse
- Diuretic overuse
psychiatry step2 -
Anchor: Image — visual slide of highlighted teaching point (supplement)
Slide illustrates the teaching that laxative overuse causes K+ and HCO3− loss leading to hypokalemic metabolic acidosisinternal step2 -
Gentamicin: primary nephrotoxicity prevention measure when given IV for sepsis/UTI?
- Measure plasma aminoglycoside trough concentrations to avoid supratherapeutic levels and reduce nephrotoxicity
internalmedicine renal infectious step2. -
Gentamicin: mechanism of synergy with beta-lactams (eg, piperacillin-tazobactam)?
- Aminoglycosides + penicillins produce stronger combined bactericidal effect (synergy)
infectious internalmedicine step2. -
Gentamicin: major toxicities relevant to a 67-year-old with sepsis?
- Ototoxicity, nephrotoxicity, neurotoxicity
renal internalmedicine step2. -
Trough concentration: timing and meaning for aminoglycoside dosing?
- Trough = serum level immediately before next dose; reflects nadir after tissue redistribution and metabolism
pharmacology internalmedicine step2. -
Initial management of septic UTI with hypotension and CVA tenderness?
- IV fluids + broad-spectrum antibiotics (eg, piperacillin-tazobactam + gentamicin) immediately
internalmedicine infectious step2. -
Central venous pressure (CVP) measurement: when is it used clinically?
- Estimate right atrial pressure/preload; used to assess volume status in shock
surgery internalmedicine step2. -
CVP measurement: when would CVP likely be decreased?
- Distributive shock (eg, septic shock) causes decreased CVP due to vasodilation and low preload
internalmedicine criticalcare step2. -
Piperacillin-tazobactam: role in urosepsis and nephrotoxicity risk?
- Covers gram-negative rods and anaerobes; needed for urosepsis; generally less nephrotoxic than gentamicin
infectious internalmedicine step2. -
When is discontinuation of piperacillin-tazobactam appropriate in sepsis?
- Only if alternative narrower therapy available or allergic/toxic effect identified; not initial step in urosepsis
infectious internalmedicine step2. -
Bicarbonate therapy: appropriate indication in septic patient?
- Severe metabolic acidosis; not indicated without diagnosed metabolic acidosis
internalmedicine criticalcare step2. -
Low-dose dopamine: typical clinical use compared with norepinephrine?
- Used for cardiogenic shock/advanced heart failure; norepinephrine preferred initial vasopressor for septic shock
cardiology internalmedicine step2. -
Why measuring gentamicin trough is correct choice to reduce acute renal failure risk?
- Trough monitoring prevents supratherapeutic gentamicin levels, lowering nephrotoxicity risk during IV aminoglycoside therapy
renal pharmacology step2. -
Image: Urosepsis with right CVA tenderness — which supportive therapy is essential before vasopressors?
- IV fluids are immediate therapy for hypotension in septic UTI; image for illustration:
internalmedicine infectious step2. - IV fluids are immediate therapy for hypotension in septic UTI; image for illustration:
-
internalmedicine pharmacology step2. pediatrics
-
Gentamicin: clinical purpose of measuring trough concentration?
- Predict and help prevent nephrotoxicity
internalmedicine pharmacology step2. pediatrics -
Screening: Which preventive test is most appropriate now for a 47-year-old obese woman (BMI 33) to detect type 2 diabetes?
Measure fasting serum glucose or hemoglobin A1c now
internalmedicine obgyn step2. -
Rationale: Why screen for diabetes in adults aged 35–70 who are overweight/obese?
Overweight/obese adults 35–70 have recommended fasting glucose or A1c testing to detect type 2 diabetes early and reduce morbidity/mortality
internalmedicine step2. -
Pap smear: When is cervical cancer screening recommended for a 47-year-old woman with prior normal Pap smears?
Pap smear every 3 years or every 5 years with normal HPV cotesting; annual Pap not indicated
obgyn step2. -
DEXA scan: When is osteoporosis screening indicated instead of now for this 47-year-old premenopausal woman?
