Save your deck before it's gone
These flashcards aren't stored yet — they'll disappear when you leave. Create a free account to keep them, and unlock everything below.
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model












What divides the liver into the right and left lobes?
The falciform ligament separates the liver into right and left lobes.
What is Cantlie's Line?
Cantlie's Line is a functional division of the liver, along the gallbladder fossa and inferior vena cava.
What surrounds the bare area of the liver?
The bare area is not covered by Glisson's capsule.
What segments form the left hemiliver?
- Segment II
- Segment III
- Segment IV
What are the four sections of the liver based on the hepatic artery?
- Right anterior section (segments V & VIII)
- Right posterior section (segments VI & VII)
- Left medial section (segment IV)
- Left lateral section (segments II & III)
The liver can be divided into 8 functional segments also known as Couinaud segments.
Which ligament is not part of the liver anatomy?
Bare Area
Right Triangular Ligament
Falciform Ligament
Coronary Ligament
What is the primary purpose of the caudate lobe?
The caudate lobe contains 3 sub-segments: spiegel lobe, paracaval, and caudate process.
What does the liver weigh approximately?
The liver weighs about 1.5 kg.
What ligament is a remnant of the obliterated umbilical vein?
The Round Ligament (ligamentum teres).
What ligaments attach the liver to the anterior abdominal wall?
- Falciform Ligament
- Coronary Ligament
- Left and Right Triangular Ligament
What supplies 75% of the liver's blood?
The portal vein.
What is the primary arterial blood supply to the liver?
The hepatic artery proper (25%).
What drains segment V, VI, VII, and VIII of the liver?
The Right hepatic vein.
What anatomical variant arises from the SMA?
Replaced right hepatic artery (10-15%).
How do segment V & VIII drain into the liver?
Via the right anterior sectoral duct (RASD).
The three main hepatic veins form sagittal planes and include the Right hepatic vein, Middle hepatic vein, and Left hepatic vein.
The portal vein divides into the right and left portal vein branches.
What is the significance of the caudate lobe's venous drainage?
It drains directly to the IVC.
What drains the segments VI and VII of the liver?
The right posterior sectoral duct (RPSD).
What is a common anatomical variant involving the biliary system?
RPSD draining into LHD (15%).
What stimulates the contraction of the gallbladder?
CCK (Cholecystokinin)
What are the two factors governing bile secretion?
- Enterohepatic circulation
- Gut hormones (CCK & secretin)
What is the consequence of a lack of bile?
Malabsorption of fats and fat-soluble vitamins (A, D, E, K)
Bile is diverted from the liver into the gallbladder due to high tone in the sphincter of Oddi.
What is the role of the liver in carbohydrate metabolism?
- Glycogenesis
- Glycogenolysis
What process occurs to amino acids during starvation?
Gluconeogenesis - conversion back to glucose
What is lipogenesis?
Conversion of glucose to glycerol + FFA forming TG (triglycerides)
What is the Cori Cycle?
Lactate is converted to glucose in the liver and returned to the muscle.
What vitamin is activated in a two-stage hydroxylation process?
Vitamin D
What is synthesized in the liver besides immunoglobulin?
Plasma proteins such as albumin and clotting factors.
What regulates iron homeostasis?
The synthesis of Hepcidin in the liver.
Which cells in the liver are responsible for phagocytosis?
Kupffer cells.
What is the role of the liver in detoxification?
Detoxify peptide hormones, drugs, and toxins.
What forms the main storage for fat-soluble vitamins?
- Vitamin A
- Vitamin D
- Vitamin E
- Vitamin K
- Vitamin B12
What substance is converted by the liver in the Cori Cycle?
Fatty acids
Lactate
Amino acids
Glucose
What is the definition of portal hypertension?
Portal Hypertension is defined as the Hepatic venous pressure gradient (HVPG) ≥ 6mmHg. Normal is 3-5mmHg.
What is the normal portal flow rate?
1-1.5 L/min is the normal portal flow rate.
What indicates high risk of developing gastroesophageal varices?
Portal HTN ≥ 10mmHg indicates high risk of gastroesophageal varices.
What pressure level poses a high risk for variceal bleed?
Portal HTN ≥ 12mmHg indicates high risk of variceal bleed.
Which organs are drained by portal veins?
- Small intestines
- Large intestines
- Stomach
- Spleen
- Pancreas
- Gallbladder
What forms the portal vein?
The SMV and the splenic vein unite behind the neck of the pancreas to form the portal vein.
The portal trunk divides into two lobar veins: the right branch that drains the cystic vein and the left branch which drains the umbilical and paraumbilical vein (caput medusae in portal HTN).
What is a consequence of portal hypertension due to cirrhosis?
Portal hypertension results from mechanical obstruction of the portal venous system.
What are the key issues with cirrhosis affecting portal hypertension?
- Architecture distortion
- Regenerative parenchymal nodules
- Disruption of liver architecture
According to Ohm's Law, the relationship between voltage (V), current (I), and resistance (R) is given by: V = IR. Poiseuille's Law states that R = 8hL/pr^4.
What impact does decreasing portal vascular radius have on resistance?
Dramatic increase in portal vascular resistance occurs with decreased vascular radius.
The diagram illustrating portal hypertension pathophysiology and collateral circulation shows key elements such as splanchnic vasodilation and TIPS (Transjugular Intrahepatic Portosystemic Shunt). 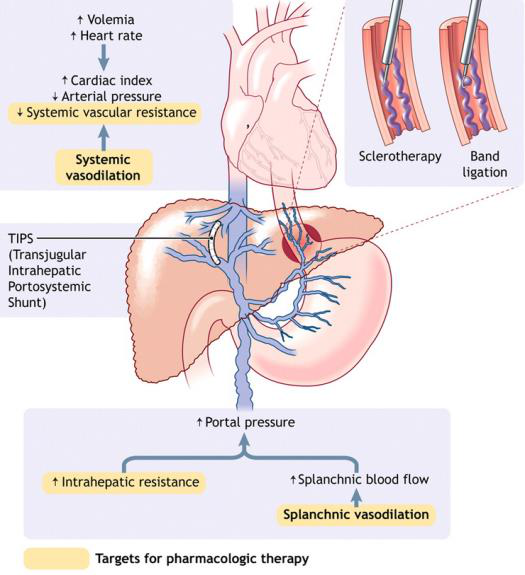
Illustration of the liver and its venous drainage highlights esophageal, paraumbilical, and rectal varices. 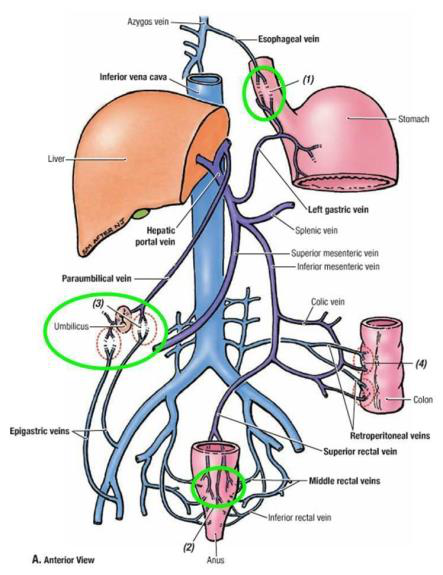
What is a major cause of pre-sinusoidal portal hypertension?
- Portal Vein Thrombosis
- Splenic Vein Thrombosis
- Congenital Atresia
What is a common cause of sinusoidal portal hypertension?
- Cirrhosis
- Massive Fatty Change
- Hemochromatosis
What are some causes of post-sinusoidal portal hypertension?
- Hepatic vein thrombosis
- IVC thrombosis
- Congenital IVC malformation
What condition is associated with Budd Chiari Syndrome?
Rare thromboembolic disorder of hepatic veins/IVC leading to post-sinusoidal portal hypertension.
What are key ultrasound findings for portal hypertension?
- Dilated splenic & superior mesenteric veins ≥ 11mm
- Splenomegaly > 12cm
- Dilated portal vein ≥ 13mm
In portal hypertension, ascites occurs due to: increased fluid shift leading to increased lymphatic drainage from liver which overwhelms thoracic duct capacity, resulting in percolation of hepatic lymph into the peritoneal cavity.
What is a significant complication of portal hypertension?
- Ascites
- Hepatic Encephalopathy
- Portal Hypertensive Gastropathy
What causes spontaneous bacterial peritonitis (SBP) in ascites?
Chronic alcoholism
Dilated portal vein
Hemochromatosis
Increased fluid shift (Starling's law)
What are some symptoms of Hepatic Encephalopathy?
- Hyperammonemia
- Neuro-toxicity
- Exacerbated by portosystemic shunting
Which anatomical area is affected by oesophageal varices?
Portal circulation through oesophageal branch of left gastric vein.
What is Caput Medusae related to?
Varicosity caused by systemic circulation through superficial epigastric veins.
What does progressive liver cirrhosis lead to?
Obstruction of intra-hepatic vasculature causing portal hypertension.
What is released due to portal HTN in cirrhotic patients?
Increased splanchnic nitric oxide (NO).
What stimulates RAAS in cirrhotic patients?
Renal hypoperfusion.
What is the effect of aldosterone in ascites treatment?
Increases retention of salt and water.
What is the diuretic of choice for cirrhotic patients with ascites?
Spironolactone (aldosterone antagonist).
What are common symptoms of ascites?
- Progressive abdominal distension
- Weight gain
- Shortness of breath
- Early satiety
What physical signs confirm the diagnosis of ascites?
- Abdominal distension
- Flank dullness
- Shifting dullness
- Umbilical eversion
What does the SAAG ≥ 1.1g/dL indicate?
Porta hypertension; common cause is liver cirrhosis.
What can a SAAG <1.1g/dL indicate?
Malignancy or infection such as peritoneal tuberculosis.
What investigations are performed for suspected ascites?
- Biochemical tests (FBC, U/E/Cr, LFT)
- Imaging (Ultrasound/CT)
What does a peritoneal tap assess?
Fluid color and appearance to distinguish between conditions.
What is the common indication for a peritoneal tap in ascites?
Diagnostic
Curative
Preventive
Therapeutic
What is a common microbiological test for ascitic fluid?
Gram stain smear, culture (aerobic / anaerobic), cytology
What are the laboratory tests included in the analysis of ascitic fluid?
- LDH
- TG
- Glucose
- TB culture
- ProBNP
What is the recommended low salt diet for ascites?
2000mg / day or 88mol/day
When should fluid restriction be considered?
If serum sodium <125mmol/L
What is the typical pharmacological treatment for diuresis in ascites?
- Spironolactone 100mg
- Furosemide 40mg (Max 400mg:160mg)
What is the recommended antibiotic for suspected spontaneous bacterial peritonitis?
IV ceftriaxone or oral quinolones (e.g., ciprofloxacin)
What is the purpose of therapeutic paracentesis?
To manage tense ascites and prevent complications.
What is the procedure for therapeutic paracentesis?
- Site: 2FB above and 2FB lateral to ASIS
- Use aseptic technique, LA, US-guided
Why is albumin administered after paracentesis?
To prevent paracentesis-induced circulatory dysfunction.
