더 많은 기능을 잠금 해제하려면 가입하세요
- 이 덱을 계정에 저장하기
- 간격 반복으로 플래시카드 공부하기
- Anki(.apkg) 또는 PDF로 내보내기
- 문서 최대 100페이지까지 처리 가능
- PDF와 문서에서 이미지 추출
- PDF와 문서에서 더 정확한 텍스트 추출
- 더 발전된 AI 모델로 더 나은 플래시카드 생성
이 덱의 플래시카드 (33)
-
What immediate action is recommended for a patient with pulmonary embolism (PE) as a medical emergency?
Call a met call and arrange ICU admission
emergency pe -
What initial oxygen therapy is recommended for suspected PE?
15 L of oxygen via a non‑rebreather mask
management oxygen -
What must be confirmed about the patient's status during initial PE management?
Make sure they are hemodynamically stable
management hemodynamics -
investigations imaging
-
investigations labs
-
investigations labs
-
Which cardiac biomarkers and related tests are listed for PE evaluation?
- BNP
- Troponins
- Coagulation studies
investigations cardiac -
investigations ecg
-
What key history points should be asked about possible DVT when assessing for PE?
- Signs of DVT
- Calf tenderness
- Asymmetrical swelling
history dvt -
Which recent activities or exposures should be asked about in PE history?
- Recent mobilization
- Recent long haul travel
- Use of blood thinners
history risk -
Which past medical and medication history items are important for PE assessment?
- Cancer history and treatments
- Previous thromboembolic events
- Coagulopathies
history pastmedical -
What aspects of symptoms should be asked about for suspected PE?
- Chest pain and if it is pleuritic
- Haemoptysis
- How the patient feels
history symptoms -
What examination components are listed for a patient with suspected PE?
Head-to-toe exam including lung and heart auscultation, carotids, renal bruits, calf tenderness, vitals, peripheral vascular, neurological
examination pe -
wells imaging
-
What is the recommended pathway if the Wells score is below 4?
Do a D-dimer and other investigations; if D-dimer is high or cause not found, do CTPA and consult ED/ICU
wells pathway -
What CXR signs may indicate pulmonary embolism?
- Knuckle sign
- Palla sign
- Hampton hump
- Westermark sign
- Fleischner sign
- Chang sign
- Polo mint sign
- Railway sign
- Pleural effusion
- Saddle embolism
radiology pulmonaryembolism cxr -
What pregnancy-related tests or questions should be asked in a woman with suspected PE?
Ask about contraceptives and pregnancy and perform a bHCG
history pregnancy pe -
When is a patient with PE considered haemodynamically unstable?
If systolic blood pressure is <90 mmHg or drops >40 mmHg from baseline
definitions hemodynamics pe -
What is the recommended alteplase regimen for thrombolysis in PE for patients >65 kg?
10 mg IV bolus followed by 90 mg infusion over 2 hours
thrombolysis alteplase pe -
What is the recommended alteplase regimen for thrombolysis in PE for patients <65 kg?
10 mg IV bolus followed by 1.5 mg/kg infusion over 2 hours
thrombolysis alteplase pe -
What are typical maintenance anticoagulation options after initial PE treatment?
LMWH (enoxaparin, dalteparin) or oral anticoagulants (NOACs such as apixaban or rivaroxaban); warfarin or dabigatran as alternatives
anticoagulation pe treatment -
What do the 2021 American guidelines suggest about NOACs for cancer-associated VTE?
NOACs can be used for cancer-associated VTE
guidelines cancer noacs -
When should an IVC filter be considered in PE management?
If anticoagulation is contraindicated or there is failure of appropriate anticoagulation/recurrent PE
intervention ivcfilter pe -
Which anticoagulants are contraindicated in pregnancy for PE?
Warfarin (teratogenic) and DOACs such as dabigatran (likely cross placenta) are contraindicated
pregnancy anticoagulation pe -
Which anticoagulant is used in massive PE with haemodynamic compromise or when rapid adjustment/reversal is needed in pregnancy?
Unfractionated heparin
pregnancy heparin pe -
What is the recommended management of enoxaparin in pregnancy and postnatally for PE?
Continue enoxaparin for the remainder of pregnancy and at least 6 weeks postnatally for a total of 3 months; postnatally you can switch to a DOAC
pregnancy enoxaparin pe -
What is the typical duration of anticoagulant therapy after a PE when no ongoing risks exist?
Typically stopped at 3 months unless factors predicting recurrence are present
duration anticoagulation pe -
alternatives fondaparinux pe
-
What is the immediate priority in suspected acute pulmonary embolism?
- Emergency recognition and initial resuscitation
pulmonaryembolism emergency -
Which clinical pathway components are used for diagnosing pulmonary embolism?
- Wells score, D-dimer, CTPA pathway
pulmonaryembolism diagnosis -
What defines the subgroup of pulmonary embolism patients who may need thrombolysis?
