デッキが消える前に保存しよう
このフラッシュカードはまだ保存されてないよ — 離れると消えちゃう。無料アカウントを作ると保存できて、下の機能も全部使えるようになるよ。
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
What is the primary function of fibrillin-1 regarding TGF-beta signaling?
What occurs in Marfan syndrome when fibrillin is reduced or absent?
What is the cellular mechanism leading to spontaneous pneumothorax in Marfan syndrome?
What condition is a classic hallmark of Marfan syndrome but not observed in Loeys-Dietz syndrome?
TGF-beta hyperactivation
Ectopia lentis
Thoracic aortic aneurysm
Autosomal dominant inheritance
What is the primary cause of Loeys-Dietz syndrome?
What are two distinct classes of genes associated with thoracic aortic aneurysms?
How are pathogenic mutations in FBN1 typically characterized in Marfan syndrome?
What causes the hyper-accumulation of receptor protein in TGFBR1/TGFBR2-driven conditions?
How do researchers validate the pathogenic impact of missense mutations in cytoskeletal genes?
What role does Angiotensin II play in vascular smooth muscle cells according to recent research?
Which disorder is described as the third most common muscular dystrophy in adults?
Marfan syndrome
Facioscapulohumeral muscular dystrophy (FSHD)
Loeys-Dietz syndrome
Duchenne muscular dystrophy
Based on the cellular signaling diagram, what is one major consequence of inflammation in the context of Marfan syndrome?
What is the defining physical pattern of muscle wasting in FSHD?
On which chromosomal region does the genetic defect of FSHD map?
What is the typical number of D4Z4 repeat units in healthy individuals?
What happens when the \(3.3\text{ kb}\) D4Z4 units express the DUX4 transcription factor?
Why is the 4QA allele of the D4Z4 array considered permissive?
Why is the 4QB allele of the D4Z4 array considered non-permissive?
What is the primary cause of FSHD Type 1?
What are the main epigenetic regulator mutations associated with FSHD Type 2?
What is the typical D4Z4 array size range for patients with FSHD Type 2?
Which diagnostic method was historically used to study D4Z4 fragments spanning hundreds of kilobases?
Which modern diagnostic approach is replacing traditional methods for detecting chromosome 4q35 variants?
Have clinical drug trials for antisense oligonucleotides targeting the DUX4 transcript proven successful?
What is the most effective evidence-based management strategy for patients with FSHD?
Which genetic mutation is NOT typically associated with FSHD Type 2?
SMCHD1
DUX4
DNMT3B
LRIF1
Flashcards in this deck (26)
-
What is the primary function of fibrillin-1 regarding TGF-beta signaling?
Fibrillin-1 binds and sequesters TGF-beta, keeping the precursor inactivated until released.
-
What occurs in Marfan syndrome when fibrillin is reduced or absent?
TGF-beta is secreted without regulation, leading to excessive activation of downstream signaling cascades.
-
What is the cellular mechanism leading to spontaneous pneumothorax in Marfan syndrome?
Structural disruption of the alveoli, resulting in the formation of large, air-filled bubbles in the lung tissue.
-
What condition is a classic hallmark of Marfan syndrome but not observed in Loeys-Dietz syndrome?
TGF-beta hyperactivation
Ectopia lentis
Thoracic aortic aneurysm
Autosomal dominant inheritance
-
What is the primary cause of Loeys-Dietz syndrome?
Gain-of-function mutations in TGF-beta receptors (TGFBR1 and TGFBR2) or downstream signaling molecules like SMAD3.
-
What are two distinct classes of genes associated with thoracic aortic aneurysms?
- Genes modifying extracellular matrix or TGF-beta signaling (e.g., FBN1, TGFBR1, COL3A1)
- Genes encoding proteins for the smooth muscle cytoskeleton (e.g., ACTA2, MYH11, MYLK)
-
How are pathogenic mutations in FBN1 typically characterized in Marfan syndrome?
They are predominantly driven by loss-of-function mutations leading to haploinsufficiency.
-
What causes the hyper-accumulation of receptor protein in TGFBR1/TGFBR2-driven conditions?
