Sauvegarde ton deck avant qu'il ne disparaisse
Ces flashcards ne sont pas encore sauvegardées — elles seront perdues si tu quittes. Crée un compte gratuit pour les garder et débloquer tout ce qui suit.
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
What is the clinical definition of gingival recession?
What primary condition is gingival recession associated with?
How does the prevalence of gingival recession correlate with age?
It is unrelated to age
It decreases with age
It increases with age
It remains constant
Which tooth surfaces are most commonly affected by gingival recession?
What secondary dental conditions may occur if a patient struggles to keep recession areas clean?
Beyond dental hygiene concerns, what is a major fear patients may have regarding gingival recession?
What factors contribute to the aetiology of gingival attachment loss?
What components define the periodontal phenotype?
What are the clinical characteristics of a thick periodontal phenotype?
How can a thick periodontal phenotype be identified using a periodontal probe?
What are the clinical signs of a thin periodontal phenotype?
List five clinical conditions associated with gingival recession.
When measuring gingival thickness by probing horizontally in an anaesthetised patient, what is the clinical recommendation regarding frequency?
It is the standard primary method for monitoring tissue health.
It should not be done on a regular basis.
It is only required for patients with thick phenotypes.
It should be performed at every recall visit.
What is considered the primary predisposing factor for gingival recession?
In a healthy periodontium, what is the typical vertical position of the buccal alveolar bone crest relative to the gingival margin?
What term describes bone loss that is limited to a single tooth, where the proximal bone height remains unaffected?
What is the clinical term for a localized discontinuity in the bone?
How do gingival tissues generally react to reduced cervical bone levels?
Where does gingival recession typically come to a natural halt?
What clinical signs suggest that a patient has a thin periodontal phenotype?
In patients with a thin periodontal phenotype, what is a potential long-term risk of orthodontic movements in the bucco-lingual direction?
How does the prevalence of post-orthodontic gingival recession change between the end of treatment and a 5-year observation period?
What anatomical factor is frequently associated with gingival recession specifically in the lower central incisors?
Which diagnostic imaging method is used to verify buccal tooth positioning and the presence of a dehiscence?
What is the primary reason why bucco-lingual tooth movement can lead to gingival recession in patients with a thin periodontal phenotype?
It causes premature tooth eruption.
It increases inflammation in the gingival sulcus.
It damages the enamel surface of the root.
It causes the loss or reduction of the buccal bone plate.
What structure is responsible for the destruction of attachment components in the context of periodontal disease?
Which of the following is true regarding the role of biofilm in periodontal attachment loss?
Biofilm is solely responsible for tissue destruction without involving the body's immune system.
Biofilm itself does not directly cause attachment loss.
Biofilm produces enough enzymes to completely destroy tissue components.
Biofilm is the primary direct cause of all attachment loss.
What is characterized by a minimal amount of keratinised gingiva apically of an exposed root surface?
Where do the frenum ligaments attach?
Why is it difficult for patients to keep exposed root surfaces clean in cases of gingival recession?
What clinical condition is associated with chronic trauma to the gingiva?
Increased keratinisation
Gingival fibrosis
Recession development
Hypertrophic gingivitis
What is a common consequence of an oral piercing that constantly contacts the gingival margins?
Besides piercings, what is another documented cause of physical trauma to the gums?
What specific toothbrushing practices can lead to long-lasting, low-level trauma resulting in gingival recession?
What is a potential adverse effect of incorrectly using interdental cleaning products?
In what type of patient do toothbrush-related recessions most commonly occur?
Patients who never perform interdental cleaning.
Patients with poor oral hygiene habits.
Patients with periodontal disease.
Patients with a high standard of oral hygiene and biofilm control.
What happens if you perform debridement on periodontal pockets with a depth of more than 3mm?
What is the potential result of performing debridement on pockets less than 2.9mm deep?
When should you avoid debridement of periodontal pockets?
When the patient reports constant pain in the area.
When pockets are 3mm or less with no bleeding, no inflammation, and no calculus or biofilm.
When pockets are deeper than 5mm.
When there is evidence of heavy calculus.
What are the common clinical consequences of over-treating periodontal pockets via unnecessary debridement?
What factors can mask the actual attachment loss in patients with periodontitis?