What surgical options are available for liver disease-related ascites?
- Liver transplantation
- Transjugular Intrahepatic Porto-Systemic Shunts (TIPSS)
- Peritoneovenous shunts
What should be controlled pre-operatively in cirrhotic patients?
Ascites
What is the risk of abdominal operations in patients with advanced cirrhosis?
High risk of complications, especially portal hypertension.
What is performed prior to major abdominal operations in high MELD score patients?
Transjugular Intrahepatic Portosystemic Shunt (TIPSS).
What does hepatomegaly refer to?
Hepatomegaly refers to the abnormal enlargement of the liver.
What are common symptoms of hepatomegaly?
- Asymptomatic
- Abdominal pain
- Nausea, vomiting
- Fever
- Signs of jaundice
What should a clinical examination for hepatomegaly include?
- Palpable organomegaly
- Tenderness
- Signs of ascites
- Digital Rectal Examination
Common presentations of hepatomegaly include: abdominal pain, nausea, vomiting, and fever.
What are signs of chronic liver disease?
- Gynaecomastia
- Clubbing of fingernails
- Palmar erythema
- Lower limb edema
What is a common risk factor for malignant lesions in hepatomegaly?
Ongoing weight loss
Sudden fever
History of liver cirrhosis
High blood pressure
Symptoms of portal hypertension may include splenomegaly and ascites.
What is a physiological cause of liver abnormalities?
Riedel's Lobe Hyperextended Chest
Name a bacterial infection that can affect the liver.
Pyogenic Liver Abscess Tuberculosis
Which viral infections are known to affect the liver?
Hepatitis EBV CMV HIV
What are some alcohol-related liver conditions?
Fatty Liver Cirrhosis
Which metabolic diseases can affect the liver?
Wilson's Disease Haemochromatosis Infiltration - amyloidosis
What are some malignant liver conditions?
Hepatocellular Carcinoma Hepatic Angiosarcoma Cholangiocarcinoma
What is a vascular/cardiac disorder that affects the liver?
Right Heart Failure (RHF) Budd-Chiari Syndrome
A benign hepatic neoplasm can be a Haemangioma, Hepatic Adenoma, or Focal nodular Hyperplasia.
What types of hepatic abscesses exist?
Pyogenic Abscess Amoebic Abscess
What are the two types of hepatic cysts?
Non Parasitic Cyst Echinococcal Cysts
Intrahepatic obstruction causes of portal hypertension include Cirrhosis and Wilson's Disease.
What is a post-hepatic obstruction condition for portal hypertension?
Budd-Chiari Syndrome IVC Thrombosis
Factors associated with Hepatic Angiosarcoma include exposure to vinyl chloride, arsenic.
What is a Full Blood Count used for?
To detect any anemia or signs of infections.
What does a Liver Function Test indicate?
Presence of hyperbilirubinemia and deranged liver enzymes.
What are Tumour Markers used for?
Their presence can indicate suspicion of malignancy.
What imaging techniques are used for liver examination?
- Ultrasound Liver
- CT Scan
- MRI
An Ultrasound of the liver can reveal a simple cyst as: - well defined smooth walls - posterior acoustic enhancement.
A CT Scan of a haemangioma shows: - early peripheral nodular enhancement - centripetal filling.
The MRI of a Hepatic Adenoma reveals: - hypervascular enhancement on arterial phase - lack of central scar.
In Focal Nodular Hyperplasia (FNH), the Doppler appearance shows: - central feeding artery - tortuous spoke-wheel vascularity.
For Hepatocellular Carcinoma (HCC), imaging might show: - hypervascular enhancement on arterial phase - portal venous washout.
Which imaging technique is NOT typically used for liver examination?
CT Scan
MRI
Endoscopy
Ultrasound Liver
What are liver hemangiomas characterized by?
Benign vascular lesions consisting of widened (dilated) blood vessels, not true neoplasms.
What is the female to male ratio for liver hemangiomas?
5-6:1, predominantly in middle-aged women.
What is the usual presentation of a liver hemangioma?
Usually asymptomatic; may cause nonspecific abdominal pain when larger than 5cm.
What imaging technique is most accurate for liver hemangiomas?
Ultrasound, with 70-80% accuracy and pathognomonic compressibility of the lesion.
What does a CT scan of a hemangioma show?
Peripheral enhancement in the arterial phase and peripheral to central enhancement over time.
The majority of liver hemangiomas are treated with observation if they are asymptomatic and smaller than 4cm.
What should never be done for diagnosing liver hemangiomas?
Biopsy, due to risk of severe and fatal hemorrhage.
What syndrome is associated with large hemangiomas?
Kasabach-Merritt syndrome, which leads to thrombocytopenia and consumptive coagulopathy.
What is a common treatment for symptomatic or complicated liver hemangiomas?
Radiation therapy
Surgical removal
Observation
Chemotherapy
What are the symptoms of large liver hemangiomas?
- Nonspecific abdominal fullness
- Abdominal pain
- Rarely, life-threatening hemorrhage
What is the definition of Focal Nodular Hyperplasia (FNH)?
FNH is a benign tumour characterized by a central stellate scar and is considered a regenerative process, not a result of arterial malformation.
What is the epidemiology of FNH?
- Second commonest benign liver tumour
- More common in females (6-8:1) aged 30 to 50 years
- Associated with AVMs and hepatic haemangioma.
What symptoms are associated with FNH?
- Asymptomatic (incidental on imaging)
- Right upper quadrant pain
- Rarely ruptures or bleeds.
How is FNH diagnosed?
- CT: Bright homogenous enhancement, hypoattenuating central scar.
- Sulphur colloid scan: Positive for kupffer cells.
- MRI: Central scar hyperintense on T2 weighted images.
What is the treatment for FNH?
- Conservative management for asymptomatic patients.
- Surgery for symptomatic patients, with liver resection preferred.
FNH is a benign tumour characterized by a central stellate scar and is considered a regenerative process.
FNH is the second commonest benign liver tumour, more common in females aged 30 to 50 years.
Symptoms of FNH include: - asymptomatic - right upper quadrant pain.
Diagnosis of FNH involves: - CT with bright enhancement and hypoattenuating scar - sulphur colloid scan - MRI.
FNH treatment options are: - conservative management for asymptomatic patients - surgery for symptomatic patients.
What are hepatic adenomas?
Benign proliferation of hepatocytes; should not be confused with hepatoma (HCC).
What is the female to male ratio for hepatic adenomas?
10:1, primarily found in young women.
What are common presentations of hepatic adenomas?
Asymptomatic or symptomatic with spontaneous rupture and intraperitoneal hemorrhage.
What percentage of hepatic adenomas may rupture?
25-35%, with nearly 100% of ruptures in lesions >5cm.
What are common diagnosis methods for hepatic adenomas?
CT (triphasic), sulphur colloid scan, and MRI.
What is the treatment for small, asymptomatic hepatic adenomas?
Conservative management with close observation and possible discontinuation of OCPs.
What is indicated for symptomatic hepatic adenomas or those >4-5cm?
Surgical resection.
Hepatic adenomas are characterized by a benign proliferation of hepatocytes, distinct from hepatoma which refers to HCC.
The risk factors for hepatic adenomas include anabolic steroids, oestrogen, and progesterone preparation (e.g., OCP).
A significant risk of hepatic adenomas is malignant transformation to well-differentiated HCC, with a risk of ~5%.
What characteristic is NOT associated with imaging findings in hepatic adenomas?
No true lobules
Sharply defined borders
More common in right lobe
Homogenous enhancement during arterial phase
What should be done if a patient has an acute hemorrhage from hepatic adenoma?
Discontinue all medications
Proceed to hepatic angioembolization followed by surgery
Immediate liver transplant
Complete bed rest without intervention
What are liver cysts commonly detected through?
Imaging, as they are mostly asymptomatic.
What percentage of liver cysts are simple ones?
5-20%
Nonparasitic liver cysts include: - Simple Liver Cysts - Polycystic Liver Disease - Neoplastic Cysts - Echinococcal Cysts.
What symptoms may occur due to symptomatic liver cysts?
- RUQ tenderness - Palpable Hepatomegaly - Bleeding, Infection, Torsion, Rupture
What are common complications of a simple liver cyst?
- Infection - Intracystic hemorrhage - Pain
What is a common extrahepatic manifestation of Polycystic Liver Disease?
Kidney Stones
Heart Disease
Lung Cancer
Cerebral Aneurysm
What management is used for symptomatic simple liver cysts?
- Percutaneous aspiration with sclerotherapy - Laparoscopic 'unroofing'
Neoplastic cysts can include: - Cystadenoma - Cystadenocarcinoma - IPMN-B.
What is a potential treatment for suspected cystadenoma?
Formal resection or enucleation.
What can blunt trauma lead to regarding liver cysts?
Intra-hepatic hematomas or bilomas developing into traumatic hepatic cysts.
What should be done for suspected cystic malignancies?
Proceed with biopsy or formal hepatic resection.
What is the primary cause of Cystic Echinococcosis?
Infestation with tapeworm of the genus Echinococcus, primarily E. granulosus.
What is a definitive host for Echinococcus?
Dogs serve as the definitive hosts for Echinococcus.
What can humans be classified as regarding Echinococcus?
Humans are considered dead-end hosts for Echinococcus.
What are common organs affected by hydatid cysts?
- Liver
- Lung
- Bone
- Kidney
- Spleen
- CNS
What is the first-line imaging technique for diagnosing hydatid cysts?
Ultrasound is the first-line imaging technique for diagnosing hydatid cysts.
What serological tests can aid in the diagnosis of Echinococcosis?
- Immunoelectrophoresis
- ELISA
What is the percutaneous treatment technique for hydatid cysts?
The PAIR technique (Puncture, Aspiration, Injection, Re-aspiration) is used.
What risks are associated with the PAIR technique for treating hydatid cysts?
- Anaphylactic shock
- Secondary echinococcosis
- Chemical cholangitis
- Biliary fistula
What surgical options are available for treating hydatid cysts?
- Radical: pericystectomy
- Conservative: unroofing of cyst
What medications are used to treat Echinococcosis?
Albendazole +/- praziquantel are used for treatment.
What is the treatment approach for inactive silent cysts?
The approach is typically to watch and wait.
What is Alveolar Echinococcosis primarily treated with?
Radical Liver Resection or Liver Transplantation.
What is the annual incidence of hepatocellular carcinoma (HCC) in Singapore for males?
18 / 100,000
What is the annual incidence of hepatocellular carcinoma (HCC) in Singapore for females?
4.6 / 100,000
HCC is the 4th most frequent cancer death among which gender?
Females
Hepatocellular carcinoma is primarily diagnosed in what decades of life?
Fifth and sixth decades
What percentage of liver cancers are HCCs?
85%
What is the most common risk factor for developing HCC?
Chronic liver disease (CLD)
What virus infection is associated with increased HCC risk due to DNA damage?
Hepatitis B Virus (HBV)
The risk of HCC approaches 2-4% annually in patients with which condition?
Cirrhosis
Alcoholic cirrhosis increases the risk of HCC by how many times?
5 times
Chronic Hepatitis C accounts for what fraction of HCC cases in the USA?