DEXA screening recommended ≥65 years or postmenopausal with major risk factors (eg, low weight, chronic glucocorticoids); not routine premenopausal
internalmedicine obgyn step2. -
ECG screening: When is a resting ECG the most appropriate screening test in asymptomatic adults like this patient?
Routine ECG not indicated for asymptomatic low-risk adults; use when symptoms or specific cardiovascular concerns exist
cardiology internalmedicine step2. -
Mammography: What is the recommended screening interval relevant to a 47-year-old woman?
Begin breast cancer screening between ages 40–50; intervals vary by guideline (eg, annually or biennially); mammography every 3 years is not standard
obgyn internalmedicine step2. -
Comparison: Why is fasting glucose/A1c preferred now over Pap smear, DEXA, ECG, or mammography for this patient?
Patient is 47 and obese (BMI 33): diabetes screening age/risk criteria met; other tests either not due (Pap), not indicated (DEXA premenopausal), unnecessary routinely (ECG), or interval/guideline-dependent (mammography)
internalmedicine obgyn step2. -
Guidelines summary: Which two screening categories encompass most adult preventive recommendations mentioned?
Cardiovascular risk assessment and cancer screening
internalmedicine step2. -
Illustration: Where to find recommended screening example for overweight 35–70-year-olds (image)?
Guideline slide showing diabetes screening recommendation:
 internalmedicine step2.
internalmedicine step2. -
Baseline ECG screening: When is an ECG indicated?
- When cardiovascular symptoms are present (eg, exertional chest pain, dyspnea, palpitations)
- When electrolyte disturbance or medication side effects suspected
- To evaluate resting angina
internal step2. -
Baseline ECG screening in asymptomatic adults: why is it not recommended?
- Inconsistent abnormal findings in asymptomatic people and can be normal in existing disease
- Leads to unnecessary testing and potential harm
internal step2. -
When is screening mammography routinely recommended by USPSTF?
- Every 1–2 years for patients >50 years
obgyn step2. -
Breast cancer screening for patients aged 40–49 years: what is the recommendation?
- Shared decision-making between patient and physician; decision depends on balance of benefits vs risks
obgyn step2. -
Why is mammography every 3 years incorrect for a 47-year-old patient?
- 47-year-old falls in 40–49 group where screening is a shared decision; USPSTF recommends 1–2 years for >50, not routine 3-year interval
obgyn step2. -
Screening for type 2 diabetes mellitus: which patients should be screened?
- Overweight or obese patients aged 35–70 years using fasting glucose or hemoglobin A1c
internal step2. -
Preventive care screening decisions: what factors determine recommendations?
- Patient sex, age, and other risk factors determine screening recommendations
internal step2. -
Illustration: Which screening topic is highlighted in the slide?
- Slide illustrates preventive-screening recommendations (eg, ECG, mammography, diabetes screening)
internal step2. -
Restless legs syndrome (RLS): core diagnostic features?
- Unpleasant leg sensations at rest or during sleep
- Partial relief with movement
- Causes distress or functional impairment
neurology internal_medicine step2 -
RLS: common associated pathophysiology mentioned?
- Abnormal dopaminergic signaling
- Abnormal iron homeostasis
neurology internal_medicine step2 -
Role of serum ferritin in RLS diagnosis?
Decreased serum ferritin is associated with RLS exacerbation and helps confirm diagnosis
internal_medicine neurology step2 -
Iron supplementation in RLS: when recommended?
- Give iron supplementation for symptom improvement in patients with or without low ferritin
internal_medicine neurology step2 -
First-line treatments for RLS?
- Sleep-hygiene and lifestyle measures
- Iron supplementation
- Dopaminergic agonists (eg, ropinirole)
neurology internal_medicine step2 -
Why measurement of serum ferritin was the most appropriate next diagnostic step in this 47-year-old with bilateral leg restlessness?
Ferritin assesses iron stores; low ferritin associates with RLS and guides diagnosis/iron therapy
internal_medicine neurology step2 -
When is Doppler ultrasonography of lower extremities appropriate (vs RLS)?
Use Doppler to evaluate suspected DVT or PAD presenting with unilateral leg pain/swelling or exertional limb pain, not bilateral rest-related restlessness
surgery internal_medicine step2 -
When is EEG appropriate for nocturnal symptoms (vs RLS)?