Why does gingival tissue retract after the removal of biofilm and calculus in periodontitis treatment?
What should patients be advised regarding potential post-treatment root surface exposure?
What anatomical components comprise the supracrestal attached tissues?
What is the average dimension of the biologic width, including its components?
What clinical consequence is expected when a crown margin is placed within the \(2\text{ mm}\) supracrestal attached tissue zone?
What is a potential risk associated with placing restorative margins within the gingival sulcus?
Mandibular stabilization
Decreased cementum thickness
Increased bone density
Gingival recession
What happens to the supracrestal attachment during restorative procedures where margins are placed improperly?
What is the primary clinical consequence of leaving gingival inflammation untreated?
What is the treatment goal for cases where inflammation causes loss of periodontal attachment?
What is the purpose of surgical crown lengthening in the context of supracrestal attachment?
Why does the risk of gingival recession increase with age?
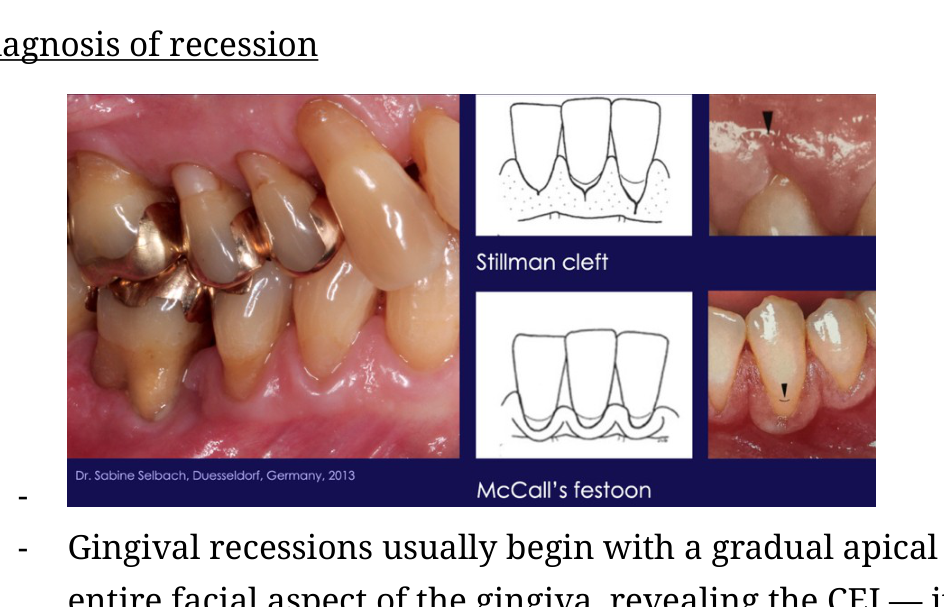
Describe the clinical process of gingival recession.
Identify two distinct clinical features associated with gingival recession that can be observed clinically.
What does a Stillman cleft in the gingiva often indicate?
What is McCall's festoon?
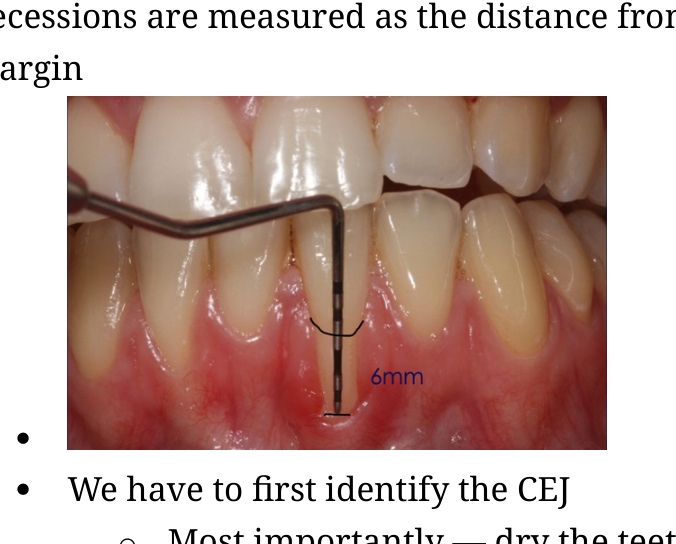
How is gingival recession measured?
