デッキが消える前に保存しよう
このフラッシュカードはまだ保存されてないよ — 離れると消えちゃう。無料アカウントを作ると保存できて、下の機能も全部使えるようになるよ。
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
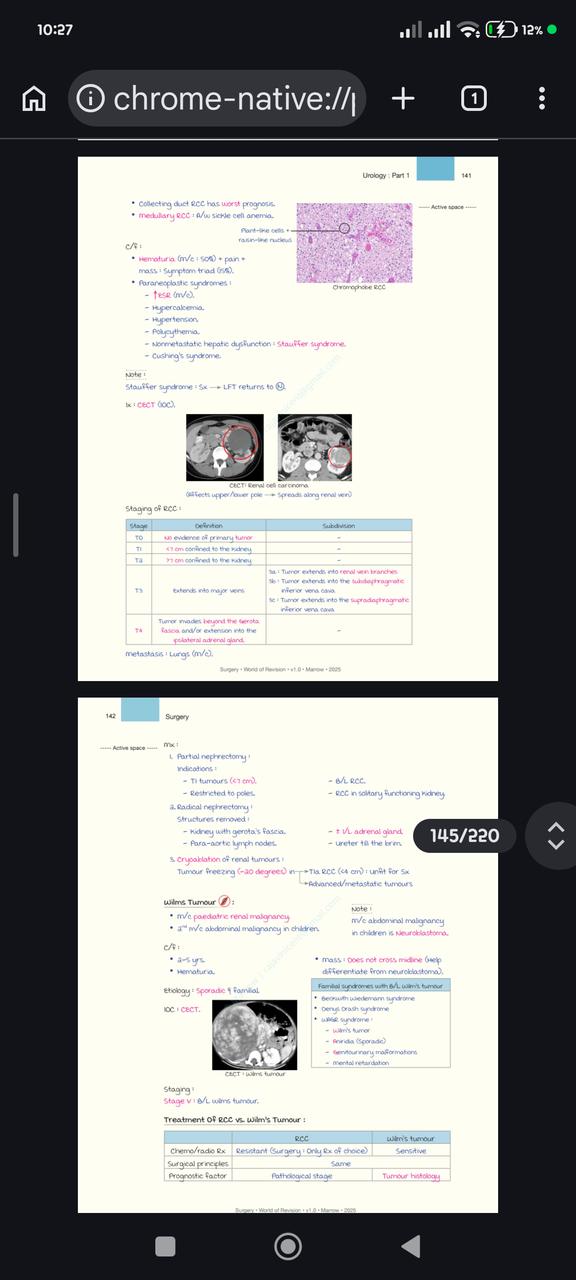
Which subtype of renal cell carcinoma has the worst prognosis?
Which renal cell carcinoma subtype is associated with sickle cell anemia?
What is the most common presenting symptom of renal cell carcinoma and its approximate frequency?
What classic symptom triad can occur in renal cell carcinoma and how often does it appear?
Name two common paraneoplastic findings in renal cell carcinoma.
What is Stauffer syndrome in the context of renal cell carcinoma?
What investigation is listed as the investigation of choice (IOC) for renal cell carcinoma?
Which organ is the most common site of metastasis for renal cell carcinoma?
How is T1 stage of renal cell carcinoma defined in the provided staging?
How is T2 stage of renal cell carcinoma described in the provided staging?
What structures are removed in a radical nephrectomy according to the notes?
What are the indications for partial nephrectomy listed in the notes?
What is the most common paediatric renal malignancy and common abdominal malignancy in children?
Typical age and a presenting sign for Wilms tumour?
How does Wilms tumour help differentiate from neuroblastoma by abdominal mass behavior?
Name three familial syndromes associated with bilateral Wilms tumour.
Use the provided image as an illustration: which investigation image is shown for renal cell carcinoma?