- Hemodynamic instability indicates consideration of thrombolysis
pulmonaryembolism thrombolysis -
What are the two core aspects of medical management after acute PE stabilization?
- Anticoagulation options and duration of therapy
pulmonaryembolism anticoagulation -
What special patient group requires tailored PE management considerations?
- Pregnancy and special situations
pulmonaryembolism pregnancy
Pulmonary Embolism (PE) — Quick Study Notes
Overview
- PE is a medical emergency; activate a MET call and consider ICU for unstable patients.
- Immediate goals: secure oxygenation, assess hemodynamics, and start appropriate anticoagulation or thrombolysis.
Key definitions
- Hemodynamically unstable PE: systolic blood pressure \(\text{SBP} < 90\ \text{mmHg}\) or a drop of \(>40\ \text{mmHg}\) from baseline.
- Wells score used for pre-test probability to guide imaging and D-dimer use.
Initial emergency management (first minutes)
- Give high-flow oxygen: \(15\ \text{L/min}\) via non-rebreather mask.
- Call MET/critical care and prepare for possible ICU transfer.
- Monitor vitals continuously, establish IV access, and obtain urgent investigations.
History — important points to ask
- Recent immobility or long-haul travel; recent surgery or trauma.
- Symptoms: pleuritic chest pain, dyspnea, hemoptysis, syncope.
- Signs or history of DVT: calf pain, unilateral swelling, prior VTE.
- Anticoagulant use, contraceptives, pregnancy (bHCG), active cancer, thrombophilia.
- Renal disease (affects DOAC use and contrast for CTPA).
- Comorbidities: diabetes, hypertension, bleeding history, alcohol and smoking.
Examination — focused elements
- Full head-to-toe exam but emphasise:
- Respiratory: breath sounds, pleural rubs, effusion signs.
- Cardiovascular: tachycardia, raised JVP, new murmur.
- Limbs: calf tenderness, unilateral swelling, Homan's sign (limited value).
- Neurological and perfusion: syncope, hypotension, cool peripheries.
Investigations
- Immediate:
- ECG — look for sinus tachycardia and S1Q3T3 pattern.
- Bloods: FBC, EUC (renal function), LFTs, CRP, coagulation studies, troponin, BNP.
- D-dimer (when pre-test probability is low or moderate).
- ABG if respiratory compromise.
- Blood cultures if sepsis suspected.
- Imaging:
- CTPA is the diagnostic test of choice when indicated.
- Chest X-ray helpful to exclude other causes and show PE signs (see image).
Chest X-ray signs of PE
- Classic but uncommon radiographic signs: Knuckle sign, Palla sign, Hampton hump, Westermark sign, Fleischner sign, Polo-mint, Railway sign, pleural effusion, saddle embolus.
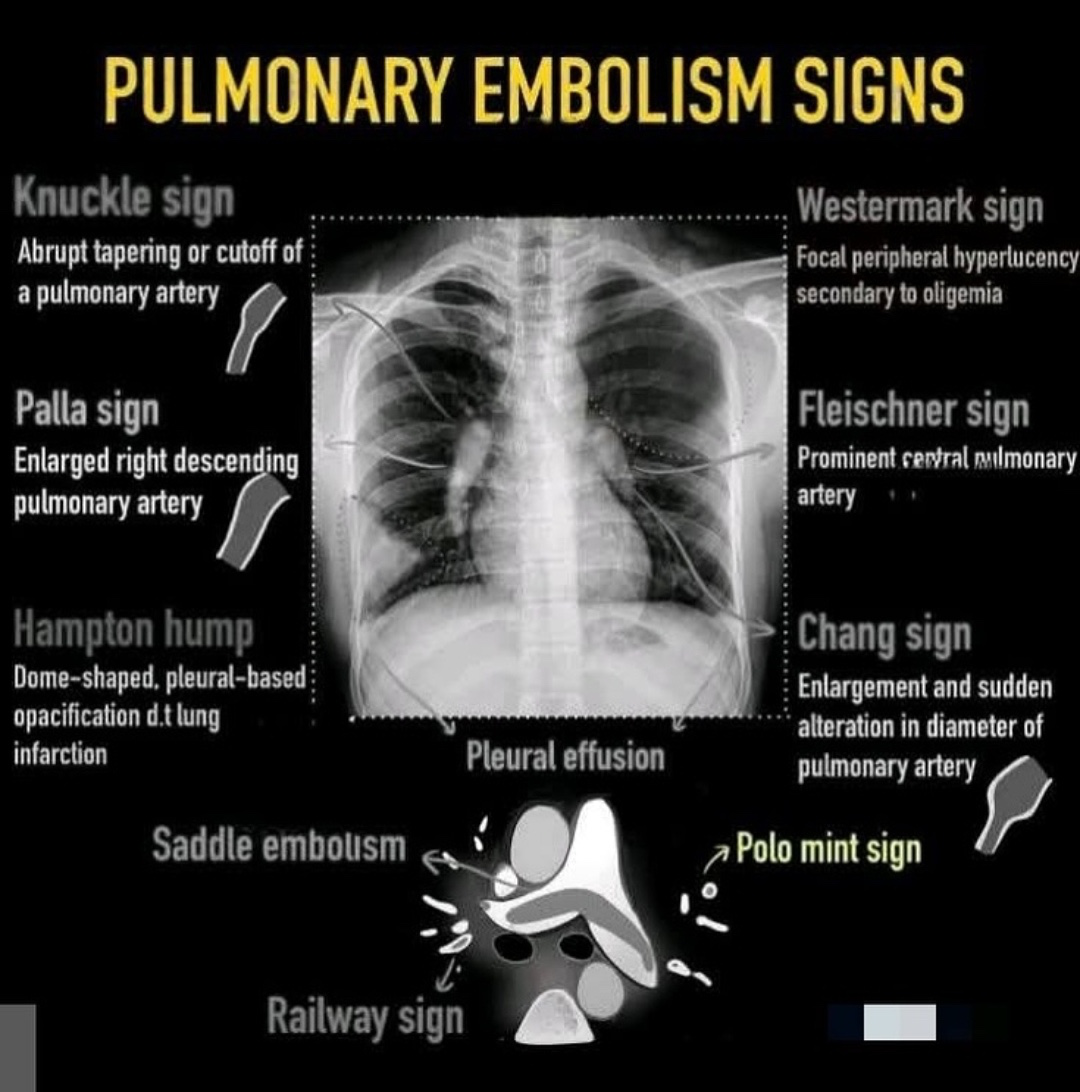
Alt text: Diagram of chest X-ray signs of pulmonary embolism.
When to do CTPA
- If Wells score > 4 → proceed to CTPA.