1/3
Non-alcoholic steatohepatitis (NASH) increases the risk of HCC by 20x.
Diet high in red meat and saturated fats is linked to what cancer?
Hepatocellular carcinoma (HCC)
What toxin found in moldy food is linked to HCC?
Aflatoxins B1
Chronic HBV along with which lifestyle factor has a synergistic effect on HCC risk?
Alcohol consumption
What condition is characterized by inflammation of the biliary tree often leading to HCC?
Primary Sclerosing Cholangitis
Recurrent infection in the biliary tree due to pyogenic cholangitis can lead to which cancer?
Hepatocellular carcinoma (HCC)
What is the process of pathogenesis associated with?
- Chronic inflammatory process
- Ongoing hepatocellular damage
- High cellular regeneration leading to genetic mutation accumulation
What classification represents worse clinical outcomes?
- Proliferative Class
- Associated with HBV infection
- High AFP levels
- High tumor grade
What factors characterize the Non-proliferative Class?
- Non-proliferative Class
- HCV infection
- Alcohol abuse
- Low tumor grade
- Better clinical outcomes
What are the histological subtypes of liver cancer?
- Non-Fibrolamellar
- Fibrolamellar (FLC) - more common in younger patients, no Hep B association
What are the main characteristics of liver cirrhosis?
- Bridging fibrosis
- Regenerative parenchymal nodules
- Disruption of liver architecture
How often should patients with cirrhosis undergo monitoring?
- Every 6 months
- Ultrasound of the liver
- Serum AFP measurement
What is the MELD score used for?
- Predicting prognosis in cirrhosis patients
- Assessing mortality risk after TIPSS
- Prioritizing liver transplantation
What factors are included in the MELD score calculation?
- Serum bilirubin
- INR
- Serum creatinine
- Constant for liver disease etiology
What does a MELD score of 15 indicate?
- 6% mortality risk at 3 months
What outcomes are best with a MELD score less than 14?
- Best outcomes with TIPSS
- Poor outcomes with scores >24
What does an increase in MELD points indicate?
- Post-op mortality risk increases by 1% for each point up to 20
- Increases by 2% for each point above 20
What criteria are included in the PELD score?
- Age
- Presence of growth failure
- Albumin instead of creatinine
What is the typical presentation of patients with HCC during screening?
Patients are often asymptomatic. HCC can be an incidental finding during ultrasound screening for chronic hepatitis B.
What are common local signs & symptoms of HCC?
- Upper abdominal pain (dull & persistent)
- Early satiety/vomiting
- Constitutional symptoms: low energy, loss of appetite, malaise
- Pyrexia
- Jaundice (5-10%)
Patients with HCC may experience upper abdominal pain, early satiety/vomiting, and constitutional symptoms such as low energy, loss of appetite.
What is Budd-Chiari syndrome?
It is the occlusion of hepatic, intrahepatic, or portal veins causing portal hypertension and congestive hepatopathy, often leading to ascites.
What are the features of decompensated chronic liver disease?
- Worsening liver function
- Hepatic encephalopathy
- Jaundice
- Ascites
- Spontaneous bacterial peritonitis
What is a possible severe complication of a liver tumor?
Hepatic fibrosis
Cirrhosis
Hepatocellular carcinoma
Tumour rupture
What symptoms are associated with portal hypertension?
- Ascites
- Lower limb oedema
- Haematemesis
- Congestive splenomegaly
Portal hypertension can present with symptoms such as ascites, lower limb oedema, and haematemesis.
What are paraneoplastic syndromes associated with HCC?
- Hypoglycemia
- Erythrocytosis
- Hypercalcemia
Common paraneoplastic syndromes include hypoglycemia due to high metabolic demands and erythrocytosis from tumour-produced erythropoietin.
What is Hepatorenal Syndrome (HRS)?
A reversible form of acute renal failure in a patient with advanced liver disease without identifiable renal pathology.
What are the two types of Hepatorenal Syndrome?
- Type 1: Rapid renal function impairment, doubling serum creatinine > 221 in < 2 weeks.
- Type 2: Subtle course, serum creatinine < 221, develops diuretic-resistant ascites.
What leads to the renal hypoperfusion in HRS?
- Advanced cirrhosis leads to portal hypertension & splanchnic arterial vasodilation
- Decreased vascular resistance causes effective arterial hypovolemia.
What is the initial therapy for Hepatorenal Syndrome?
- Octreotide
- Midodrine
- Vasopressin analogue.
- Can progress to dialysis dependence.
What can reverse Hepatorenal Syndrome?
Liver transplant, even after dialysis dependence.
What are common causes of Hepatic Encephalopathy?
- High nitrogenous waste (BGIT)
- Infections (e.g., sepsis)
- Medications (e.g., benzodiazepines)
- Electrolyte imbalances.
- High protein diet.
What is Stage 0 of Hepatic Encephalopathy?
Lack of detectable changes in personality or behavior.
What characterizes Stage 1 of Hepatic Encephalopathy?
- Shortened attention span
- Impaired math skills
- Hypersomnia or insomnia
- Asterixis can be detected.
What are the symptoms of Stage 3 Hepatic Encephalopathy?
Gross disorientation, semi-stupor to stupor, bizarre behaviors.
What is the treatment for Hepatic Encephalopathy?
- Lactulose
- Low protein diet (<70g/day)
- Branched-chain amino acids.
- Neomycin for ammonia-producing bacteria if required.
What is the gold standard diagnostic approach for hepatocellular carcinoma?
A triphasic CT scan with arterial and portal venous phase contrast imaging.
What does the arterial phase of a triphasic CT scan show?
Early enhancement with lesions appearing hyper-dense relative to hypo-dense hepatic parenchyma.
What indicates tumor washout in a triphasic CT scan?
Hypo-density of a nodule in the delayed phase compared to surrounding hepatic parenchyma.
The radiological hallmark of HCC includes: arterial hypervascularity and venous/late phase washout.
What does HCC's tendency to invade the portal vein indicate?
An enhancing portal vein thrombus.
What is the role of a lipiodol contrast CT scan?
To detect areas of tumor that may not be clear in pre-lipiodol CT, as lipiodol is retained in HCC.
What is the significance of detecting Alpha-FetoProtein (AFP) levels?
A rise in serum AFP in a cirrhosis patient suggests the development of HCC.
What imaging modality is most accurate for distinguishing HCC from dysplastic nodules?
MRI scan (dynamic, contrast-enhanced).
What are the complications to assess during HCC diagnosis?
Tumor burden, liver function, and patient's performance status.
What does the MRI appearance of HCC typically show?
Highly intense on T2 images and low-intensity on T1-weighted images.
What is the role of ultrasound in liver cirrhosis?
Ultrasonography is often used for screening in the setting of liver cirrhosis.
What is detected using contrast-enhanced ultrasound in HCC?
It is used for detecting arterial enhancement in HCC.
What may biopsies risk during HCC assessment?
Biopsies have a risk of bleeding and needle tract seeding.
What does the Child-Pugh Score assess?
It assesses liver function using LFTs + PT/INR/APTT.
What is the maximum surgical mortality for Class B in Child-Pugh Score?
The surgical mortality for Class B is 20-30%.
What does a Class C rating in Child-Pugh Score signify?
Class C indicates not for resection and a surgical mortality of 75-80%.
What indicates post-resection liver function adequacy?
Indocyanine green (ICG) assessment indicates post-resection liver function adequacy.
What is the FLR threshold for normal liver function?
For normal liver, FLR should be 20% of the standardized liver volume (SLV).
What is the significance of ECOG performance scale?
ECOG scale assesses patient activity level from fully active (0) to disabled (higher).
The Child-Pugh Score is based on: - Albumin - Bilirubin - Coagulation - Distension - Encephalopathy
What are the levels of physical activity restriction for patients?
- 1: Restricted in physically strenuous activity, otherwise fully ambulatory
- 2: ADL independent, up and about > 50% of waking hours
- 3: ADL dependent, confined to bed/chair > 50% of waking hours
- 4: ADL dependent, totally confined to bed/chair
What investigations are considered for low Hb from BGIT?
- FBC: low Hb from BGIT
- U/E/Cr: dehydration, possible nephropathy
- Other tests: PT/PTT, LFT, GXM, ECG, CXR, CT TAP
What is the purpose of CT TAP imaging?
To suspect metastatic disease.
What procedures are done if hepatic lesions are suspected?
- OGD
- Colonoscopy
The Barcelona Clinic Liver Cancer management algorithm includes treatment options like: - resection - transplantation - ablation - chemoembolization - systemic therapies.
Which systemic drugs are first-line for liver cancer treatment?
Paracetamol
Ibuprofen
Lenvatinib
Aspirin
Sorafenib
What is included in the management algorithm regarding survival?
Immediate cure
Estimated survival time
Surgical complication risks
Patient's weight
What does the diagram for the Barcelona Clinic Liver Cancer management algorithm illustrate?
It details stages, liver function, performance status, tumor burden, treatment options, and estimated survival time.
What is the treatment of choice for non-cirrhotic patients with HCC?
Surgical resection, especially for solitary tumors at early stage (i.e. 0 or A).
What percentage of HCC patients are amenable to surgery?
Only about 10-20%.
What is the 5-year survival rate for patients treated with surgical resection?
60%, but with a high recurrence rate of 70%.
What is a major concern for patients undergoing hepatectomy?
High recurrence rates due to the 'field-change' effect in the liver.
What is the balance required in hepatectomy?
Between adequate resection margins (~1cm) and preservation of functional liver.
What monitoring is essential post-operation for liver assessment?
Vitals signs, urine output, biochemical markers (FBC, LFTs, INR).
What kind of drugs should be avoided post-operation?
Hepatotoxic drugs.
What is the definitive treatment for HCC that replaces the cirrhotic liver?
Liver transplantation.
What are the Milan criteria for liver transplantation?
- Single tumor <5cm
- Max 3 tumors with none >3cm
- No evidence of vascular invasion.
What is the UCSF criteria for liver transplantation?
- Single tumor <6.5cm
- Max 3 tumors with none >4.5cm & cumulative size <8cm.
What is bridging therapy in the context of liver transplantation?
Using RFA, TACE, Y-90 to shrink disease until a donor's liver is available.
The treatment modalities for HCC management include curative and palliative approaches, such as: - Curative: Surgical resection, liver transplantation. - Palliative: Local (radiofrequency ablation), regional (TACE), systemic (Sorafenib).
What is a contraindication for liver resection?
- Metastatic disease
- Multicentric disease affecting both lobes
What factors increase postoperative mortality in cirrhotic patients?
- Liver failure
- Bleeding
- Infection
What Child's status allows for resection in cirrhotic patients?
- Child's A
- Good Child's B
What ICG result indicates tolerance for major liver surgery?
< 10% remains after 15 minutes
What FLR requirement is needed for patients with normal liver?
<blockquote>
20% of pre-operative liver volume
</blockquote>
What is the appropriate management for tumors > 2.5cm in size?
- Multiple RFA deployments
What is a contraindication for Radiofrequency Ablation (RFA)?
- Tumor at hilar plate
- Biliary stricture/fistula risks
What is the best therapy for early-stage HCC not suitable for resection?