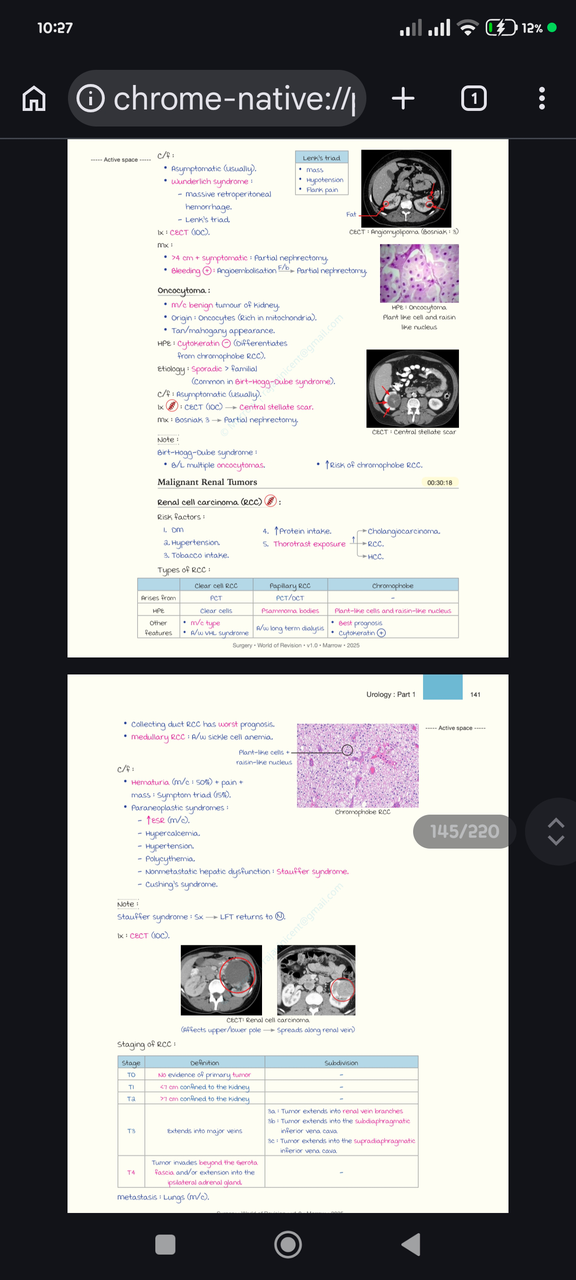
What is the usual clinical presentation of angiomyolipoma (AML)?
What is Lenk's triad in Wunderlich syndrome related to AML?
Which imaging study is listed for evaluation of renal masses like AML and RCC?
What is the management for symptomatic angiomyolipoma larger than 4 cm?
What is the immediate management for a bleeding angiomyolipoma?
What are the key histologic features described as 'plant-like' in the notes?
Give two gross or histologic features of oncocytoma listed in the notes.
Which immunohistochemical marker is noted to help differentiate oncocytoma from chromophobe RCC?
What syndrome is associated with multiple bilateral oncocytomas?
List three risk factors for renal cell carcinoma (RCC) mentioned in the notes.
Which RCC subtype is described as the most common and associated with VHL syndrome?
Which RCC subtype is noted to contain psammoma bodies and be associated with long-term dialysis?
Which RCC subtype is reported to have the best prognosis in the notes?
What is the most common presenting symptom of RCC and its approximate frequency?
Name three paraneoplastic syndromes associated with RCC from the notes.
What nonmetastatic hepatic phenomenon is named in association with RCC?
According to the notes, where does RCC most commonly metastasize?
What defines T1 stage of RCC in the provided staging lines?
What is the defining feature of T3 stage in RCC staging provided?
Which collecting-duct-related RCC variant is noted to have the worst prognosis?
Which medullary RCC association is mentioned in the notes?
Which image file from the provided media shows a CT scan feature of oncocytoma?