- If Wells score ≤ 4 → get D-dimer; if D-dimer elevated or suspicion persists, then do CTPA.
Hemodynamic risk stratification
- Unstable (massive PE): shock, hypotension (\(\text{SBP} < 90\)) or large drop in BP.
- Stable (submassive or low risk): normotensive but may have RV strain or elevated biomarkers.
Definitive management
- General: start anticoagulation unless contraindicated.
- If haemodynamically unstable (massive PE): consider systemic thrombolysis (alteplase):
- For patients >65 kg: \(10\ \text{mg}\) IV bolus + \(90\ \text{mg}\) infusion over \(2\ \text{h}\).
- For patients <65 kg: \(10\ \text{mg}\) IV bolus + \(1.5\ \text{mg/kg}\) infusion over \(2\ \text{h}\).
- Give in monitored setting (ICU) and prepare for bleeding management.
- If thrombolysis contraindicated or fails: consider surgical or catheter-directed embolectomy.
Anticoagulation (maintenance)
- First-line for most stable patients: NOACs/DOACs (e.g., apixaban, rivaroxaban).
- Alternatives: LMWH (enoxaparin, dalteparin) or warfarin if DOACs unsuitable.
- Cancer-associated VTE: guidelines now support DOACs as an option; consider bleeding risk and drug interactions.
- Typical planned duration: at least \(3\) months; extend if ongoing risk (active cancer, recurrent VTE, thrombophilia).
- Use an IVC filter only when anticoagulation is contraindicated or recurrent PE despite adequate therapy.
Pregnancy and peripartum
- Avoid warfarin (teratogenic) and most DOACs (placental crossing uncertain).
- Use LMWH (enoxaparin) throughout pregnancy; continue at least \(6\) weeks postnatally for a total of \(3\) months.
- Unfractionated heparin may be preferred in massive PE or when rapid reversal is needed around delivery.
- Consider fondaparinux if heparin intolerance (e.g., HIT) and expert input.
Special considerations
- Renal impairment: adjust or avoid certain DOACs and contrast for CTPA; check renal function before DOACs.
- Bleeding risk: balance anticoagulation vs. thrombolysis; involve haematology when complex.
- Ongoing monitoring: observe for RV dysfunction (echo), rising troponin or BNP indicating higher risk.
Practical algorithm (brief)
- Airway/oxygen: \(15\ \text{L/min}\) NRB; call MET/ICU.
- Assess vitals and compute Wells score.
- If Wells \(>4\) → CTPA. If Wells \(\le 4\) → D-dimer, then CTPA if elevated.
- If unstable → thrombolyse (follow dosing) and ICU care.
- Start anticoagulation in all without contraindication; decide long-term agent and duration.
Key takeaways
- Treat PE as an emergency; stabilise airway/oxygenation and circulation first.
- Use Wells + D-dimer to decide imaging; CTPA is diagnostic standard.
- Hemodynamically unstable patients may need thrombolysis or embolectomy.
- Most stable patients receive DOACs or LMWH, typically for at least \(3\) months.