Radiofrequency ablation (RFA)
What are major complications of Trans-arterial Chemoembolization (TACE)?
- Portal vein thrombosis
- Decompensated cirrhosis
What is the typical method of entry for TACE?
Via the femoral artery
What can be performed to encourage hypertrophy of the liver?
Portal vein embolization
What indicates increased resistance to flow during liver resection?
Worsened portal hypertension
What condition can cause fever secondary to cytokine release?
Tumour lysis.
What are the symptoms associated with tumour lysis?
- Abdominal pain
- Nausea
- Vomiting
What do raised ALT and AST levels reflect?
Ischemic hepatitis due to hepatic failure.
Why should TACE not be used for Child's class C cirrhosis?
It can cause hepatic failure due to infarction.
What does Yttrium-90 do when injected into the hepatic artery?
It irradiates the tumor, inducing tumor necrosis.
What is Sorafenib and its effect on survival?
Multi-kinase inhibitor that improves median survival by 3 months.
What is the estimated 5-year survival rate for HCC with treatment?
18%.
What is the median survival length for untreated HCC?
3 to 6 months.
Trans-arterial embolization (TAE) is a technique used to treat tumors in the liver.
What is the outcome of combining TACE with systemic drugs like Sorafenib?
Does not improve survival
Increases tumor size
Significantly improves survival
Reduces side effects
What percentage of liver tumors are secondary malignancies?
90% of liver tumors are secondary malignancies.
Which cancer is the most common cause of secondary liver malignancy?
Colorectal cancer.
What are the types of liver metastases classified by origin?
Neuroendocrine and non-neuroendocrine liver metastases.
Colorectal liver metastases are detected in 20-25% of patients as synchronous lesions and up to 40% as metachronous lesions.
What signs indicate metastasis to liver parenchyma?
- Fullness in RUQ
- Hard, irregular hepatomegaly
- Constitutional symptoms (i.e. LOW, LOA)
- Jaundice as a late sign
What is a common complication from extensive liver metastasis?
Liver failure with ascites and coagulopathy.
What should be done for patients with metastatic disease to the liver?
They should be discussed at a multidisciplinary tumor board and referred to a medical oncologist.
For colorectal liver metastases, liver resection is recommended due to the tumour biology's favourable nature.
What is the overall frequency of recurrence for liver metastases after 5 years?
60-80% recurrence at 5 years.
What is a characteristic imaging finding for liver metastases on CT?
Hyperdense on arterial phase
Uniform density
Hypodense on arterial phase
Cystic appearance
What is a hepatic abscess?
A pus-filled area in the liver, usually in the right lobe, occurring secondary to bacterial sepsis.
What organisms can cause a hepatic abscess?
- Klebsiella
- E. coli
- Proteus vulgaris
- Streptococcus milleri/faecalis
- Staphylococcus epidermidis
- Bacteroides fragilis
What are the risk factors for hepatic abscess?
- Diabetes
- Immunocompromised status
- Underlying hepatobiliary disease
- Elderly age
What is the most common route of infection for hepatic abscess?
Biliary tree: direct spread from biliary infections (60%).
What are common clinical presentations of hepatic abscess?
- Spiking fever
- Abdominal pain
- Jaundice
- Hepatomegaly
- Nonspecific symptoms
What is the most definitive imaging technique for diagnosing hepatic abscess?
CT scanning is used to exclude liver tumors and confirm diagnosis.
What laboratory findings indicate a hepatic abscess?
- Leukocytosis
- Elevated CRP/ESR
- Deranged LFTs
- Blood/pus cultures (e.g. Klebsiella)
A hepatic abscess often arises due to infections in the biliary system, with a common cause being ascending cholangitis.
What should be done if resuscitation is needed?
Resuscitate if necessary.
What is crucial for monitoring patients?
Close monitoring of vitals with strict IO charting.
What complications should be watched for?
Klebsiella endophthalmitis, especially in diabetic patients.
What are the empirical antibiotics for pyogenic liver abscess?
- IV ceftriaxone 1gm every 12 hours
- Metronidazole 500mg every 8 hours
What is the total duration of antibiotic treatment?
4-6 weeks, counting from the drainage date.
When is drainage indicated?
If abscess > 3cm.
What is required for a colonoscopy in patients >50 years with DM and K pneumoniae PLA?
To rule out colonic malignant lesions.
What is a contraindication for percutaneous drainage?
Ascites.
What is the gold standard for treating liver abscesses?
Open drainage (OD).
What are the advantages of laparoscopic drainage?
- Shorter surgery duration
- Less blood loss
- Faster recovery
What is the definition of hepatic amoebic abscess?
Hepatic amoebic abscess is caused by liquefaction necrosis, filled with blood and liquefied liver tissue, resembling 'anchovy sauce'.
How much more frequent is hepatic amoebic abscess in adult men compared to women?
7-10 times more frequent.
What protozoan causes amoebiasis?
Entamoeba histolytica.
What is the transmission route of hepatic amoebic abscess?
Transmission is faecal-oral; humans are the principal host.
What is a common clinical presentation of hepatic amoebic abscess?
- Persistent fever
- Right upper quadrant pain
- Diarrhoea (in <1/3 of patients)
What is a diagnostic method for hepatic amoebic abscess?
Ultrasound or CTAP is used to confirm the presence of a liver abscess.
What is the first-line treatment for hepatic amoebic abscess?
Metronidazole (750mg oral TDS or IV 500mg QDS for 7-10 days).
What complications can arise from hepatic amoebic abscess?
- Rupture causing peritonitis
- Bacterial superinfection
- Free rupture into the peritoneal cavity
What is the mortality rate in complicated cases of hepatic amoebic abscess?
Mortality can be as high as 20%.
Flashcards in this deck (323)
-
-
-
-
-
-
-
What divides the liver into the right and left lobes?
The falciform ligament separates the liver into right and left lobes.
anatomy liver -
What is Cantlie's Line?
Cantlie's Line is a functional division of the liver, along the gallbladder fossa and inferior vena cava.
anatomy liver -
What surrounds the bare area of the liver?
The bare area is not covered by Glisson's capsule.
anatomy liver -
What segments form the left hemiliver?
- Segment II
- Segment III
- Segment IV
anatomy liver -
What are the four sections of the liver based on the hepatic artery?
- Right anterior section (segments V & VIII)
- Right posterior section (segments VI & VII)
- Left medial section (segment IV)
- Left lateral section (segments II & III)
anatomy liver -
The liver can be divided into 8 functional segments also known as Couinaud segments.
anatomy liver -
Which ligament is not part of the liver anatomy?
Bare Area
Right Triangular Ligament
Falciform Ligament
Coronary Ligament
anatomy liver -
What is the primary purpose of the caudate lobe?
The caudate lobe contains 3 sub-segments: spiegel lobe, paracaval, and caudate process.
anatomy liver -
What does the liver weigh approximately?
The liver weighs about 1.5 kg.
anatomy liver -
What ligament is a remnant of the obliterated umbilical vein?
The Round Ligament (ligamentum teres).
anatomy liver -
What ligaments attach the liver to the anterior abdominal wall?
- Falciform Ligament
- Coronary Ligament
- Left and Right Triangular Ligament
anatomy ligaments liver -
What supplies 75% of the liver's blood?
The portal vein.
physiology blood_supply liver -
What is the primary arterial blood supply to the liver?
The hepatic artery proper (25%).
physiology blood_supply liver -
What drains segment V, VI, VII, and VIII of the liver?
The Right hepatic vein.
anatomy venous_drainage liver -
What anatomical variant arises from the SMA?
Replaced right hepatic artery (10-15%).
anatomy variations vascular -
How do segment V & VIII drain into the liver?
Via the right anterior sectoral duct (RASD).
anatomy biliary_system -
The three main hepatic veins form sagittal planes and include the Right hepatic vein, Middle hepatic vein, and Left hepatic vein.
anatomy venous_drainage liver -
The portal vein divides into the right and left portal vein branches.
physiology blood_supply liver -
What is the significance of the caudate lobe's venous drainage?
It drains directly to the IVC.
anatomy venous_drainage liver -
What drains the segments VI and VII of the liver?
The right posterior sectoral duct (RPSD).
anatomy biliary_system -
What is a common anatomical variant involving the biliary system?
RPSD draining into LHD (15%).
anatomy variations biliary_system -
What stimulates the contraction of the gallbladder?
CCK (Cholecystokinin)
physiology gallbladder -
What are the two factors governing bile secretion?
- Enterohepatic circulation
- Gut hormones (CCK & secretin)
physiology bile -
What is the consequence of a lack of bile?
Malabsorption of fats and fat-soluble vitamins (A, D, E, K)
physiology bile -
Bile is diverted from the liver into the gallbladder due to high tone in the sphincter of Oddi.
physiology gallbladder -
What is the role of the liver in carbohydrate metabolism?
- Glycogenesis
- Glycogenolysis
metabolism carbohydrates -
What process occurs to amino acids during starvation?
Gluconeogenesis - conversion back to glucose
metabolism proteins -
What is lipogenesis?
Conversion of glucose to glycerol + FFA forming TG (triglycerides)
metabolism lipids -
What is the Cori Cycle?
Lactate is converted to glucose in the liver and returned to the muscle.
physiology metabolism -
What vitamin is activated in a two-stage hydroxylation process?
Vitamin D
physiology vitamins -
What is synthesized in the liver besides immunoglobulin?
Plasma proteins such as albumin and clotting factors.
physiology proteins -
What regulates iron homeostasis?
The synthesis of Hepcidin in the liver.
physiology iron -
Which cells in the liver are responsible for phagocytosis?
Kupffer cells.
physiology immunity -
What is the role of the liver in detoxification?
Detoxify peptide hormones, drugs, and toxins.
physiology detoxification -
What forms the main storage for fat-soluble vitamins?
- Vitamin A
- Vitamin D
- Vitamin E
- Vitamin K
- Vitamin B12
physiology storage -
What substance is converted by the liver in the Cori Cycle?
Fatty acids
Lactate
Amino acids
Glucose
physiology cori_cycle -
What is the definition of portal hypertension?
Portal Hypertension is defined as the Hepatic venous pressure gradient (HVPG) ≥ 6mmHg. Normal is 3-5mmHg.
medicine portal_hypertension -
What is the normal portal flow rate?
1-1.5 L/min is the normal portal flow rate.
medicine flow_rate -
What indicates high risk of developing gastroesophageal varices?
Portal HTN ≥ 10mmHg indicates high risk of gastroesophageal varices.
medicine risk -
What pressure level poses a high risk for variceal bleed?
Portal HTN ≥ 12mmHg indicates high risk of variceal bleed.
medicine risk -
Which organs are drained by portal veins?
- Small intestines
- Large intestines
- Stomach
- Spleen
- Pancreas
- Gallbladder
anatomy portal_veins -
What forms the portal vein?
The SMV and the splenic vein unite behind the neck of the pancreas to form the portal vein.
anatomy portal_veins -
The portal trunk divides into two lobar veins: the right branch that drains the cystic vein and the left branch which drains the umbilical and paraumbilical vein (caput medusae in portal HTN).
anatomy portal_hypertension -
What is a consequence of portal hypertension due to cirrhosis?