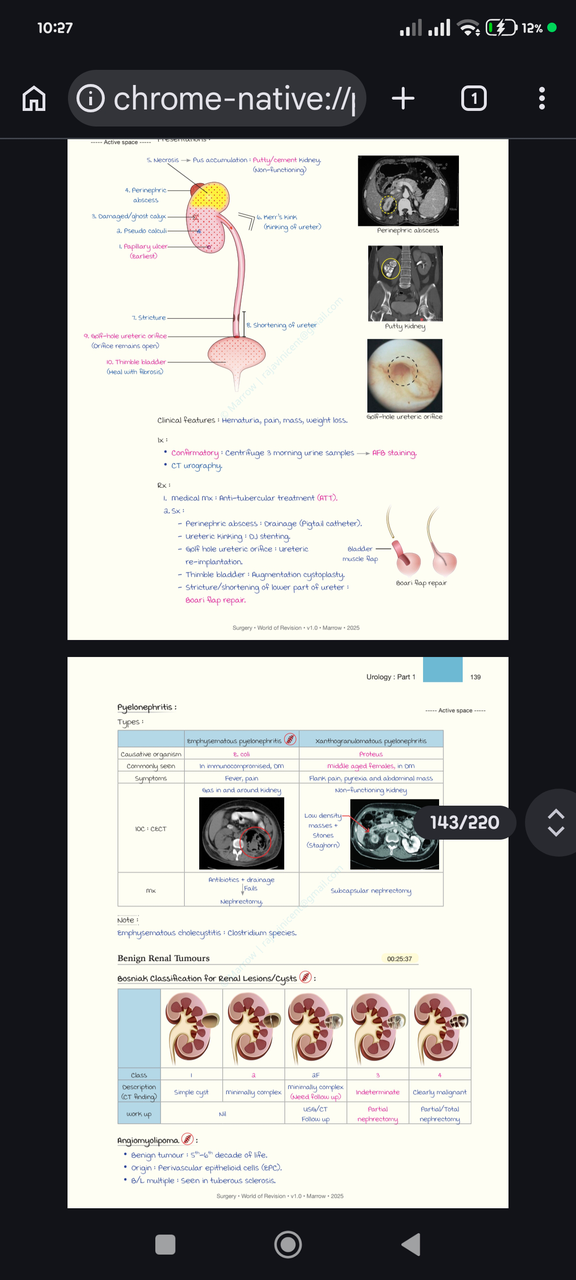
List three early complications of renal tuberculosis shown in the sequence of lesions.
What radiological appearance is described by the term 'Putty kidney' in renal tuberculosis?
Name three clinical features associated with a putty/cement kidney.
Which investigations are listed for confirming a 'golf-hole' ureteric orifice in renal tuberculosis?
What is the first-line medical management for renal tuberculosis?
Give one surgical treatment listed for perinephric abscess complicating renal TB.
What operative procedure is recommended for a golf-hole ureteric orifice?
What reconstructive procedure is listed for a thimble bladder healed with fibrosis?
Which repair is indicated for stricture/shortening of the lower ureter?
Which organism is most commonly associated with emphysematous pyelonephritis and what is a key imaging modality?
Name the typical patient group and a key feature of xanthogranulomatous pyelonephritis.
What is the described management for xanthogranulomatous pyelonephritis?
Provide the Bosniak class management recommendations for Bosniak 3 and Bosniak 4 renal lesions.
Give two key facts about angiomyolipoma from the notes.
Supplementary image: page from the study notes discussing pyelonephritis and benign renal tumours.
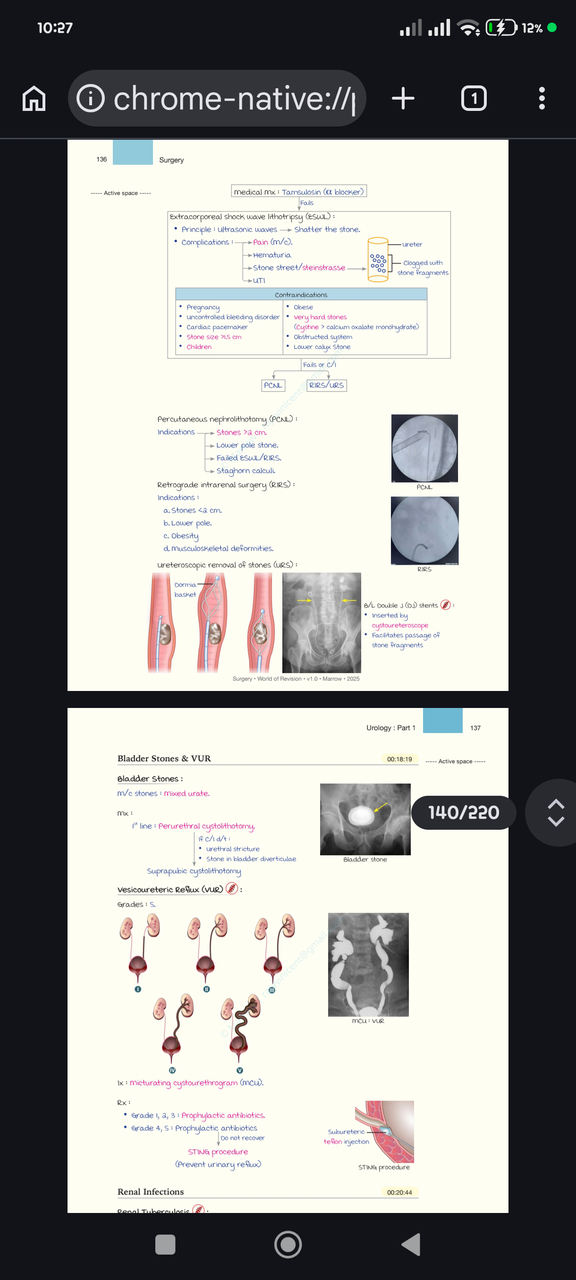
What medical management drug is listed for urinary stone treatment?