What is the primary method to start identifying the CEJ on a tooth surface?
Apply fluoride varnish
Anesthetize the gingiva
Use a disclosing solution
Dry the teeth
How does the tactile sensation differ between enamel and cementum when using a probe?
If a tooth has cervical lesions or fillings, what techniques can help identify the CEJ?
When measuring recessions for teeth with crowns, what assumption is typically made regarding the preparation margin?
Can facial gingival recessions be identified using radiographs?
How is Type 1 gingival recession defined in terms of attachment loss?
What is the key diagnostic criteria for Type 2 gingival recession?
How does Type 3 gingival recession differ from Type 2 regarding attachment loss?
How is interproximal attachment loss measured for Type 2 recession?
How is recession depth defined in the context of gingival measurements?
What is the primary landmark used to measure attachment loss?
Describe the clinical characteristic of RT1 gingival recession.
What defines RT2 gingival recession regarding interproximal attachment loss?
What defines RT3 gingival recession regarding interproximal attachment loss?
In the classification of mucogingival conditions, what do the symbols 'Class A' and 'Class B' denote regarding the CEJ?
How is the presence of a cervical step defined in the classification of mucogingival conditions?
What methods are used for the thorough assessment and documentation of gingival recession?
Why is thorough documentation of gingival recession important during treatment?
What is the primary action taken after assessment in the treatment of gingival recession?
What is the typical rate of gingival recession development?
It typically occurs slowly
It only occurs overnight
It is always congenital
It typically occurs quickly
What are two consequences of root surface exposure that require clinical attention?
How is dental hypersensitivity managed in patients with root surface exposure?
When is it appropriate to monitor recession defects?
What clinical signs or factors indicate a need for intervention in patients with gingival recession?
How can U-shaped local gingival recession be corrected via orthodontic treatment?
What type of surgical procedure is used for treating gingival recession using a graft?
What specific patient conditions might necessitate a connective tissue autograft procedure?
What tissues are harvested for a free gingival autograft?
What is the primary purpose of a free gingival autograft in cases of mild recession?
What characteristic distinguishes a pedicle flap from grafts transferred from the palate?
In what clinical condition is a coronally repositioned flap indicated?
What is the two-step surgical process for treating extensive recession beyond the mucogingival junction?
What clinical visual signs are indicative of a thin periodontal phenotype?
Which teeth exhibit gingival recession in the provided clinical example?
What anatomical characteristics are associated with a thin periodontal phenotype and a buccally positioned tooth?
What does a white square lesion on a tooth after orthodontic treatment typically indicate?
What is the likely cause of grooves observed on the enamel of a tooth following the removal of orthodontic brackets?
What clinical sign suggests that a patient has previously undergone a frenectomy?
What dental condition is associated with a high frenum attachment between the two incisors?
What clinical signs suggest that a patient may have an aggressive brushing technique?
What clinical feature on the canine suggests a potential issue with bruxism?
Describe the state of the buccal bone plate for tooth 14.
What bone defects are identified on the mesial and distobuccal roots of tooth 16?
Describe the radiographic appearance of the root of tooth 17.
What clinical observations indicate good oral hygiene?
Flashcards in this deck (102)
-
What is the clinical definition of gingival recession?
An apical shift of the gingival margin, causing it to displace away from the CEJ.
dentistry recession -
What primary condition is gingival recession associated with?
Clinical attachment loss.
dentistry recession -
How does the prevalence of gingival recession correlate with age?
It is unrelated to age
It decreases with age
It increases with age
It remains constant
dentistry epidemiology -
Which tooth surfaces are most commonly affected by gingival recession?
Buccal smooth surfaces.
dentistry recession -
What secondary dental conditions may occur if a patient struggles to keep recession areas clean?
- Root caries
- Non-carious cervical lesions
dentistry complications -
Beyond dental hygiene concerns, what is a major fear patients may have regarding gingival recession?
They may be anxious and fearful of losing their teeth.
dentistry patient-care -
What factors contribute to the aetiology of gingival attachment loss?
An interplay of morphology, anatomy, and an inflammatory component.
periodontology aetiology -
What components define the periodontal phenotype?