Portal hypertension results from mechanical obstruction of the portal venous system.
pathophysiology cirrhosis -
What are the key issues with cirrhosis affecting portal hypertension?
- Architecture distortion
- Regenerative parenchymal nodules
- Disruption of liver architecture
pathophysiology cirrhosis -
According to Ohm's Law, the relationship between voltage (V), current (I), and resistance (R) is given by: V = IR. Poiseuille's Law states that R = 8hL/pr^4.
physics vascular_flow -
What impact does decreasing portal vascular radius have on resistance?
Dramatic increase in portal vascular resistance occurs with decreased vascular radius.
pathophysiology resistance -
The diagram illustrating portal hypertension pathophysiology and collateral circulation shows key elements such as splanchnic vasodilation and TIPS (Transjugular Intrahepatic Portosystemic Shunt).
pathophysiology portal_hypertension -
Illustration of the liver and its venous drainage highlights esophageal, paraumbilical, and rectal varices.
anatomy varices -
What is a major cause of pre-sinusoidal portal hypertension?
- Portal Vein Thrombosis
- Splenic Vein Thrombosis
- Congenital Atresia
portal hypertension pre-sinusoidal -
What is a common cause of sinusoidal portal hypertension?
- Cirrhosis
- Massive Fatty Change
- Hemochromatosis
portal hypertension sinusoidal -
What are some causes of post-sinusoidal portal hypertension?
- Hepatic vein thrombosis
- IVC thrombosis
- Congenital IVC malformation
portal hypertension post-sinusoidal -
What condition is associated with Budd Chiari Syndrome?
Rare thromboembolic disorder of hepatic veins/IVC leading to post-sinusoidal portal hypertension.
budd_chiari portal_hypertension -
What are key ultrasound findings for portal hypertension?
- Dilated splenic & superior mesenteric veins ≥ 11mm
- Splenomegaly > 12cm
- Dilated portal vein ≥ 13mm
ultrasound portal_hypertension investigations -
In portal hypertension, ascites occurs due to: increased fluid shift leading to increased lymphatic drainage from liver which overwhelms thoracic duct capacity, resulting in percolation of hepatic lymph into the peritoneal cavity.
portal_hypertension ascites -
What is a significant complication of portal hypertension?
- Ascites
- Hepatic Encephalopathy
- Portal Hypertensive Gastropathy
complications portal_hypertension -
What causes spontaneous bacterial peritonitis (SBP) in ascites?
Chronic alcoholism
Dilated portal vein
Hemochromatosis
Increased fluid shift (Starling's law)
ascites sbp -
What are some symptoms of Hepatic Encephalopathy?
- Hyperammonemia
- Neuro-toxicity
- Exacerbated by portosystemic shunting
hepatic_encephalopathy portal_hypertension -
Which anatomical area is affected by oesophageal varices?
Portal circulation through oesophageal branch of left gastric vein.
oesophageal_varices portal_circulation -
What is Caput Medusae related to?
Varicosity caused by systemic circulation through superficial epigastric veins.
caput_medusae portal_hypertension -
What does progressive liver cirrhosis lead to?
Obstruction of intra-hepatic vasculature causing portal hypertension.
pathophysiology cirrhosis -
What is released due to portal HTN in cirrhotic patients?
Increased splanchnic nitric oxide (NO).
pathophysiology cirrhosis -
What stimulates RAAS in cirrhotic patients?
Renal hypoperfusion.
pathophysiology cirrhosis -
What is the effect of aldosterone in ascites treatment?
Increases retention of salt and water.
treatment ascites -
What is the diuretic of choice for cirrhotic patients with ascites?
Spironolactone (aldosterone antagonist).
treatment ascites -
What are common symptoms of ascites?
- Progressive abdominal distension
- Weight gain
- Shortness of breath
- Early satiety
clinical ascites -
What physical signs confirm the diagnosis of ascites?
- Abdominal distension
- Flank dullness
- Shifting dullness
- Umbilical eversion
physical_exam ascites -
What does the SAAG ≥ 1.1g/dL indicate?
Porta hypertension; common cause is liver cirrhosis.
diagnosis ascites -
What can a SAAG <1.1g/dL indicate?
Malignancy or infection such as peritoneal tuberculosis.
diagnosis ascites -
What investigations are performed for suspected ascites?
- Biochemical tests (FBC, U/E/Cr, LFT)
- Imaging (Ultrasound/CT)
investigations ascites -
What does a peritoneal tap assess?
Fluid color and appearance to distinguish between conditions.
diagnosis ascites -
What is the common indication for a peritoneal tap in ascites?
Diagnostic
Curative
Preventive
Therapeutic
investigations ascites -
What is a common microbiological test for ascitic fluid?
Gram stain smear, culture (aerobic / anaerobic), cytology
microbiology ascites -
What are the laboratory tests included in the analysis of ascitic fluid?
- LDH
- TG
- Glucose
- TB culture
- ProBNP
laboratory ascites -
What is the recommended low salt diet for ascites?
2000mg / day or 88mol/day
diet ascites -
When should fluid restriction be considered?
If serum sodium <125mmol/L
fluid_restriction ascites -
What is the typical pharmacological treatment for diuresis in ascites?
- Spironolactone 100mg
- Furosemide 40mg (Max 400mg:160mg)
pharmacology ascites -
What is the recommended antibiotic for suspected spontaneous bacterial peritonitis?
IV ceftriaxone or oral quinolones (e.g., ciprofloxacin)
antibiotics sbp -
What is the purpose of therapeutic paracentesis?
To manage tense ascites and prevent complications.
procedure ascites -
What is the procedure for therapeutic paracentesis?
- Site: 2FB above and 2FB lateral to ASIS
- Use aseptic technique, LA, US-guided
procedure paracentesis -
Why is albumin administered after paracentesis?
To prevent paracentesis-induced circulatory dysfunction.
albumin ascites -
What surgical options are available for liver disease-related ascites?
- Liver transplantation
- Transjugular Intrahepatic Porto-Systemic Shunts (TIPSS)
- Peritoneovenous shunts
surgery ascites liver_disease -
What should be controlled pre-operatively in cirrhotic patients?
Ascites
surgery cirrhosis -
What is the risk of abdominal operations in patients with advanced cirrhosis?
High risk of complications, especially portal hypertension.
surgery cirrhosis risks -
What is performed prior to major abdominal operations in high MELD score patients?
Transjugular Intrahepatic Portosystemic Shunt (TIPSS).
surgery cirrhosis meld -
What does hepatomegaly refer to?
Hepatomegaly refers to the abnormal enlargement of the liver.
medical definitions -
What are common symptoms of hepatomegaly?
- Asymptomatic
- Abdominal pain
- Nausea, vomiting
- Fever
- Signs of jaundice
medical symptoms -
What should a clinical examination for hepatomegaly include?
- Palpable organomegaly
- Tenderness
- Signs of ascites
- Digital Rectal Examination
medical examination -
Common presentations of hepatomegaly include: abdominal pain, nausea, vomiting, and fever.
medical presentation -
What are signs of chronic liver disease?
- Gynaecomastia
- Clubbing of fingernails
- Palmar erythema
- Lower limb edema
medical liver_disease -
What is a common risk factor for malignant lesions in hepatomegaly?
Ongoing weight loss
Sudden fever
History of liver cirrhosis
High blood pressure
medical diagnosis -
Symptoms of portal hypertension may include splenomegaly and ascites.
medical portal_hypertension -
What is a physiological cause of liver abnormalities?
Riedel's Lobe Hyperextended Chest
physiology liver -
Name a bacterial infection that can affect the liver.
Pyogenic Liver Abscess Tuberculosis
infective liver -
Which viral infections are known to affect the liver?
Hepatitis EBV CMV HIV
infective viral liver -
What are some alcohol-related liver conditions?
Fatty Liver Cirrhosis
alcoholic liver -
Which metabolic diseases can affect the liver?
Wilson's Disease Haemochromatosis Infiltration - amyloidosis
metabolic liver -
What are some malignant liver conditions?
Hepatocellular Carcinoma Hepatic Angiosarcoma Cholangiocarcinoma
malignant liver -
What is a vascular/cardiac disorder that affects the liver?
Right Heart Failure (RHF) Budd-Chiari Syndrome
vascular _cardiac liver -
A benign hepatic neoplasm can be a Haemangioma, Hepatic Adenoma, or Focal nodular Hyperplasia.
benign neoplasm liver -
What types of hepatic abscesses exist?
Pyogenic Abscess Amoebic Abscess
abscess liver -
What are the two types of hepatic cysts?
Non Parasitic Cyst Echinococcal Cysts
cysts liver -
Intrahepatic obstruction causes of portal hypertension include Cirrhosis and Wilson's Disease.
portal_hypertension liver -
What is a post-hepatic obstruction condition for portal hypertension?
Budd-Chiari Syndrome IVC Thrombosis
portal_hypertension liver -
Factors associated with Hepatic Angiosarcoma include exposure to vinyl chloride, arsenic.
malignant liver -
What is a Full Blood Count used for?
To detect any anemia or signs of infections.
laboratory hematology -
What does a Liver Function Test indicate?
Presence of hyperbilirubinemia and deranged liver enzymes.
laboratory liver -
What are Tumour Markers used for?
Their presence can indicate suspicion of malignancy.
oncology diagnostics -
What imaging techniques are used for liver examination?
- Ultrasound Liver
- CT Scan
- MRI
imaging liver -
An Ultrasound of the liver can reveal a simple cyst as: - well defined smooth walls - posterior acoustic enhancement.
imaging liver -
A CT Scan of a haemangioma shows: - early peripheral nodular enhancement - centripetal filling.
imaging haemangioma -
The MRI of a Hepatic Adenoma reveals: - hypervascular enhancement on arterial phase - lack of central scar.
imaging adenoma -
In Focal Nodular Hyperplasia (FNH), the Doppler appearance shows: - central feeding artery - tortuous spoke-wheel vascularity.
imaging fnh -
For Hepatocellular Carcinoma (HCC), imaging might show: - hypervascular enhancement on arterial phase - portal venous washout.
imaging hcc -
Which imaging technique is NOT typically used for liver examination?
CT Scan
MRI
Endoscopy
Ultrasound Liver
imaging liver -
What are liver hemangiomas characterized by?
Benign vascular lesions consisting of widened (dilated) blood vessels, not true neoplasms.
pathology liver hemangioma -
What is the female to male ratio for liver hemangiomas?
5-6:1, predominantly in middle-aged women.
epidemiology liver hemangioma -
What is the usual presentation of a liver hemangioma?
Usually asymptomatic; may cause nonspecific abdominal pain when larger than 5cm.
presentation liver hemangioma -
What imaging technique is most accurate for liver hemangiomas?
Ultrasound, with 70-80% accuracy and pathognomonic compressibility of the lesion.
diagnosis liver hemangioma -
What does a CT scan of a hemangioma show?
Peripheral enhancement in the arterial phase and peripheral to central enhancement over time.
diagnosis liver hemangioma -
The majority of liver hemangiomas are treated with observation if they are asymptomatic and smaller than 4cm.
treatment liver hemangioma -
What should never be done for diagnosing liver hemangiomas?
