Sauvegarde ton deck avant qu'il ne disparaisse
Ces flashcards ne sont pas encore sauvegardées — elles seront perdues si tu quittes. Crée un compte gratuit pour les garder et débloquer tout ce qui suit.
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
What is the primary bacterial target listed for nafcillin/dicloxacillin?
Which organisms are covered by amoxicillin/ampicillin in the chart?
Which beta-lactam/beta-lactamase inhibitor combinations are listed (chart) for broader coverage?
Which drugs are listed as anti-Enterococcal agents in the chart?
Which carbapenems are listed on the chart?
Which agent on the chart is noted as covering Pseudomonas?
Which cephalosporins are explicitly listed by generation on the chart?
Which agents are listed for MRSA/MSSA distinction on the chart?
Which oral outpatient options are listed on the chart for common infections?
Which antibiotics are listed for anaerobic coverage on the chart?
Which agents are listed under Enterics for Gram-negative coverage including aminoglycosides and fluoroquinolones?
What image supplements the antibiotic spectrum chart?
Flashcards in this deck (12)
-
What is the primary bacterial target listed for nafcillin/dicloxacillin?
- Staph
internal_medicine step2. -
Which organisms are covered by amoxicillin/ampicillin in the chart?
- Strep
- Enterics
internal_medicine step2. -
Which beta-lactam/beta-lactamase inhibitor combinations are listed (chart) for broader coverage?
- Amox/Clavulanate
- Amp/Sulbactam
- Piperacillin/tazobactam
internal_medicine step2. -
Which drugs are listed as anti-Enterococcal agents in the chart?
- Vancomycin
- Daptomycin
- Linezolid
internal_medicine step2. -
Which carbapenems are listed on the chart?
- Imipenem/meropenem/doripenem
- Ertapenem
internal_medicine step2. -
Which agent on the chart is noted as covering Pseudomonas?
- Piperacillin/tazobactam
internal_medicine step2. -
Which cephalosporins are explicitly listed by generation on the chart?
- 1st gen (cephalexin/cefazolin)
- 2nd gen (cefuroxime)
- 4th gen (cefepime)
internal_medicine step2. -
Which agents are listed for MRSA/MSSA distinction on the chart?
- MRSA appears in Strep/Staph header; MSSA listed near nafcillin/dicloxacillin
internal_medicine step2. -
Which oral outpatient options are listed on the chart for common infections?
- TMP/SMX
- Doxycycline
- Nitrofurantoin
internal_medicine step2. -
Which antibiotics are listed for anaerobic coverage on the chart?
- Metronidazole
- Clindamycin
- Moxifloxacin
internal_medicine step2. -
Which agents are listed under Enterics for Gram-negative coverage including aminoglycosides and fluoroquinolones?
- Aminoglycosides (eg gentamicin)
- Ciprofloxacin/Levofloxacin
internal_medicine step2. -
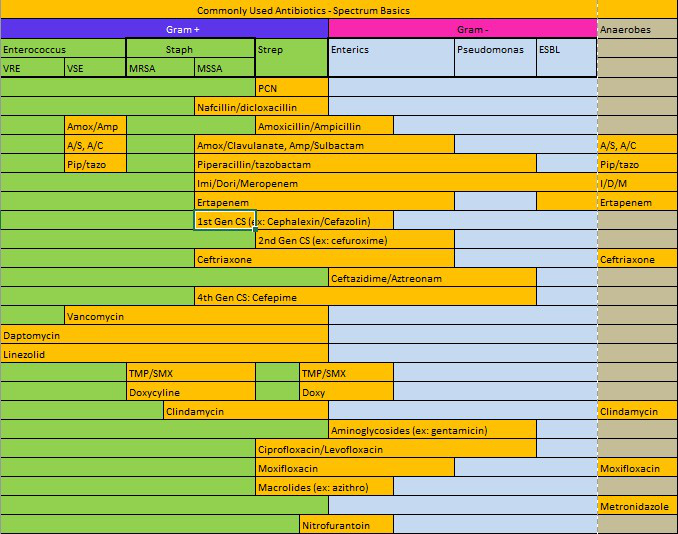
What image supplements the antibiotic spectrum chart?
- Spectrum chart image:
 (illustration only)
(illustration only)
internal_medicine step2. - Spectrum chart image:
High-level summary
Alt: Antibiotic spectrum basics chart by organism groups.
A compact reference of common antibiotics grouped by their usual activity against Gram-positive bacteria (Enterococcus, Staph, Strep), Gram-negative bacteria (enterics, Pseudomonas, ESBLs) and anaerobes, plus key agents for resistant organisms.
Quick-reference table (verbal)
- Narrow anti-staphylococcal penicillins (nafcillin, dicloxacillin): target MSSA and many strep species; not active vs MRSA.
- Aminopenicillins (amoxicillin, ampicillin): good for strep, some enterococci, and susceptible enterics; prone to beta-lactamase degradation.
- Beta-lactam/beta-lactamase inhibitors (amox/clav, amp/sulbactam): extend aminopenicillin coverage to many beta-lactamase producers and anaerobes.