- Gingival thickness
- Width of keratinised gingiva
- Bone morphology
- Thickness of buccal bone plate
periodontology phenotype -
What are the clinical characteristics of a thick periodontal phenotype?
- Presence of a good buccal bone plate
- Gingival tissue thickness greater than \(1mm\)
- Presence of a wide band of keratinised gingiva
periodontology phenotype -
How can a thick periodontal phenotype be identified using a periodontal probe?
By inserting the probe into the sulcus; the probe will not be visible shimmering through the gingival tissues.
periodontology diagnostics -
What are the clinical signs of a thin periodontal phenotype?
- Fairly thin buccal bone plate
- Gingiva appears semi-transparent (see-through)
- The periodontal probe is visible shimmering through the gingiva when inserted into the sulcus
periodontology phenotype -
List five clinical conditions associated with gingival recession.
- Dentine Hypersensitivity
- Non-carious cervical lesions (NCCL)
- Esthetic concerns
- Impaired oral hygiene (OH)
- Caries
periodontology clinical -
When measuring gingival thickness by probing horizontally in an anaesthetised patient, what is the clinical recommendation regarding frequency?
It is the standard primary method for monitoring tissue health.
It should not be done on a regular basis.
It is only required for patients with thick phenotypes.
It should be performed at every recall visit.
periodontology diagnostics -
What is considered the primary predisposing factor for gingival recession?
The lack of keratinized tissues.
periodontology gingiva -
In a healthy periodontium, what is the typical vertical position of the buccal alveolar bone crest relative to the gingival margin?
It lies approximately 2mm apically to the gingival margin.
periodontology anatomy -
What term describes bone loss that is limited to a single tooth, where the proximal bone height remains unaffected?
Dehiscence.
periodontology pathology -
What is the clinical term for a localized discontinuity in the bone?
Fenestration.
periodontology pathology -
How do gingival tissues generally react to reduced cervical bone levels?
The gingiva follows and reduces with the bone, resulting in recession.
periodontology gingiva -
Where does gingival recession typically come to a natural halt?
At the apex area where the buccal bone plate becomes thicker.
periodontology gingiva -
What clinical signs suggest that a patient has a thin periodontal phenotype?
The periodontal phenotype is considered thin when blood vessels and the underlying bone plate are visible through the gingiva.
dentistry periodontology -
In patients with a thin periodontal phenotype, what is a potential long-term risk of orthodontic movements in the bucco-lingual direction?
These movements may occur at the expense of the buccal bone plate, which can lead to the development of gingival recession after treatment.
dentistry orthodontics periodontology -
How does the prevalence of post-orthodontic gingival recession change between the end of treatment and a 5-year observation period?
The prevalence increases from 5-12% at the end of treatment up to 47% after 5 years.
dentistry orthodontics -
What anatomical factor is frequently associated with gingival recession specifically in the lower central incisors?
A high frenum attachment.
dentistry periodontology -
Which diagnostic imaging method is used to verify buccal tooth positioning and the presence of a dehiscence?
A CR scan.
dentistry diagnostics -
What is the primary reason why bucco-lingual tooth movement can lead to gingival recession in patients with a thin periodontal phenotype?
It causes premature tooth eruption.
It increases inflammation in the gingival sulcus.
It damages the enamel surface of the root.
It causes the loss or reduction of the buccal bone plate.
dentistry orthodontics -
What structure is responsible for the destruction of attachment components in the context of periodontal disease?
The body's own inflammatory reaction.
periodontology inflammation -
Which of the following is true regarding the role of biofilm in periodontal attachment loss?
Biofilm is solely responsible for tissue destruction without involving the body's immune system.
Biofilm itself does not directly cause attachment loss.
Biofilm produces enough enzymes to completely destroy tissue components.
Biofilm is the primary direct cause of all attachment loss.
periodontology biofilm -
What is characterized by a minimal amount of keratinised gingiva apically of an exposed root surface?
A thinner periodontal phenotype.
periodontology phenotype -
Where do the frenum ligaments attach?
Into the supracrestal connective tissue.
anatomy periodontology -
Why is it difficult for patients to keep exposed root surfaces clean in cases of gingival recession?
Recession leads to increased biofilm accumulation and potentially a secondary infection of gingivitis.
periodontology recession -
What clinical condition is associated with chronic trauma to the gingiva?