Truncating mutations lead to the production of a hyper-stable protein lacking its terminal degradation domain, which accumulates and causes unmitigated signaling.
-
How do researchers validate the pathogenic impact of missense mutations in cytoskeletal genes?
By using Saccharomyces cerevisiae (yeast) models to express normal and abnormal actin and visually observe structural aberrations in the microtubule-cytoskeletal network.
-
What role does Angiotensin II play in vascular smooth muscle cells according to recent research?
It upregulates TGF-beta activity.
-
Which disorder is described as the third most common muscular dystrophy in adults?
Marfan syndrome
Facioscapulohumeral muscular dystrophy (FSHD)
Loeys-Dietz syndrome
Duchenne muscular dystrophy
-
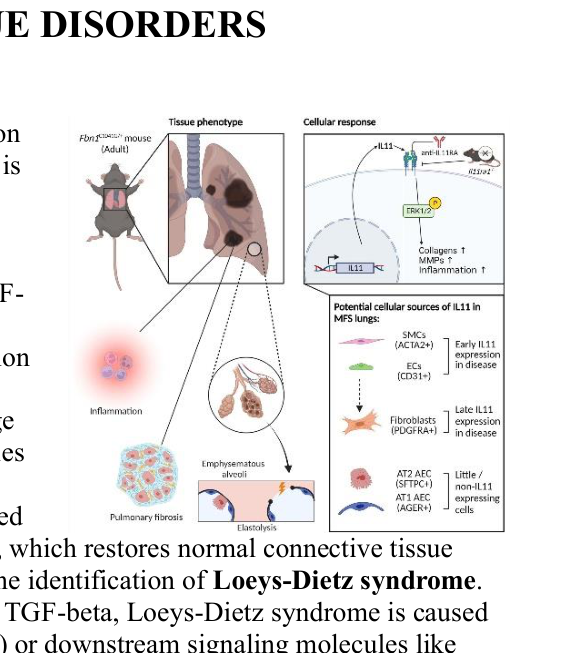
Based on the cellular signaling diagram, what is one major consequence of inflammation in the context of Marfan syndrome?
Increased levels of collagen and MMPs (matrix metalloproteinases).
-
What is the defining physical pattern of muscle wasting in FSHD?
It is a highly asymmetric pattern involving facial muscles, such as the orbicularis oculi and oris, and scapular stabilizer muscles.
-
On which chromosomal region does the genetic defect of FSHD map?
The subteleomeric region of chromosome 4q35.
-
What is the typical number of D4Z4 repeat units in healthy individuals?
Between 21 and over 100 units.
-
What happens when the \(3.3\text{ kb}\) D4Z4 units express the DUX4 transcription factor?
It triggers structural atrophy and rapid cell apoptosis in skeletal muscle.
-
Why is the 4QA allele of the D4Z4 array considered permissive?
It contains a functional polyadenylation signal that stabilizes the DUX4 mRNA.
-
Why is the 4QB allele of the D4Z4 array considered non-permissive?
It lacks the functional polyadenylation signal, making the transcript unstable and subject to degradation.
-
What is the primary cause of FSHD Type 1?
A structural contraction of the D4Z4 array to fewer than 11 units, leading to loss of hypermethylation.
-
What are the main epigenetic regulator mutations associated with FSHD Type 2?
Heterozygous loss-of-function mutations in SMCHD1, DNMT3B, or LRIF1.
-
What is the typical D4Z4 array size range for patients with FSHD Type 2?
Between 11 and 20 units, known as the gray zone.
-
Which diagnostic method was historically used to study D4Z4 fragments spanning hundreds of kilobases?
Southern Blotting.
-
Which modern diagnostic approach is replacing traditional methods for detecting chromosome 4q35 variants?
Long-read sequencing technologies.
-
Have clinical drug trials for antisense oligonucleotides targeting the DUX4 transcript proven successful?
No, they have failed to generate therapeutic successes.
-
What is the most effective evidence-based management strategy for patients with FSHD?
Structured physical exercise and neuromuscular electrical stimulation.
-
Which genetic mutation is NOT typically associated with FSHD Type 2?
SMCHD1
DUX4
DNMT3B
LRIF1