What is the principle of Extracorporeal Shock Wave Lithotripsy (ESWL)?
What is the most common complication after ESWL?
Name other complications or consequences associated with ESWL.
What does 'stone street' (steinstrasse) refer to after lithotripsy?
List two contraindications to performing ESWL mentioned in the notes.
Where can an illustrative image of ESWL and related procedures be found for review?
Flashcards in this deck (61)
-
Which subtype of renal cell carcinoma has the worst prognosis?
- Collecting duct RCC has the worst prognosis.
prognosis rcc -
Which renal cell carcinoma subtype is associated with sickle cell anemia?
- Medullary RCC is associated with sickle cell anemia.
rcc associations -
What is the most common presenting symptom of renal cell carcinoma and its approximate frequency?
- Hematuria; most common, present in about 50% of cases.
rcc presentation -
What classic symptom triad can occur in renal cell carcinoma and how often does it appear?
- Hematuria + pain + mass; the triad occurs in about 15% of cases.
rcc presentation -
Name two common paraneoplastic findings in renal cell carcinoma.
- Raised ESR (most common)
- Hypercalcemia
rcc paraneoplastic -
What is Stauffer syndrome in the context of renal cell carcinoma?
- Nonmetastatic hepatic dysfunction associated with RCC (Stauffer syndrome).
rcc stauffer -
What investigation is listed as the investigation of choice (IOC) for renal cell carcinoma?
- CECT (contrast-enhanced CT) is the investigation of choice.
rcc investigation -
Which organ is the most common site of metastasis for renal cell carcinoma?
- Lungs are the most common site of metastasis.
rcc metastasis -
How is T1 stage of renal cell carcinoma defined in the provided staging?
- T1: tumor <7 cm confined to the kidney.
staging rcc -
How is T2 stage of renal cell carcinoma described in the provided staging?
- T2: listed as 77 cm confined to the kidney (as written).
staging rcc -
What structures are removed in a radical nephrectomy according to the notes?
- Kidney with Gerota's fascia
- Ipsilateral adrenal gland (1/L)
- Para-aortic lymph nodes
- Ureter till the brim
surgery nephrectomy -
What are the indications for partial nephrectomy listed in the notes?
- T1 tumours (<7 cm)
- Tumour restricted to poles
surgery partialnephrectomy -
What is the most common paediatric renal malignancy and common abdominal malignancy in children?
- Wilms tumour is the most common paediatric renal malignancy and the most common abdominal malignancy in children.
wilms paediatrics -
Typical age and a presenting sign for Wilms tumour?
- Age: 2–5 years
- Sign: Hematuria
presentation wilms -
How does Wilms tumour help differentiate from neuroblastoma by abdominal mass behavior?
- Wilms tumour mass does not cross the midline, which helps differentiate it from neuroblastoma.
wilms differential -
Name three familial syndromes associated with bilateral Wilms tumour.
- Beckwith-Wiedemann syndrome
- Denys-Drash syndrome
- WAGR syndrome
genetics wilms -
Use the provided image as an illustration: which investigation image is shown for renal cell carcinoma?