Increased keratinisation
Gingival fibrosis
Recession development
Hypertrophic gingivitis
periodontology trauma -
What is a common consequence of an oral piercing that constantly contacts the gingival margins?
Constant scrubbing against the delicate gingival margins, which can lead to gum recession.
dentistry trauma gingiva -
Besides piercings, what is another documented cause of physical trauma to the gums?
Direct physical trauma, such as a cut to the gums.
dentistry trauma gingiva -
What specific toothbrushing practices can lead to long-lasting, low-level trauma resulting in gingival recession?
Using a hard toothbrush or employing an inadequate horizontal scrubbing technique.
dentistry hygiene recession -
What is a potential adverse effect of incorrectly using interdental cleaning products?
Physical wounding of the delicate gingival margins, which can cause gradual gingival recession.
dentistry hygiene recession -
In what type of patient do toothbrush-related recessions most commonly occur?
Patients who never perform interdental cleaning.
Patients with poor oral hygiene habits.
Patients with periodontal disease.
Patients with a high standard of oral hygiene and biofilm control.
dentistry hygiene recession -
What happens if you perform debridement on periodontal pockets with a depth of more than 3mm?
It will result in an attachment gain.
periodontics debridement -
What is the potential result of performing debridement on pockets less than 2.9mm deep?
It can result in attachment loss.
periodontics debridement -
When should you avoid debridement of periodontal pockets?
When the patient reports constant pain in the area.
When pockets are 3mm or less with no bleeding, no inflammation, and no calculus or biofilm.
When pockets are deeper than 5mm.
When there is evidence of heavy calculus.
periodontics debridement -
What are the common clinical consequences of over-treating periodontal pockets via unnecessary debridement?
Recessions and exposed root surfaces.
periodontics debridement -
What factors can mask the actual attachment loss in patients with periodontitis?
- Gingival oedema
- Inflammatory infiltrate
- Exudate
periodontitis pathology -
Why does gingival tissue retract after the removal of biofilm and calculus in periodontitis treatment?
The gingiva follows the reduction of bone crest height and contour as inflammation resolves.
periodontitis healing -
What should patients be advised regarding potential post-treatment root surface exposure?
It is a result of eliminating inflammation, not a direct result of the surgical instrument removal of tissue.
periodontics patient-education -
What anatomical components comprise the supracrestal attached tissues?
- Junctional epithelium
- Supracrestal connective tissue attachment
periodontics anatomy -
What is the average dimension of the biologic width, including its components?
The biologic width is approximately \(2.04\text{ mm}\) wide, consisting of: - \(0.97\text{ mm}\) junctional epithelium - \(1.07\text{ mm}\) connective tissue attachment
periodontics anatomy -
What clinical consequence is expected when a crown margin is placed within the \(2\text{ mm}\) supracrestal attached tissue zone?
Gingival inflammation will occur.
periodontics restorative -
What is a potential risk associated with placing restorative margins within the gingival sulcus?
Mandibular stabilization
Decreased cementum thickness
Increased bone density
Gingival recession
restorative periodontics -
What happens to the supracrestal attachment during restorative procedures where margins are placed improperly?
The restoration violates the supracrestal attachment.
restorative periodontics -
What is the primary clinical consequence of leaving gingival inflammation untreated?
The loss of periodontal attachment.
periodontology inflammation -
What is the treatment goal for cases where inflammation causes loss of periodontal attachment?
To recreate the supracrestal attachment tissues, typically aiming for 2mm.
treatment periodontology -
What is the purpose of surgical crown lengthening in the context of supracrestal attachment?
To intentionally remove some bone to recreate the space needed for the supracrestal attachment to reform.
surgery crown-lengthening -
Why does the risk of gingival recession increase with age?
It is because aetiological factors have acted on the patient for a longer duration, rather than the aging process directly causing the recession.
recession aetiology -
Describe the clinical process of gingival recession.
It is a slow, chronic process defined by the gradual apical migration of the entire facial aspect of the gingiva, which reveals the cemento-enamel junction (CEJ).
recession gingiva -
Identify two distinct clinical features associated with gingival recession that can be observed clinically.