EEG helps diagnose seizures or sleep arousals from epilepsy; not required when presentation fits RLS without seizure features
neurology psychiatry step2 -
When is fasting serum glucose useful for leg symptoms (vs RLS)?
Check fasting glucose to evaluate diabetes when suspected diabetic neuropathy causing sensory/motor deficits in a stocking‑glove distribution
internal_medicine endocrinology step2 -
Why 'no further testing' is incorrect for this patient?
Testing ferritin can confirm RLS and guide iron therapy; therefore at least ferritin measurement is indicated
internal_medicine neurology step2 -
Distinguishing feature: RLS vs peripheral arterial disease (PAD)?
RLS symptoms occur at rest and improve with movement; PAD causes activity‑provoked claudication relieved by rest
internal_medicine vascular_surgery step2 -
Distinguishing feature: RLS vs deep vein thrombosis (DVT)?
DVT usually causes unilateral leg pain and swelling; RLS causes bilateral rest-related unpleasant sensations without overt swelling
surgery internal_medicine step2 -
Distinguishing feature: RLS vs diabetic peripheral neuropathy?
Diabetic neuropathy causes sensory loss and weakness in stocking‑glove distribution; RLS has normal strength and light-touch sensation with rest‑provoked discomfort
internal_medicine neurology step2 -
Use of provided image as supplementary material for RLS education
 Image illustrates teaching points; do not use to identify diagnosisneurology internal_medicine step2
Image illustrates teaching points; do not use to identify diagnosisneurology internal_medicine step2 -
Scaphoid fracture: typical mechanism and common location
- Fall onto outstretched hand
- Scaphoid is most commonly fractured carpal bone
surgery step2. -
Scaphoid fracture: presenting exam findings
- Wrist pain with swelling
- Tenderness in anatomical snuffbox (between extensor pollicis longus and brevis)
internal_medicine step2. -
Scaphoid blood supply relevance to complications
Blood supply enters distally from a branch of the radial artery, placing proximal pole fractures at risk for nonunion and necrosis
surgery step2. -
orthopedics step2.
-
Initial imaging and next step if x-ray unremarkable but suspicion remains
- X-ray initial imaging
- If x-ray unremarkable and high suspicion: immobilize and repeat x-rays in 2–3 weeks
radiology step2. -
surgery step2.
-
Displaced scaphoid fracture: management consideration
Surgery may be indicated for displaced fractures
surgery step2. -
When is distal fat embolus expected after orthopedic trauma?
After pelvic or long-bone fractures due to bone marrow fat entering bloodstream; causes respiratory, neurologic, or petechial findings
critical step2. -
Osteomyelitis: diagnostic features distinguishing it from simple fracture
Infection with ↑ inflammatory markers (ESR, CRP) and radiographic lytic lesions or cortical destruction
infectious step2. -
Malunion of scaphoid fracture: expected consequence
Poor angulation causing pain or altered wrist biomechanics after healing
surgery step2. -
Wrist fusion in scaphoid disease: when considered
Considered after noninvasive measures fail for pain from nonunion or necrosis
orthopedics step2. -
Use of the provided image for scaphoid fracture learning
Image shows highlighted teaching slide; use as illustration for scaphoid fracture features and management
 education step2.
education step2. -
surgery step2.
-
Scaphoid blood supply and clinical consequence?
- Distal blood supply from a radial artery branch → risk of nonunion
surgery step2. -
surgery step2.
-
Scaphoid fracture: indications for surgical intervention?
- Displaced fractures
- Proximal pole fractures
surgery step2. -
Scaphoid fracture: why proximal pole fractures favor surgery?
- Proximal pole has poorer blood supply → higher nonunion risk → surgery recommended
surgery step2.
High-yield clinical notes (NBME-style cases)
Ethics & decision-making
- Assess decisional capacity first (case: 90-year-old refusing surgery). Capacity is decision-specific and requires the patient to: 1) express a consistent choice, 2) understand risks/benefits, 3) appreciate personal consequences, and 4) reason about options. If capacity intact, respect autonomy; if not, use durable power of attorney/ surrogate. Competence is a legal determination.