- Anti-pseudomonal penicillins (piperacillin/tazobactam): broad gram-negative including Pseudomonas plus anaerobes.
- Carbapenems (imipenem, meropenem, doripenem): very broad (Gram+, Gram-, anaerobes) and active vs ESBL producers; ertapenem: similar but does NOT cover Pseudomonas.
- Cephalosporins: 1st gen (cefazolin/cephalexin) — MSSA, strep, some enterics; 2nd gen (cefuroxime) — improved gram-neg; 3rd gen (ceftriaxone) — broad community gram-neg and strep; ceftazidime — anti-Pseudomonas; 4th gen (cefepime) — broad gram-neg incl Pseudomonas.
- Monobactam (aztreonam): aerobic Gram-negative including Pseudomonas; useful in severe penicillin allergy.
- Glycopeptides & related: vancomycin — MRSA, most Gram+ (not VRE); daptomycin & linezolid — options for MRSA and VRE (daptomycin: not for pulmonary infections).
- TMP-SMX: good oral option for many enterics and community MRSA strains.
- Tetracyclines (doxycycline): covers atypicals, some MRSA and some Gram-negatives.
- Clindamycin: Gram+ and anaerobes (particularly above diaphragm), useful for toxin suppression in strep/staph.
- Aminoglycosides (gentamicin): potent Gram-negative activity and synergy for enterococcal endocarditis; notable nephro/ototoxicity.
- Fluoroquinolones: ciprofloxacin/levofloxacin — strong Gram-negative (cipro best for Pseudomonas); levo covers some Gram+/atypicals; moxifloxacin — better anaerobe/Gram+ but not Pseudomonas.
- Metronidazole: anaerobes (below diaphragm) and protozoa.
- Nitrofurantoin: oral agent for uncomplicated cystitis (E. coli); not for pyelonephritis.
- Macrolides (azithromycin): atypicals and some respiratory pathogens.
Important resistance-related points
- MRSA: treat with vancomycin, daptomycin (not for pneumonia), or linezolid.
- VRE: linezolid or daptomycin are first-line options.
- ESBL-producing Enterobacterales: often resistant to penicillins and cephalosporins; carbapenems (imipenem/meropenem/doripenem) are preferred.
- Pseudomonas: requires anti-pseudomonal agents (piperacillin-tazobactam, ceftazidime, cefepime, aztreonam, carbapenems except ertapenem, ciprofloxacin, aminoglycosides).
Drug-specific clinical pearls
- Ertapenem: broad-spectrum but no Pseudomonas coverage; useful for community ESBL or polymicrobial infections excluding Pseudomonas.
- Daptomycin: inactivated by lung surfactant — avoid for pneumonia.
- Aztreonam: safe in severe penicillin allergy; covers Gram-negatives only.
- Nitrofurantoin: oral, concentrates in urine — for cystitis only, not systemic infections.
- Metronidazole: excellent for anaerobes and C. difficile (treatment choice historically), but oral vancomycin or fidaxomicin now preferred for severe C. difficile.
- Aminoglycosides: monitor levels; nephro- and ototoxicity risks.
How to choose empiric therapy (practical steps)
- Identify likely pathogens by site of infection and host factors (community vs healthcare-associated, recent antibiotics).
- Assess need for Pseudomonas / ESBL / MRSA coverage.
- Check allergies — if severe beta-lactam allergy, consider aztreonam (Gram-neg), vancomycin/linezolid (Gram+).
- Start broad empiric therapy for severe infections; narrow (de-escalate) once culture/susceptibilities return.
- Consider drug properties: oral bioavailability, tissue penetration (e.g., lung, CSF), renal/hepatic dosing, toxicity.
Common clinical examples (concise)
- Uncomplicated cystitis: nitrofurantoin or TMP-SMX (based on local resistance).
- Skin & soft tissue (non-purulent): beta-lactam active vs streptococci (e.g., cefazolin); purulent MRSA — TMP-SMX or doxycycline.
- Community-acquired pneumonia: ceftriaxone + macrolide or respiratory fluoroquinolone (site/severity dependent).
- Intra-abdominal/aspiration: agents with anaerobic coverage (piperacillin-tazobactam, ertapenem, or ceftriaxone + metronidazole).
- Sepsis/critically ill: broad Gram-negative + Gram-positive coverage including anti-pseudomonal and anti-MRSA agents until cultures guide therapy.
Rapid checklist for exams/wards
- If suspect MRSA → add vancomycin/linezolid/daptomycin.
- If suspect Pseudomonas → choose anti-pseudomonal beta-lactam (cefepime, ceftazidime, piperacillin-tazobactam) ± aminoglycoside or ciprofloxacin.
- If suspect ESBL → use carbapenem (imipenem/meropenem/doripenem); ertapenem if Pseudomonas unlikely.
- For anaerobes below the diaphragm → metronidazole or beta-lactam/beta-lactamase inhibitor or carbapenem.
Final reminders
- Always tailor antibiotics to culture results and local antibiogram data.
- Weigh efficacy vs toxicity, site penetration, and route (IV vs oral) when switching therapy.
- De-escalate promptly to limit resistance and adverse effects.