- Stillman cleft
- McCall's festoon
 pathology clinical
pathology clinical -
What does a Stillman cleft in the gingiva often indicate?
It is often seen as an early sign of a very rapidly progressing gingival recession.
periodontology recession -
What is McCall's festoon?
A non-inflammatory fibrotic response of the gingiva, characterized by a thickened and rolled gingival margin in cases of pronounced recession.
periodontology gingiva -
How is gingival recession measured?
It is measured as the distance from the cementoenamel junction (CEJ) to the gingival margin.
 periodontology measurement
periodontology measurement -
What is the primary method to start identifying the CEJ on a tooth surface?
Apply fluoride varnish
Anesthetize the gingiva
Use a disclosing solution
Dry the teeth
periodontology cej -
How does the tactile sensation differ between enamel and cementum when using a probe?
Enamel feels smooth, whereas cementum feels rough.
periodontology diagnosis -
If a tooth has cervical lesions or fillings, what techniques can help identify the CEJ?
- Follow the adjacent CEJ in a scalloped pattern
- Compare with the CEJ of the contralateral tooth
periodontology clinical -
When measuring recessions for teeth with crowns, what assumption is typically made regarding the preparation margin?
It is assumed that the preparation margin was placed at the height of the CEJ (cementoenamel junction).
dentistry periodontics recession -
Can facial gingival recessions be identified using radiographs?
No, we are unable to identify any facial gingival recessions on radiographs.
dentistry radiography diagnostics -
How is Type 1 gingival recession defined in terms of attachment loss?
Type 1 recession is characterized by gingival recession with no loss of interproximal attachments, where the interproximal CEJ is clinically undetectable.
dentistry classification periodontics -
What is the key diagnostic criteria for Type 2 gingival recession?
Type 2 recession is associated with the loss of interproximal attachment, where the interproximal attachment loss is less than or equal to the buccal attachment loss.
dentistry classification periodontics -
How does Type 3 gingival recession differ from Type 2 regarding attachment loss?
In Type 3 recession, the interproximal attachment loss is higher than the buccal attachment loss.
dentistry classification periodontics -
How is interproximal attachment loss measured for Type 2 recession?
It is measured from the interproximal CEJ to the depth of the interproximal sulcus.
dentistry periodontics measurements -
How is recession depth defined in the context of gingival measurements?
Recession is measured from the cemento-enamel junction (CEJ) to the gingival margin.
dentistry periodontology -
What is the primary landmark used to measure attachment loss?
Attachment loss is measured from the cemento-enamel junction (CEJ) to the depth of the pocket.
dentistry periodontology -
Describe the clinical characteristic of RT1 gingival recession.
Gingival recession with no loss of interproximal attachment.
dentistry classification -
What defines RT2 gingival recession regarding interproximal attachment loss?
Gingival recession associated with interproximal attachment loss, where the loss measured from the interproximal CEJ to the depth of the pocket is less than or equal to the buccal attachment loss measured from the buccal CEJ to the apical end of the buccal sulcus/pocket.
dentistry classification -
What defines RT3 gingival recession regarding interproximal attachment loss?
Gingival recession associated with interproximal attachment loss, where the loss measured from the interproximal CEJ to the depth of the pocket is greater than the buccal attachment loss measured from the buccal CEJ to the apical end of the buccal sulcus/pocket.
dentistry classification -
In the classification of mucogingival conditions, what do the symbols 'Class A' and 'Class B' denote regarding the CEJ?
- Class A: Detectable cemento-enamel junction (CEJ)
- Class B: Un-detectable cemento-enamel junction (CEJ)
dentistry definitions -
How is the presence of a cervical step defined in the classification of mucogingival conditions?
A cervical step is defined as root surface concavity greater than \(0.5\text{ mm}\).
dentistry definitions -
What methods are used for the thorough assessment and documentation of gingival recession?
- Perio charting
- Intra-oral photography
- Study models
- Intra-oral scanning
dentistry recession -
Why is thorough documentation of gingival recession important during treatment?
To track the progression rate of the recession.
dentistry recession -
What is the primary action taken after assessment in the treatment of gingival recession?
To identify and modify aetiological factors contributing to the condition.
dentistry recession -
What is the typical rate of gingival recession development?