General diagnostic principles
- Single abnormal vital sign or lab rarely proves chronic disease (eg, one high BP does NOT equal hypertension). Confirm with repeat or home/serial measurements before workup for secondary causes.
- Use targeted tests: reserve complex imaging/ invasive tests for when they will change management (eg, CT angio for suspected PE when pretest probability high).
Trauma / Emergency
- Hemothorax after blunt chest trauma: immediate management = tube thoracostomy to drain blood, re-expand lung, and monitor ongoing bleeding (massive hemothorax if >1000–1500 mL initial or >200 mL/hr × 4 h).
- Intubation / airway: in anaphylaxis with stridor, give epinephrine immediately; if airway fails to improve or obstruction worsens, prepare for urgent intubation or surgical airway.
Pulmonary conditions
- Pulmonary embolism (PE): suspect with sudden dyspnea/hypoxemia and risk factors (immobility, obesity, recent surgery); spiral CT chest (CT pulmonary angiography) is preferred confirmatory test when clinical suspicion is high.
- Cardiogenic shock after MI: first-line inotropic support = dobutamine (B1 agonist) to increase contractility; vasopressors (eg, norepinephrine) may be used adjunctively if needed.
- Bacterial tracheitis (child with high fever, inspiratory stridor, no response to racemic epinephrine): think bacterial tracheitis — treat with antibiotics + steroids; airway surveillance (may need intubation).
Infectious diseases & prophylaxis
- Meningococcal exposure: give chemoprophylaxis to close contacts (rifampin, ciprofloxacin, or ceftriaxone), not all ED personnel.
- Postpartum endometritis: fever, foul lochia, uterine fundal tenderness after C-section → start broad-spectrum antibiotics promptly (eg, clindamycin + gentamicin) rather than routine imaging.
- Splenectomy preop vaccines: vaccinate against encapsulated organisms: Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis (give before splenectomy if possible).
Cardiac / vascular
- Right ventricular infarction (inferior MI with V4R–V6R changes): patients often are preload-dependent — give IV crystalloids (saline) as initial stabilization rather than diuretics or negative inotropes.
- Amaurosis fugax / Hollenhorst plaque: visible yellow refractile plaque in retinal arterioles suggests cholesterol embolus; evaluate with carotid duplex (ipsilateral carotid is common source).
- Atrial septal defect (fixed wide split S2) → chronic left-to-right shunt → risk of pulmonary vascular remodeling and later pulmonary hypertension/Eisenmenger if uncorrected.
Renal / GU
- Single functional kidney with hydronephrosis/obstruction: if imaging shows proximal obstruction and worsening renal function, percutaneous nephrostomy to decompress is appropriate as a temporizing measure.
- Gentamicin/aminoglycoside use in sepsis: monitor trough (and peak) levels to reduce nephrotoxicity risk; adjust dosing based on troughs.
- Septic shock with refractory hypotension: consider IV hydrocortisone for possible relative adrenal insufficiency when fluids + vasopressors inadequate and electrolytes suggest adrenal dysfunction.
Nephrology / transplant
- Tertiary hyperparathyroidism (long-standing CKD/transplant): persistent high PTH with hypercalcemia due to parathyroid hyperplasia and autonomous secretion; treat surgical parathyroidectomy if refractory.
- Membranous nephropathy (nephrotic): ACE inhibitors (eg, lisinopril) reduce intraglomerular pressure (efferent dilation) and slow progression by reducing hyperfiltration injury.
Hematology / transfusion
- Isoimmunization to RBC antigens (eg, Kell): strongest risk factor = prior blood transfusion (greater blood exposure increases alloimmunization risk) — important in pregnancy counseling and paternal antigen testing.
Gastroenterology / hepatology
- Acute viral hepatitis: very high AST/ALT (often >1000 U/L), +/- modest leukocytosis; supportive care while identifying specific viral cause.
- Pancreatic cancer suspicion: painless jaundice, weight loss, epigastric fullness, cholestatic labs → CT abdomen with contrast is the initial imaging of choice to evaluate for pancreatic mass.
GI/abdominal emergencies in adults
- Intussusception in adults: less common than in children, usually pathologic lead point; CT abdomen may show the "target sign" (telescoping bowel) — adult cases usually need surgical management.