Image:
 - CECT image of renal cell carcinoma.rcc image
- CECT image of renal cell carcinoma.rcc image -
What is the usual clinical presentation of angiomyolipoma (AML)?
- Asymptomatic (usually)
angiomyolipoma presentation -
What is Lenk's triad in Wunderlich syndrome related to AML?
- Hypotension
- Flank pain
- Mass
presentation wunderlich lenk -
Which imaging study is listed for evaluation of renal masses like AML and RCC?
- CECT (IOC)
imaging cect -
What is the management for symptomatic angiomyolipoma larger than 4 cm?
- Partial nephrectomy
management angiomyolipoma -
What is the immediate management for a bleeding angiomyolipoma?
- Angioembolisation followed by partial nephrectomy
management angiomyolipoma bleeding -
What are the key histologic features described as 'plant-like' in the notes?
- Plant-like cells with raisin-like nucleus
histology description -
Give two gross or histologic features of oncocytoma listed in the notes.
- Tan/mahogany appearance
- Origin: oncocytes (rich in mitochondria)
oncocytoma features -
Which immunohistochemical marker is noted to help differentiate oncocytoma from chromophobe RCC?
- Cytokeratin
ihc oncocytoma -
What syndrome is associated with multiple bilateral oncocytomas?
- Birt-Hogg-Dube syndrome
oncocytoma syndrome -
List three risk factors for renal cell carcinoma (RCC) mentioned in the notes.
- Diabetes mellitus
- Hypertension
- Tobacco intake
rcc risks -
Which RCC subtype is described as the most common and associated with VHL syndrome?
- Clear cell RCC
rcc clearcell -
Which RCC subtype is noted to contain psammoma bodies and be associated with long-term dialysis?
- Papillary RCC
rcc papillary -
Which RCC subtype is reported to have the best prognosis in the notes?
- Chromophobe RCC
prognosis rcc chromophobe -
What is the most common presenting symptom of RCC and its approximate frequency?
- Hematuria — most common, ~50%
rcc presentation -
Name three paraneoplastic syndromes associated with RCC from the notes.
- Raised ESR
- Hypercalcemia
- Polycythemia
rcc paraneoplastic -
What nonmetastatic hepatic phenomenon is named in association with RCC?
- Stauffer syndrome
rcc stauffer -
According to the notes, where does RCC most commonly metastasize?
- Lungs (most common)
rcc metastasis -
What defines T1 stage of RCC in the provided staging lines?
- T1: <7 cm confined to the kidney
staging rcc -
What is the defining feature of T3 stage in RCC staging provided?
- T3: Extends into major veins
staging rcc -
Which collecting-duct-related RCC variant is noted to have the worst prognosis?
- Collecting duct RCC
prognosis rcc collectingduct -
Which medullary RCC association is mentioned in the notes?
- Medullary RCC: associated with sickle cell anemia
rcc medullary -
Which image file from the provided media shows a CT scan feature of oncocytoma?
- CT scan showing central stellate scar
oncocytoma image - CT scan showing central stellate scar
-
List three early complications of renal tuberculosis shown in the sequence of lesions.
- Papillary ulcer
- Pseudo calculi
- Damaged/ghost calyx
renaltb complications -
What radiological appearance is described by the term 'Putty kidney' in renal tuberculosis?
Accumulation of necrotic pus producing a putty/cement kidney with a non-functioning kidney
renaltb puttykidney -
Name three clinical features associated with a putty/cement kidney.
- Hematuria
- Pain
- Mass
clinical renaltb -
Which investigations are listed for confirming a 'golf-hole' ureteric orifice in renal tuberculosis?
- Centrifuge 3 morning urine samples for AFB staining
- CT urography
renaltb investigations -
What is the first-line medical management for renal tuberculosis?
Anti-tubercular treatment (ATT)
treatment renaltb -
Give one surgical treatment listed for perinephric abscess complicating renal TB.
Drainage with pigtail catheter
surgery renaltb -
What operative procedure is recommended for a golf-hole ureteric orifice?
Ureteric re-implantation
ureter surgery -
What reconstructive procedure is listed for a thimble bladder healed with fibrosis?
Augmentation cystoplasty
surgery bladder -
Which repair is indicated for stricture/shortening of the lower ureter?