It typically occurs slowly
It only occurs overnight
It is always congenital
It typically occurs quickly
dentistry recession -
What are two consequences of root surface exposure that require clinical attention?
- Dental hypersensitivity
- Root surface caries or non-carious cervical lesions
dentistry recession -
How is dental hypersensitivity managed in patients with root surface exposure?
By implementing desensitisation treatments.
dentistry recession -
When is it appropriate to monitor recession defects?
When the aetiological factor is successfully modified and the consequences of root surface exposure are managed.
dentistry recession -
What clinical signs or factors indicate a need for intervention in patients with gingival recession?
- Increasing recession
- Persistent inflammation
- Uncontrollable dentine hypersensitivity
- Aesthetic concerns
- Presence of early carious lesions
- Young patients with deep recessions
periodontics dentistry -
How can U-shaped local gingival recession be corrected via orthodontic treatment?
By orthodontically repositioning the incisor, which allows the buccal bone plate to thicken and the exposed root surface to be covered with gingiva again.
orthodontics periodontics -
What type of surgical procedure is used for treating gingival recession using a graft?
Mucogingival surgery using a free soft tissue graft, such as a connective tissue autograft.
surgery periodontics -
What specific patient conditions might necessitate a connective tissue autograft procedure?
- Aesthetic compromise
- Early caries on the root surface
surgery periodontics -
What tissues are harvested for a free gingival autograft?
- Keratinised epithelium
- Some underlying connective tissue
surgery graft dentistry -
What is the primary purpose of a free gingival autograft in cases of mild recession?
To thicken the keratinised gingiva.
surgery graft dentistry -
What characteristic distinguishes a pedicle flap from grafts transferred from the palate?
A pedicle flap remains attached through its base, which allows it to maintain its blood supply.
surgery pedicle-flap dentistry -
In what clinical condition is a coronally repositioned flap indicated?
It is used when there is extensive recession beyond the mucogingival junction.
surgery coronally-repositioned-flap dentistry -
What is the two-step surgical process for treating extensive recession beyond the mucogingival junction?
- First: A free gingival autograft is performed to widen the keratinised gingiva.
- Second: A gingival flap is pulled coronally to the CEJ.
surgery coronally-repositioned-flap dentistry -
What clinical visual signs are indicative of a thin periodontal phenotype?
The ability to see blood vessels shining through the gingival tissue and areas where the underlying bone is visible through the tissue.
periodontics phenotype -
Which teeth exhibit gingival recession in the provided clinical example?
Tooth 32, the upper canine, and the premolars.
recession clinical -
What anatomical characteristics are associated with a thin periodontal phenotype and a buccally positioned tooth?
A thin buccal plate and a reduced buccal dimension of both the gingiva and the underlying bone.
anatomy periodontics -
What does a white square lesion on a tooth after orthodontic treatment typically indicate?
It is a sign of demineralisation, often resulting from suboptimal oral hygiene during the time the patient wore orthodontic brackets.
orthodontics pathology -
What is the likely cause of grooves observed on the enamel of a tooth following the removal of orthodontic brackets?
The grooves likely occurred during the enamel polishing process when the brackets were being removed.
orthodontics enamel -
What clinical sign suggests that a patient has previously undergone a frenectomy?
The presence of scarring at the frenum attachment site.
frenectomy oral_surgery -
What dental condition is associated with a high frenum attachment between the two incisors?
The presence of a gap between the teeth.
frenum dentistry -
What clinical signs suggest that a patient may have an aggressive brushing technique?
Recessions occurring primarily on the upper canines and premolars.
dentistry diagnosis -
What clinical feature on the canine suggests a potential issue with bruxism?
The presence of wear facets.
dentistry bruxism -
Describe the state of the buccal bone plate for tooth 14.
There is nearly no buccal bone plate existing all the way to the apex.
dentistry bone -
What bone defects are identified on the mesial and distobuccal roots of tooth 16?
A large dehiscence on the mesial buccal root and a fenestration on the distobuccal root.
dentistry bone -
Describe the radiographic appearance of the root of tooth 17.
The root appears fairly thin.
dentistry radiology -
What clinical observations indicate good oral hygiene?
Limited presence of interproximal biofilm and minimal calculus.
dentistry hygiene