Biopsy, due to risk of severe and fatal hemorrhage.
diagnosis liver hemangioma -
What syndrome is associated with large hemangiomas?
Kasabach-Merritt syndrome, which leads to thrombocytopenia and consumptive coagulopathy.
complications hemangioma -
What is a common treatment for symptomatic or complicated liver hemangiomas?
Radiation therapy
Surgical removal
Observation
Chemotherapy
treatment liver hemangioma -
What are the symptoms of large liver hemangiomas?
- Nonspecific abdominal fullness
- Abdominal pain
- Rarely, life-threatening hemorrhage
presentation liver hemangioma -
What is the definition of Focal Nodular Hyperplasia (FNH)?
FNH is a benign tumour characterized by a central stellate scar and is considered a regenerative process, not a result of arterial malformation.
medical definitions -
What is the epidemiology of FNH?
- Second commonest benign liver tumour
- More common in females (6-8:1) aged 30 to 50 years
- Associated with AVMs and hepatic haemangioma.
medical epidemiology -
What symptoms are associated with FNH?
- Asymptomatic (incidental on imaging)
- Right upper quadrant pain
- Rarely ruptures or bleeds.
medical symptoms -
How is FNH diagnosed?
- CT: Bright homogenous enhancement, hypoattenuating central scar.
- Sulphur colloid scan: Positive for kupffer cells.
- MRI: Central scar hyperintense on T2 weighted images.
medical diagnosis -
What is the treatment for FNH?
- Conservative management for asymptomatic patients.
- Surgery for symptomatic patients, with liver resection preferred.
medical treatment -
FNH is a benign tumour characterized by a central stellate scar and is considered a regenerative process.
medical definitions -
FNH is the second commonest benign liver tumour, more common in females aged 30 to 50 years.
medical epidemiology -
Symptoms of FNH include: - asymptomatic - right upper quadrant pain.
medical symptoms -
Diagnosis of FNH involves: - CT with bright enhancement and hypoattenuating scar - sulphur colloid scan - MRI.
medical diagnosis -
FNH treatment options are: - conservative management for asymptomatic patients - surgery for symptomatic patients.
medical treatment -
What are hepatic adenomas?
Benign proliferation of hepatocytes; should not be confused with hepatoma (HCC).
health pathology -
What is the female to male ratio for hepatic adenomas?
10:1, primarily found in young women.
epidemiology gender -
What are common presentations of hepatic adenomas?
Asymptomatic or symptomatic with spontaneous rupture and intraperitoneal hemorrhage.
presentation symptoms -
What percentage of hepatic adenomas may rupture?
25-35%, with nearly 100% of ruptures in lesions >5cm.
risk rupture -
What are common diagnosis methods for hepatic adenomas?
CT (triphasic), sulphur colloid scan, and MRI.
diagnosis imaging -
What is the treatment for small, asymptomatic hepatic adenomas?
Conservative management with close observation and possible discontinuation of OCPs.
treatment management -
What is indicated for symptomatic hepatic adenomas or those >4-5cm?
Surgical resection.
treatment surgery -
Hepatic adenomas are characterized by a benign proliferation of hepatocytes, distinct from hepatoma which refers to HCC.
definition health -
The risk factors for hepatic adenomas include anabolic steroids, oestrogen, and progesterone preparation (e.g., OCP).
risk_factors health -
A significant risk of hepatic adenomas is malignant transformation to well-differentiated HCC, with a risk of ~5%.
risk malignancy -
What characteristic is NOT associated with imaging findings in hepatic adenomas?
No true lobules
Sharply defined borders
More common in right lobe
Homogenous enhancement during arterial phase
diagnosis health -
What should be done if a patient has an acute hemorrhage from hepatic adenoma?
Discontinue all medications
Proceed to hepatic angioembolization followed by surgery
Immediate liver transplant
Complete bed rest without intervention
treatment emergency -
What are liver cysts commonly detected through?
Imaging, as they are mostly asymptomatic.
medicine liver -
What percentage of liver cysts are simple ones?
5-20%
medicine liver -
Nonparasitic liver cysts include: - Simple Liver Cysts - Polycystic Liver Disease - Neoplastic Cysts - Echinococcal Cysts.
medicine liver -
What symptoms may occur due to symptomatic liver cysts?
- RUQ tenderness - Palpable Hepatomegaly - Bleeding, Infection, Torsion, Rupture
medicine liver -
What are common complications of a simple liver cyst?
- Infection - Intracystic hemorrhage - Pain
medicine liver -
What is a common extrahepatic manifestation of Polycystic Liver Disease?
Kidney Stones
Heart Disease
Lung Cancer
Cerebral Aneurysm
medicine liver -
What management is used for symptomatic simple liver cysts?
- Percutaneous aspiration with sclerotherapy - Laparoscopic 'unroofing'
medicine liver -
Neoplastic cysts can include: - Cystadenoma - Cystadenocarcinoma - IPMN-B.
medicine liver -
What is a potential treatment for suspected cystadenoma?
Formal resection or enucleation.
medicine liver -
What can blunt trauma lead to regarding liver cysts?
Intra-hepatic hematomas or bilomas developing into traumatic hepatic cysts.
medicine liver -
What should be done for suspected cystic malignancies?
Proceed with biopsy or formal hepatic resection.
medicine liver -
What is the primary cause of Cystic Echinococcosis?
Infestation with tapeworm of the genus Echinococcus, primarily E. granulosus.
parasitology cysticechinococcosis -
What is a definitive host for Echinococcus?
Dogs serve as the definitive hosts for Echinococcus.
parasitology hosts -
What can humans be classified as regarding Echinococcus?
Humans are considered dead-end hosts for Echinococcus.
parasitology hosts -
What are common organs affected by hydatid cysts?
- Liver
- Lung
- Bone
- Kidney
- Spleen
- CNS
parasitology organs -
What is the first-line imaging technique for diagnosing hydatid cysts?
Ultrasound is the first-line imaging technique for diagnosing hydatid cysts.
diagnosis imaging -
What serological tests can aid in the diagnosis of Echinococcosis?
- Immunoelectrophoresis
- ELISA
diagnosis serology -
What is the percutaneous treatment technique for hydatid cysts?
The PAIR technique (Puncture, Aspiration, Injection, Re-aspiration) is used.
treatment pair -
What risks are associated with the PAIR technique for treating hydatid cysts?
- Anaphylactic shock
- Secondary echinococcosis
- Chemical cholangitis
- Biliary fistula
treatment risks -
What surgical options are available for treating hydatid cysts?
- Radical: pericystectomy
- Conservative: unroofing of cyst
treatment surgery -
What medications are used to treat Echinococcosis?
Albendazole +/- praziquantel are used for treatment.
treatment medications -
What is the treatment approach for inactive silent cysts?
The approach is typically to watch and wait.
treatment inactive -
What is Alveolar Echinococcosis primarily treated with?
Radical Liver Resection or Liver Transplantation.
treatment alveolarechinococcosis -
What is the annual incidence of hepatocellular carcinoma (HCC) in Singapore for males?
18 / 100,000
epidemiology hcc -
What is the annual incidence of hepatocellular carcinoma (HCC) in Singapore for females?
4.6 / 100,000
epidemiology hcc -
HCC is the 4th most frequent cancer death among which gender?
Females
epidemiology hcc -
Hepatocellular carcinoma is primarily diagnosed in what decades of life?
Fifth and sixth decades
epidemiology hcc -
What percentage of liver cancers are HCCs?
85%
epidemiology hcc -
What is the most common risk factor for developing HCC?
Chronic liver disease (CLD)
risk_factors hcc -
What virus infection is associated with increased HCC risk due to DNA damage?
Hepatitis B Virus (HBV)
risk_factors hbv hcc -
The risk of HCC approaches 2-4% annually in patients with which condition?
Cirrhosis
risk_factors hcc -
Alcoholic cirrhosis increases the risk of HCC by how many times?
5 times
risk_factors hcc -
Chronic Hepatitis C accounts for what fraction of HCC cases in the USA?
1/3
risk_factors hcc -
Non-alcoholic steatohepatitis (NASH) increases the risk of HCC by 20x.
risk_factors hcc -
Diet high in red meat and saturated fats is linked to what cancer?
Hepatocellular carcinoma (HCC)
risk_factors diet hcc -
What toxin found in moldy food is linked to HCC?
Aflatoxins B1
risk_factors toxins hcc -
Chronic HBV along with which lifestyle factor has a synergistic effect on HCC risk?
Alcohol consumption
risk_factors hcc -
What condition is characterized by inflammation of the biliary tree often leading to HCC?
Primary Sclerosing Cholangitis
risk_factors hcc -
Recurrent infection in the biliary tree due to pyogenic cholangitis can lead to which cancer?
Hepatocellular carcinoma (HCC)
risk_factors hcc -
What is the process of pathogenesis associated with?
- Chronic inflammatory process
- Ongoing hepatocellular damage
- High cellular regeneration leading to genetic mutation accumulation
pathology pathogenesis -
What classification represents worse clinical outcomes?
- Proliferative Class
- Associated with HBV infection
- High AFP levels
- High tumor grade
pathology classification -
What factors characterize the Non-proliferative Class?
- Non-proliferative Class
- HCV infection
- Alcohol abuse
- Low tumor grade
- Better clinical outcomes
pathology classification -
What are the histological subtypes of liver cancer?
- Non-Fibrolamellar
- Fibrolamellar (FLC) - more common in younger patients, no Hep B association
pathology histology -
What are the main characteristics of liver cirrhosis?
- Bridging fibrosis
- Regenerative parenchymal nodules
- Disruption of liver architecture
pathology cirrhosis -
How often should patients with cirrhosis undergo monitoring?
- Every 6 months
- Ultrasound of the liver
- Serum AFP measurement
pathology monitoring -
What is the MELD score used for?
- Predicting prognosis in cirrhosis patients
- Assessing mortality risk after TIPSS
- Prioritizing liver transplantation
pathology meld -
What factors are included in the MELD score calculation?
- Serum bilirubin
- INR
- Serum creatinine
- Constant for liver disease etiology
pathology meld -
What does a MELD score of 15 indicate?
- 6% mortality risk at 3 months
pathology meld -
What outcomes are best with a MELD score less than 14?
- Best outcomes with TIPSS
- Poor outcomes with scores >24
pathology meld -
What does an increase in MELD points indicate?
- Post-op mortality risk increases by 1% for each point up to 20
- Increases by 2% for each point above 20
pathology meld -
What criteria are included in the PELD score?
- Age
- Presence of growth failure
- Albumin instead of creatinine
pathology peld -
What is the typical presentation of patients with HCC during screening?
Patients are often asymptomatic. HCC can be an incidental finding during ultrasound screening for chronic hepatitis B.
hcc screening -
What are common local signs & symptoms of HCC?
- Upper abdominal pain (dull & persistent)
- Early satiety/vomiting
- Constitutional symptoms: low energy, loss of appetite, malaise
- Pyrexia
- Jaundice (5-10%)
hcc symptoms -
Patients with HCC may experience upper abdominal pain, early satiety/vomiting, and constitutional symptoms such as low energy, loss of appetite.
hcc symptoms -
What is Budd-Chiari syndrome?