Boari flap repair
ureter surgery -
Which organism is most commonly associated with emphysematous pyelonephritis and what is a key imaging modality?
- E. coli
- Contrast-enhanced CT (CECT)
pyelonephritis emphysematous -
Name the typical patient group and a key feature of xanthogranulomatous pyelonephritis.
- Middle-aged females, often with diabetes mellitus
- Flank pain, fever and abdominal mass; non-functioning kidney with low-density masses and stones
pyelonephritis xanthogranulomatous -
What is the described management for xanthogranulomatous pyelonephritis?
Subcapsular nephrectomy
pyelonephritis surgery -
Provide the Bosniak class management recommendations for Bosniak 3 and Bosniak 4 renal lesions.
- Bosniak 3: Indeterminate — partial nephrectomy
- Bosniak 4: Clearly malignant — partial/total nephrectomy
renal bosniak -
Give two key facts about angiomyolipoma from the notes.
- Benign tumour typically in 5th–6th decade
- Origin: perivascular epithelioid cells; bilateral multiple lesions seen in tuberous sclerosis
angiomyolipoma tumour -
Supplementary image: page from the study notes discussing pyelonephritis and benign renal tumours.
 - Image is supplementary; facts must be answered without viewing it.image reference
- Image is supplementary; facts must be answered without viewing it.image reference -
What medical management drug is listed for urinary stone treatment?
- Tamsulosin — a blocker
stones urology medical -
What is the principle of Extracorporeal Shock Wave Lithotripsy (ESWL)?
- Ultrasonic waves that shatter the stone
treatment eswl urology -
What is the most common complication after ESWL?
- Pain (most common)
eswl complications -
Name other complications or consequences associated with ESWL.
- Hematuria
- Steinstrasse (stone street)
- Urinary tract infection (UTI)
stones eswl complications -
What does 'stone street' (steinstrasse) refer to after lithotripsy?
- Ureter clogged with stone fragments
eswl complications steinstrasse -
List two contraindications to performing ESWL mentioned in the notes.
- Pregnancy
- Uncontrolled bleeding disorder
eswl contraindications -
Where can an illustrative image of ESWL and related procedures be found for review?
- See image:
eswl visual resources - See image:
Renal tumours — quick overview
- Renal tumours include malignant (RCC subtypes, collecting-duct, medullary) and benign (oncocytoma, angiomyolipoma) lesions.
- Investigation of choice for solid renal masses: Contrast-enhanced CT (CECT).
Renal cell carcinoma (RCC)
Key clinical features
- Classic triad: hematuria (≈50%), flank pain, palpable mass (triad present in ~15%).
- Other signs: weight loss, fever, paraneoplastic syndromes (↑ESR common, hypercalcemia, hypertension, polycythemia, Cushing's, Stauffer syndrome — reversible hepatic dysfunction).
- Metastasis: lungs most common.
Subtypes & important associations
- Clear cell RCC — most common; arises from proximal tubules; associated with VHL syndrome.
- Papillary RCC — often shows psammoma bodies; associated with long-term dialysis.
- Chromophobe RCC — best prognosis; histology shows pale cells.
- Collecting-duct / Medullary RCC — worst prognosis; medullary RCC associated with sickle cell trait/disease.
Imaging and pathology
- CECT: mass often arises from upper or lower pole and may extend into renal vein/IVC.
- Histology clues: "clear cells" for clear-cell, papillary architecture for papillary, eosinophilic oncocytes for oncocytoma (benign).
Alt: Page of notes on RCC staging and features
Staging (tumour extent — TNM T categories summarized)
- T0: No evidence of primary tumor.
- T1: Tumor ≤ 7 cm, confined to kidney.
- T2: Tumor > 7 cm, confined to kidney.
- T3: Tumor extends into major veins or perinephric tissues but not beyond Gerota's fascia.
- T3a: Into renal vein or its segmental branches.
- T3b: Into IVC below diaphragm (subdiaphragmatic).
- T3c: Into IVC above diaphragm (supradiaphragmatic) or invades vena cava wall.
- T4: Invades beyond Gerota's fascia and/or involves ipsilateral adrenal gland.
Management principles
- Partial nephrectomy (nephron-sparing): indicated for T1 (≤7 cm), especially polar/small tumours.