Musculoskeletal / ortho
- Scaphoid fracture (fall on outstretched hand): common carpal fracture; frequent complication = nonunion due to retrograde/limited blood supply to proximal pole — immobilize and follow-up imaging; consider surgery if displaced.
- Spinal degenerative disease / chronic low back pain: in absence of red flags or focal neuro deficits, plain lumbar x-rays are an appropriate initial imaging test; reserve MRI for neurologic deficits or surgical planning.
Pediatrics
- Osteomyelitis (hematogenous, child): fever, refusal to bear weight, marrow edema on MRI; blood cultures and Gram stain guide therapy — vancomycin empirically for suspected MRSA in children until sensitivities return.
- Child with anaphylaxis while eating: immediate IM/IV epinephrine is first-line therapy.
- Bacterial tracheitis vs croup: unresponsive stridor and high fever after epinephrine suggests bacterial tracheitis — treat with antibiotics and airway monitoring.
Obstetrics / gynecology
- Rho(D) and other RBC antibodies: prior blood transfusion is a major risk for isoimmunization (eg, anti-Kell). Determine paternal antigen status to assess fetal risk; close monitoring or intervention if fetus at risk.
- Post-splenectomy: ensure vaccines against encapsulated organisms prior to surgery when possible.
Dermatology
- Cherry angiomas: common benign vascular papules appearing after age ~30; no workup needed and removal optional for cosmesis.
Alt: Cherry angiomas on skin, multiple small red papules.
Ophthalmology
- Hollenhorst plaque (cholesterol embolus) → transient monocular vision loss (amaurosis fugax); next step = carotid duplex to look for ipsilateral carotid atherosclerosis.
Alt: Fundus photo with bright refractile plaque in a retinal arteriole.
Dermatology / EENT quick points
- Bacterial vaginosis: gray malodorous discharge + clue cells on wet mount; treat with metronidazole.
- Cherry angiomas: benign, no testing required.
Endocrine / metabolic
- Bulimia with chronic laxative abuse: expect hypokalemia and non–anion-gap metabolic acidosis (loss of bicarbonate in stool); orthostatic hypotension from volume depletion is common.
- Restless legs syndrome (RLS): assess serum ferritin (iron deficiency worsens RLS); treat with iron repletion and dopamine agonists if symptomatic.
Oncology / pathology
- Lung cancer histology clues: central mass + hypercalcemia → squamous cell carcinoma (keratinization, intercellular bridges). Peripheral masses and nonsmokers → adenocarcinoma.
- Hodgkin lymphoma: Reed-Sternberg cells on node biopsy → next step = staging imaging (CT or PET) to assess distribution and plan therapy.
Pharmacology & toxicology
- Aminoglycosides (eg, gentamicin): nephrotoxicity risk — monitor trough levels and adjust dosing to prevent AKI.
- Hypertensive emergency due to sympathomimetics (eg, phentermine): use an α-blocker (eg, phentolamine) or direct vasodilator (eg, sodium nitroprusside); avoid β-blockers alone if α stimulation present.
Quality improvement & study design
- Medication errors from look-alike packaging: root-cause analysis often leads to systems fix (eg, repackage/relabel vials) rather than blaming staff.
- Intention-to-treat (ITT) analysis vs per-protocol: ITT preserves randomization and avoids bias; analyzing subjects by treatment actually received can produce misleading results.
- Statistical vs clinical significance: a small absolute difference can be statistically significant (P<0.05) but lack clinical relevance; consider absolute risk reduction and number needed to treat.
Imaging examples (selected)
- Chest x-ray (PE suspicion): may be nonspecific; if high suspicion, proceed to CT pulmonary angiography.
Alt: Chest x-ray used in PE case.
- CT abdomen with target sign: adult intussusception can show telescoped bowel with concentric rings/target appearance — usually surgical management.
Alt: CT abdomen with target sign consistent with intussusception.
Study tips: focus on pattern recognition (presenting features → likely diagnosis) and the single most important immediate management step for emergencies (eg, epinephrine for anaphylaxis; chest tube for hemothorax; CT angio for PE; dobutamine for cardiogenic shock).