It is the occlusion of hepatic, intrahepatic, or portal veins causing portal hypertension and congestive hepatopathy, often leading to ascites.
hcc budd-chiari -
What are the features of decompensated chronic liver disease?
- Worsening liver function
- Hepatic encephalopathy
- Jaundice
- Ascites
- Spontaneous bacterial peritonitis
liver decompensation -
What is a possible severe complication of a liver tumor?
Hepatic fibrosis
Cirrhosis
Hepatocellular carcinoma
Tumour rupture
hcc complications -
What symptoms are associated with portal hypertension?
- Ascites
- Lower limb oedema
- Haematemesis
- Congestive splenomegaly
portal_hypertension symptoms -
Portal hypertension can present with symptoms such as ascites, lower limb oedema, and haematemesis.
portal_hypertension symptoms -
What are paraneoplastic syndromes associated with HCC?
- Hypoglycemia
- Erythrocytosis
- Hypercalcemia
hcc paraneoplastic -
Common paraneoplastic syndromes include hypoglycemia due to high metabolic demands and erythrocytosis from tumour-produced erythropoietin.
hcc paraneoplastic -
What is Hepatorenal Syndrome (HRS)?
A reversible form of acute renal failure in a patient with advanced liver disease without identifiable renal pathology.
medical renal -
What are the two types of Hepatorenal Syndrome?
- Type 1: Rapid renal function impairment, doubling serum creatinine > 221 in < 2 weeks.
- Type 2: Subtle course, serum creatinine < 221, develops diuretic-resistant ascites.
medical renal -
What leads to the renal hypoperfusion in HRS?
- Advanced cirrhosis leads to portal hypertension & splanchnic arterial vasodilation
- Decreased vascular resistance causes effective arterial hypovolemia.
medical pathophysiology -
What is the initial therapy for Hepatorenal Syndrome?
- Octreotide
- Midodrine
- Vasopressin analogue.
- Can progress to dialysis dependence.
medical treatment -
What can reverse Hepatorenal Syndrome?
Liver transplant, even after dialysis dependence.
medical treatment -
What are common causes of Hepatic Encephalopathy?
- High nitrogenous waste (BGIT)
- Infections (e.g., sepsis)
- Medications (e.g., benzodiazepines)
- Electrolyte imbalances.
- High protein diet.
medical causes -
What is Stage 0 of Hepatic Encephalopathy?
Lack of detectable changes in personality or behavior.
medical stages -
What characterizes Stage 1 of Hepatic Encephalopathy?
- Shortened attention span
- Impaired math skills
- Hypersomnia or insomnia
- Asterixis can be detected.
medical stages -
What are the symptoms of Stage 3 Hepatic Encephalopathy?
Gross disorientation, semi-stupor to stupor, bizarre behaviors.
medical stages -
What is the treatment for Hepatic Encephalopathy?
- Lactulose
- Low protein diet (<70g/day)
- Branched-chain amino acids.
- Neomycin for ammonia-producing bacteria if required.
medical treatment -
What is the gold standard diagnostic approach for hepatocellular carcinoma?
A triphasic CT scan with arterial and portal venous phase contrast imaging.
diagnosis hcc -
What does the arterial phase of a triphasic CT scan show?
Early enhancement with lesions appearing hyper-dense relative to hypo-dense hepatic parenchyma.
diagnosis ct_scan -
What indicates tumor washout in a triphasic CT scan?
Hypo-density of a nodule in the delayed phase compared to surrounding hepatic parenchyma.
diagnosis hcc -
The radiological hallmark of HCC includes: arterial hypervascularity and venous/late phase washout.
diagnosis hcc -
What does HCC's tendency to invade the portal vein indicate?
An enhancing portal vein thrombus.
diagnosis hcc -
What is the role of a lipiodol contrast CT scan?
To detect areas of tumor that may not be clear in pre-lipiodol CT, as lipiodol is retained in HCC.
diagnosis lipiodol -
What is the significance of detecting Alpha-FetoProtein (AFP) levels?
A rise in serum AFP in a cirrhosis patient suggests the development of HCC.
diagnosis afp -
What imaging modality is most accurate for distinguishing HCC from dysplastic nodules?
MRI scan (dynamic, contrast-enhanced).
diagnosis mri -
What are the complications to assess during HCC diagnosis?
Tumor burden, liver function, and patient's performance status.
assessment hcc -
What does the MRI appearance of HCC typically show?
Highly intense on T2 images and low-intensity on T1-weighted images.
diagnosis mri -
What is the role of ultrasound in liver cirrhosis?
Ultrasonography is often used for screening in the setting of liver cirrhosis.
ultrasound liver cirrhosis -
What is detected using contrast-enhanced ultrasound in HCC?
It is used for detecting arterial enhancement in HCC.
hcc ultrasound diagnosis -
What may biopsies risk during HCC assessment?
Biopsies have a risk of bleeding and needle tract seeding.
biopsy hcc risks -
What does the Child-Pugh Score assess?
It assesses liver function using LFTs + PT/INR/APTT.
child-pugh liver assessment -
What is the maximum surgical mortality for Class B in Child-Pugh Score?
The surgical mortality for Class B is 20-30%.
child-pugh surgical_mortality -
What does a Class C rating in Child-Pugh Score signify?
Class C indicates not for resection and a surgical mortality of 75-80%.
child-pugh surgical_risk -
What indicates post-resection liver function adequacy?
Indocyanine green (ICG) assessment indicates post-resection liver function adequacy.
icg liver_function -
What is the FLR threshold for normal liver function?
For normal liver, FLR should be 20% of the standardized liver volume (SLV).
flr liver function -
What is the significance of ECOG performance scale?
ECOG scale assesses patient activity level from fully active (0) to disabled (higher).
ecog performance assessment -
The Child-Pugh Score is based on: - Albumin - Bilirubin - Coagulation - Distension - Encephalopathy
child-pugh assessment liver -
What are the levels of physical activity restriction for patients?
- 1: Restricted in physically strenuous activity, otherwise fully ambulatory
- 2: ADL independent, up and about > 50% of waking hours
- 3: ADL dependent, confined to bed/chair > 50% of waking hours
- 4: ADL dependent, totally confined to bed/chair
health activity mobility -
What investigations are considered for low Hb from BGIT?
- FBC: low Hb from BGIT
- U/E/Cr: dehydration, possible nephropathy
- Other tests: PT/PTT, LFT, GXM, ECG, CXR, CT TAP
health investigations diagnostics -
What is the purpose of CT TAP imaging?
To suspect metastatic disease.
health imaging oncology -
What procedures are done if hepatic lesions are suspected?
- OGD
- Colonoscopy
health procedures diagnostics -
The Barcelona Clinic Liver Cancer management algorithm includes treatment options like: - resection - transplantation - ablation - chemoembolization - systemic therapies.
health management oncology -
Which systemic drugs are first-line for liver cancer treatment?
Paracetamol
Ibuprofen
Lenvatinib
Aspirin
Sorafenib
health medication oncology -
What is included in the management algorithm regarding survival?
Immediate cure
Estimated survival time
Surgical complication risks
Patient's weight
health management survival -
What does the diagram for the Barcelona Clinic Liver Cancer management algorithm illustrate?
It details stages, liver function, performance status, tumor burden, treatment options, and estimated survival time.
health diagram oncology -
What is the treatment of choice for non-cirrhotic patients with HCC?
Surgical resection, especially for solitary tumors at early stage (i.e. 0 or A).
hcc treatment surgery -
What percentage of HCC patients are amenable to surgery?
Only about 10-20%.
hcc statistics -
What is the 5-year survival rate for patients treated with surgical resection?
60%, but with a high recurrence rate of 70%.
hcc survival surgery -
What is a major concern for patients undergoing hepatectomy?
High recurrence rates due to the 'field-change' effect in the liver.
hcc surgery recurrence -
What is the balance required in hepatectomy?
Between adequate resection margins (~1cm) and preservation of functional liver.
hcc surgery hepatectomy -
What monitoring is essential post-operation for liver assessment?
Vitals signs, urine output, biochemical markers (FBC, LFTs, INR).
hcc post-op monitoring -
What kind of drugs should be avoided post-operation?
Hepatotoxic drugs.
hcc medications surgery -
What is the definitive treatment for HCC that replaces the cirrhotic liver?
Liver transplantation.
hcc treatment transplant -
What are the Milan criteria for liver transplantation?
- Single tumor <5cm
- Max 3 tumors with none >3cm
- No evidence of vascular invasion.
hcc transplant milan_criteria -
What is the UCSF criteria for liver transplantation?
- Single tumor <6.5cm
- Max 3 tumors with none >4.5cm & cumulative size <8cm.
hcc transplant ucsf_criteria -
What is bridging therapy in the context of liver transplantation?
Using RFA, TACE, Y-90 to shrink disease until a donor's liver is available.
hcc transplant bridging_therapy -
The treatment modalities for HCC management include curative and palliative approaches, such as: - Curative: Surgical resection, liver transplantation. - Palliative: Local (radiofrequency ablation), regional (TACE), systemic (Sorafenib).
hcc treatment modalities -
What is a contraindication for liver resection?
- Metastatic disease
- Multicentric disease affecting both lobes
surgery oncology -
What factors increase postoperative mortality in cirrhotic patients?
- Liver failure
- Bleeding
- Infection
surgery risk -
What Child's status allows for resection in cirrhotic patients?
- Child's A
- Good Child's B
surgery cirrhosis -
What ICG result indicates tolerance for major liver surgery?
< 10% remains after 15 minutes
surgery icg -
What FLR requirement is needed for patients with normal liver?
<blockquote>
20% of pre-operative liver volume
</blockquote>
surgery flr -
What is the appropriate management for tumors > 2.5cm in size?
- Multiple RFA deployments
treatment tumors -
What is a contraindication for Radiofrequency Ablation (RFA)?
- Tumor at hilar plate
- Biliary stricture/fistula risks
treatment rfa -
What is the best therapy for early-stage HCC not suitable for resection?
Radiofrequency ablation (RFA)
treatment hcc -
What are major complications of Trans-arterial Chemoembolization (TACE)?
- Portal vein thrombosis
- Decompensated cirrhosis
treatment tace -
What is the typical method of entry for TACE?
Via the femoral artery
treatment tace -
What can be performed to encourage hypertrophy of the liver?
Portal vein embolization
surgery portal_vein -
What indicates increased resistance to flow during liver resection?
Worsened portal hypertension
surgery physiology -
What condition can cause fever secondary to cytokine release?
Tumour lysis.
oncology fever -
What are the symptoms associated with tumour lysis?
- Abdominal pain
- Nausea
- Vomiting
symptoms oncology -
What do raised ALT and AST levels reflect?
Ischemic hepatitis due to hepatic failure.
liver biochemistry -
Why should TACE not be used for Child's class C cirrhosis?
It can cause hepatic failure due to infarction.
cirrhosis treatment -
What does Yttrium-90 do when injected into the hepatic artery?
It irradiates the tumor, inducing tumor necrosis.
treatment radiation -
What is Sorafenib and its effect on survival?
Multi-kinase inhibitor that improves median survival by 3 months.
medication oncology -
What is the estimated 5-year survival rate for HCC with treatment?