- Radical nephrectomy: remove kidney with Gerota's fascia, ipsilateral adrenal when involved, regional nodes (e.g., para‑aortic), and ureter to the pelvic brim when indicated.
- Ablative therapies (cryoablation/RFA): option for small tumours (<4 cm) in solitary kidney, bilateral disease, or unfit patients.
- Systemic therapy (targeted/immunotherapy) for advanced/metastatic disease; RCC historically less chemo/radio-sensitive.
Benign renal tumours
Oncocytoma
- Most common benign renal tumour; originates from oncocytes (many mitochondria).
- CT clue: central stellate scar; gross: tan/mahogany colour.
- Associated with Birt–Hogg–Dubé syndrome (multiple oncocytomas).
- Management: often partial nephrectomy if imaging/indication uncertain (Bosniak 3/indeterminate).
Alt: Notes page on oncocytoma and RCC
Angiomyolipoma (AML)
- Benign tumour of perivascular epithelioid cells containing fat, muscle, and vessels.
- Often sporadic; bilateral/multiple AMLs suggest tuberous sclerosis.
- Presentation: usually asymptomatic; can present with spontaneous retroperitoneal hemorrhage (Wunderlich syndrome) when large.
- Treatment: observe small asymptomatic lesions; intervene when >4 cm or symptomatic — options include selective angioembolisation or partial nephrectomy.
Wilms tumour (nephroblastoma)
- Most common pediatric renal malignancy; peak age 2–5 years.
- Presents as abdominal mass; usually does not cross midline (helps differentiate from neuroblastoma).
- Associated syndromes: WAGR, Beckwith–Wiedemann, Denys–Drash.
- Investigations: CECT for staging.
- Management: chemo + surgery ± radiotherapy — Wilms is chemo- and radio-sensitive (different from RCC which is resistant).
Renal tuberculosis — key complications & management
- Early lesion: papillary ulceration; progression can produce pseudo‑calculi, damaged (ghost) calyx, perinephric abscess, and putty/calcified kidney (nonfunctional).
- Ureteric sequelae: strictures, shortening, kinking, and the golf‑hole ureteric orifice.
- Bladder sequela: thimble bladder (fibrotic small-capacity bladder) — may need augmentation.
- Diagnosis: three early-morning urine AFBs / mycobacterial culture and CT urography.
- Medical: standard anti-tubercular therapy (ATT). Surgical options based on complications: drainage of abscess, ureteric re-implantation, Boari flap for lower ureter shortening, augmentation cystoplasty for small bladder.
Alt: Page with pyelonephritis and benign renal tumour notes
Pyelonephritis — specific forms
- Emphysematous pyelonephritis: gas-forming infection (commonly E. coli), seen in diabetics/immunocompromised; treat with antibiotics and percutaneous drainage, nephrectomy if refractory.
- Xanthogranulomatous pyelonephritis: chronic destructive infection (often Proteus), associated with staghorn calculi and non-functioning kidney; treatment often subcapsular nephrectomy.
Bosniak classification (renal cysts — imaging‑based management)
- I: Simple cyst — benign; no follow-up needed.
- II / IIF: Minimally complex; IIF requires imaging follow-up.
- III: Indeterminate cystic lesion — consider partial nephrectomy (surgical exploration).
- IV: Clearly malignant features (enhancing soft‑tissue components) — treat as renal cancer (partial/total nephrectomy).
Stones — ESWL (brief)
- ESWL principle: focused shock waves fragment stones noninvasively.
- Common complications: pain, hematuria, urinary tract infection, and "stone‑street" (ureter clogged with fragments).
- Contraindications include pregnancy and uncontrolled bleeding diatheses.
High-yield facts (for exams/recall)
- RCC classic triad: hematuria, flank pain, mass (triad uncommon).
- CECT is investigation of choice for renal masses.
- Partial nephrectomy is preferred for tumours ≤ 7 cm (T1) when feasible.
- Wilms tumour: common in children 2–5 years, usually chemo-sensitive and does not cross midline.
- Angiomyolipoma >4 cm or symptomatic → treat (embolisation or surgery).
- Emphysematous pyelonephritis occurs in diabetics and may require nephrectomy if drainage/antibiotics fail.