18%.
prognosis hcc -
What is the median survival length for untreated HCC?
3 to 6 months.
prognosis hcc -
Trans-arterial embolization (TAE) is a technique used to treat tumors in the liver.
treatment tae -
What is the outcome of combining TACE with systemic drugs like Sorafenib?
Does not improve survival
Increases tumor size
Significantly improves survival
Reduces side effects
treatment oncology -
What percentage of liver tumors are secondary malignancies?
90% of liver tumors are secondary malignancies.
liver malignancy statistics -
Which cancer is the most common cause of secondary liver malignancy?
Colorectal cancer.
cancer colorectal malignancy -
What are the types of liver metastases classified by origin?
Neuroendocrine and non-neuroendocrine liver metastases.
liver metastases classification -
Colorectal liver metastases are detected in 20-25% of patients as synchronous lesions and up to 40% as metachronous lesions.
liver colorectal statistics -
What signs indicate metastasis to liver parenchyma?
- Fullness in RUQ
- Hard, irregular hepatomegaly
- Constitutional symptoms (i.e. LOW, LOA)
- Jaundice as a late sign
clinical liver symptoms -
What is a common complication from extensive liver metastasis?
Liver failure with ascites and coagulopathy.
complications liver cancer -
What should be done for patients with metastatic disease to the liver?
They should be discussed at a multidisciplinary tumor board and referred to a medical oncologist.
management liver oncology -
For colorectal liver metastases, liver resection is recommended due to the tumour biology's favourable nature.
management liver colorectal -
What is the overall frequency of recurrence for liver metastases after 5 years?
60-80% recurrence at 5 years.
statistics liver recurrence -
What is a characteristic imaging finding for liver metastases on CT?
Hyperdense on arterial phase
Uniform density
Hypodense on arterial phase
Cystic appearance
imaging liver ct -
What is a hepatic abscess?
A pus-filled area in the liver, usually in the right lobe, occurring secondary to bacterial sepsis.
pathology liver -
What organisms can cause a hepatic abscess?
- Klebsiella
- E. coli
- Proteus vulgaris
- Streptococcus milleri/faecalis
- Staphylococcus epidermidis
- Bacteroides fragilis
microbiology bacteria -
What are the risk factors for hepatic abscess?
- Diabetes
- Immunocompromised status
- Underlying hepatobiliary disease
- Elderly age
risk_factors health -
What is the most common route of infection for hepatic abscess?
Biliary tree: direct spread from biliary infections (60%).
pathophysiology infection -
What are common clinical presentations of hepatic abscess?
- Spiking fever
- Abdominal pain
- Jaundice
- Hepatomegaly
- Nonspecific symptoms
signs symptoms -
What is the most definitive imaging technique for diagnosing hepatic abscess?
CT scanning is used to exclude liver tumors and confirm diagnosis.
imaging diagnosis -
What laboratory findings indicate a hepatic abscess?
- Leukocytosis
- Elevated CRP/ESR
- Deranged LFTs
- Blood/pus cultures (e.g. Klebsiella)
investigations lab_tests -
A hepatic abscess often arises due to infections in the biliary system, with a common cause being ascending cholangitis.
pathophysiology infection -
What should be done if resuscitation is needed?
Resuscitate if necessary.
management treatment -
What is crucial for monitoring patients?
Close monitoring of vitals with strict IO charting.
monitoring management -
What complications should be watched for?
Klebsiella endophthalmitis, especially in diabetic patients.
complications klebsiella -
What are the empirical antibiotics for pyogenic liver abscess?
- IV ceftriaxone 1gm every 12 hours
- Metronidazole 500mg every 8 hours
antibiotics treatment -
What is the total duration of antibiotic treatment?
4-6 weeks, counting from the drainage date.
treatment antibiotics -
When is drainage indicated?
If abscess > 3cm.
drainage management -
What is required for a colonoscopy in patients >50 years with DM and K pneumoniae PLA?
To rule out colonic malignant lesions.
colonoscopy screening -
What is a contraindication for percutaneous drainage?
Ascites.
contraindications drainage -
What is the gold standard for treating liver abscesses?
Open drainage (OD).
drainage management -
What are the advantages of laparoscopic drainage?
- Shorter surgery duration
- Less blood loss
- Faster recovery
laparoscopic treatment -
What is the definition of hepatic amoebic abscess?
Hepatic amoebic abscess is caused by liquefaction necrosis, filled with blood and liquefied liver tissue, resembling 'anchovy sauce'.
medical definitions -
How much more frequent is hepatic amoebic abscess in adult men compared to women?
7-10 times more frequent.
epidemiology gender -
What protozoan causes amoebiasis?
Entamoeba histolytica.
microbiology protozoa -
What is the transmission route of hepatic amoebic abscess?
Transmission is faecal-oral; humans are the principal host.
transmission infectious_diseases -
What is a common clinical presentation of hepatic amoebic abscess?
- Persistent fever
- Right upper quadrant pain
- Diarrhoea (in <1/3 of patients)
clinical_presentation symptoms -
What is a diagnostic method for hepatic amoebic abscess?
Ultrasound or CTAP is used to confirm the presence of a liver abscess.
diagnosis imaging -
What is the first-line treatment for hepatic amoebic abscess?
Metronidazole (750mg oral TDS or IV 500mg QDS for 7-10 days).
management treatment -
What complications can arise from hepatic amoebic abscess?
- Rupture causing peritonitis
- Bacterial superinfection
- Free rupture into the peritoneal cavity
complications risks -
What is the mortality rate in complicated cases of hepatic amoebic abscess?
Mortality can be as high as 20%.
mortality complications
Surgical Anatomy of the Liver
Liver Anatomy
Divisions of the Liver
- Anatomical division: Right and left lobes separated by the falciform ligament.
- Functional division: Defined by the gallbladder fossa and inferior vena cava (Cantlie's Line).
- Lobes and segments:
- Left anatomical division: Segments II & III.
- Functional segments: 4 main sections based on blood supply.
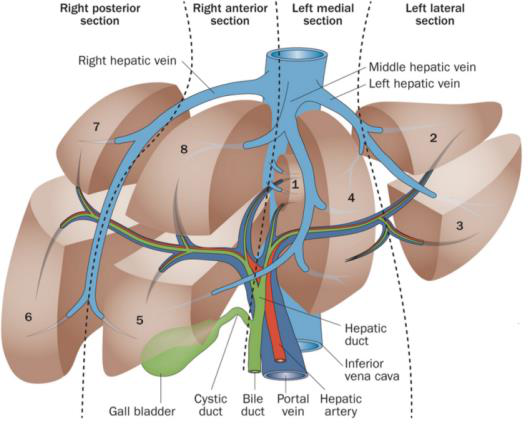
Ligaments around the Liver
- Round Ligament (ligamentum teres): Remnant of obliterated umbilical vein.
- Falciform Ligament: Attaches liver to the anterior abdominal wall.
- Coronary Ligament: Surrounds the liver; also left and right triangular ligaments.
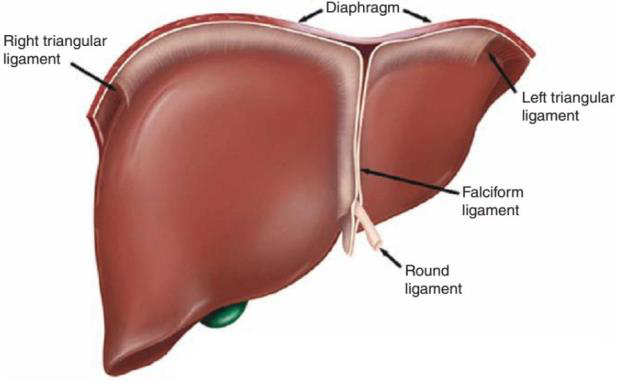
Blood Supply
Arterial & Venous Blood Supply
- Portal Vein: 75% of liver blood supply; formed by the confluence of splenic and superior mesenteric veins.
- Hepatic Artery Proper: 25%; branches from the coeliac trunk.
- Hepatic Veins:
- Right hepatic vein: Drains segments V-VIII.
- Middle hepatic vein: Drains segments IV, V, VIII.
- Left hepatic vein: Drains segments II-III.
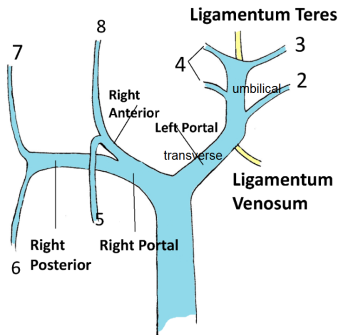
Functions of the Liver
Physiological Functions
- Bile Production: Governed by enterohepatic circulation and gut hormones (CCK).
- Metabolism:
- Carbohydrate: Glycogenesis and glycogenolysis.
- Protein: Amino acid conversion and urea synthesis.
- Lipids: Lipogenesis and lipolysis.
| Function | Process |
|---|---|
| Carbohydrate | Gluconeogenesis, Glycogenesis |
| Protein | Amino acid degradation, Urea synthesis |
| Lipid | Lipogenesis, Lipolysis |
| Lactate | Cori Cycle (lactate to glucose) |
Portal Hypertension
Definition
Portal Hypertension is defined as a hepatic venous pressure gradient (HVPG) ≥ 6 mmHg (normal: 3-5 mmHg). - Key pressure thresholds: - ≥ 10 mmHg: High risk of varices. - ≥ 12 mmHg: High risk of bleeding.
Pathophysiology
- Caused by mechanical obstruction in the portal venous system (e.g., cirrhosis). Using Ohm's and Poiseuille's Law to understand relationships among flow, pressure, and resistance:
-
\[ V = IR \]
-
\[ Q = \frac{\Delta P}{R} \]

Ascites
Pathogenesis (in Cirrhosis)
- Portal hypertension leads to increased splanchnic NO release.
- Decreased effective blood volume.
- Renal hypoperfusion: activates RAAS, increases aldosterone, leading to salt and water retention.
Clinical Presentation
- Symptoms: Abdominal distension, discomfort, shortness of breath, low-grade fever.
Investigations
- Biochemical: Full blood count, liver function test, and serum-ascites albumin gradient (SAAG).
| SAAG ≥ 1.1g/dL | Conditions |
|---|---|
| Liver Cirrhosis | Alcoholic Hepatitis, Portal Vein Thrombosis |
Hepatocellular Carcinoma (HCC)
Epidemiology
- Most common type of primary liver cancer, mainly in males.
- Risk factors include chronic liver disease (cirrhosis) and hepatitis B/C.
Clinical Presentation
- Asymptomatic
- Local symptoms: abdominal pain, jaundice, weight loss.
- General symptoms: fever, malaise, ascites.
Diagnosis
- Imaging: Triphasic CT scans as the gold standard.
- AFP levels may indicate HCC but are not definitive.

Management Approaches
Treatment Modalities for HCC
Curative
- Surgical resection, liver transplantation (Milan Criteria).
Palliative
- Local: RFA, microwave ablation.
- Regional: TACE (Trans-arterial chemoembolization).
- Systemic: Sorafenib.
Prognosis
- Poor without treatment; approximately 5-year survival post-treatment is 18%.