Save your deck before it's gone
These flashcards aren't stored yet — they'll disappear when you leave. Create a free account to keep them, and unlock everything below.
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
Hypertension in adults is defined as a systolic blood pressure of ≥ 140 mmHg or a diastolic blood pressure of ≥ 90 mmHg.
Primary hypertension is described as hypertension that is chiefly of unknown cause or attributable to a pre-existing condition.
Chronic hypertension typically results in thickening and inelasticity of arterial walls and hypertrophy of the left ventricle.
Hypertension is a risk factor for major organ diseases including cerebrovascular disease, cardiovascular disease, kidney disease, and eye disease.
Blood pressure measurement is a clinical procedure; an example image of a clinician measuring BP is shown as supplementary material on the answer side.

What common clinical tool is used to measure arterial blood pressure?
The term 'abnormally high arterial blood pressure' refers to sustained elevations in systolic and/or diastolic pressure above defined adult thresholds (e.g., ≥ 140/90 mmHg).
Blood pressure (BP) is the pressure exerted on the walls of the blood vessels.
Systolic BP: - the maximum blood pressure exerted by the blood against the artery walls - Corresponds to contraction of the ventricles (systole)
Diastolic BP: - the minimum pressure in the main arteries - Corresponds to relaxation of the ventricles (diastole)
Blood pressure equals cardiac output × systemic vascular resistance.
Cardiac factors that influence blood pressure include: - heart rate - contractibility
Drugs listed that act on cardiac factors include: - beta blockers - calcium channel blockers - centrally acting adrenergics
Circulating volume influences BP via: - salt - aldosterone
Drugs affecting circulating volume listed are: - ACE inhibitors - diuretics
Examples of vasodilator or related drug types given include: - vasodilators - prostaglandins - ACE inhibitors - calcium channel blockers - angiotensin II blockers
Peripheral sympathetic receptor types and related agents: - Alpha: alpha1 blockers - CNS: centrally acting adrenergics (alpha2) - Beta: beta blockers
Name three cardiac factors that influence blood pressure: - heart rate - contractibility - cardiac output (derived)
Illustration: 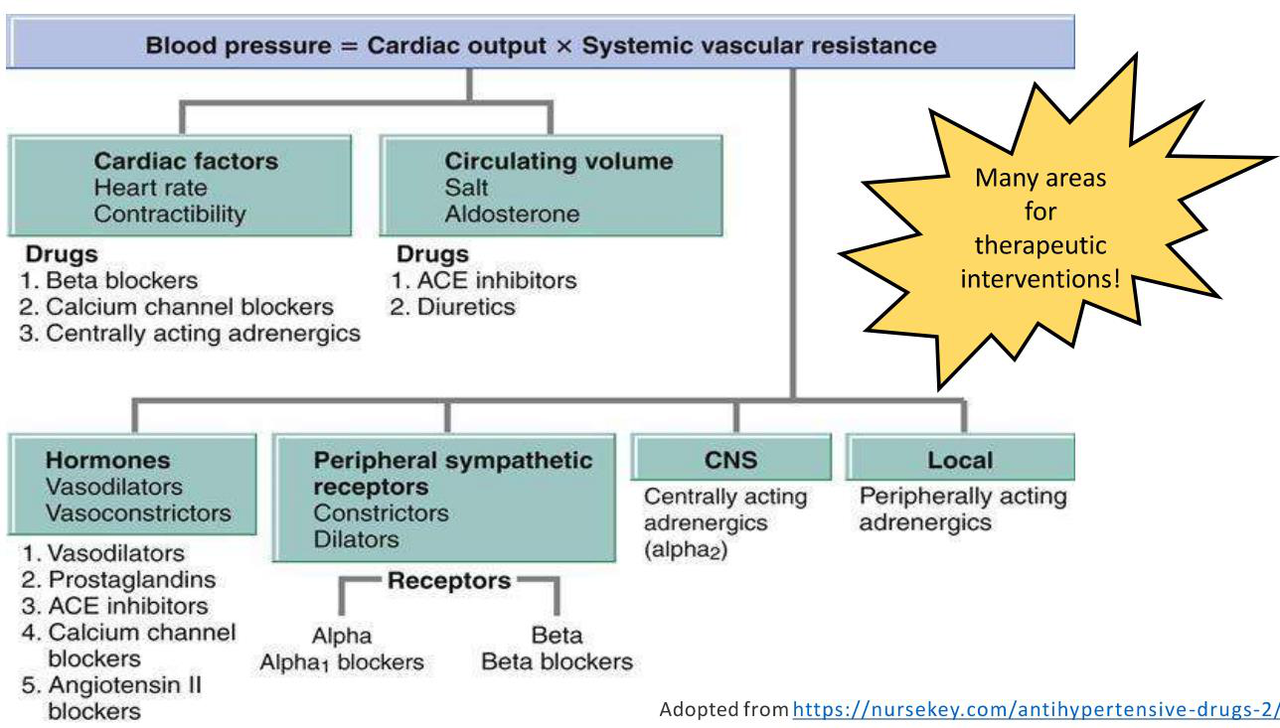
A common blood pressure (BP) diagnostic cutoff is approximately 140/90 mmHg and worldwide prevalence of hypertension is about 30%.
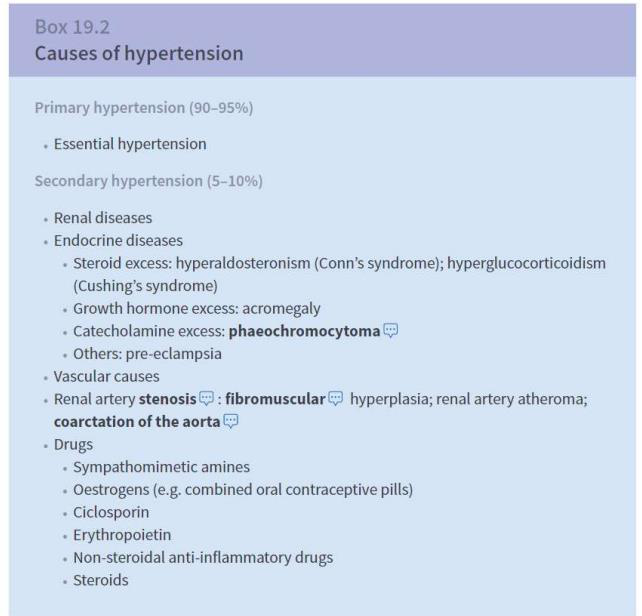
Primary (essential) hypertension is characterized by no identifiable cause and accounts for 90-95% of hypertension cases.
Secondary hypertension has an identifiable known cause and represents 5-10% of hypertension cases.
Major categories of causes for secondary hypertension include: - renal diseases - endocrine diseases - vascular causes - drugs
Endocrine causes of secondary hypertension listed include: - steroid excess (hyperaldosteronism, Cushing's) - growth hormone excess (acromegaly) - catecholamine excess (phaeochromocytoma) - pre-eclampsia
Vascular causes of secondary hypertension include: - renal artery stenosis (fibromuscular hyperplasia; renal artery atheroma) - coarctation of the aorta
Drugs that can cause or worsen hypertension include: - sympathomimetic amines - oestrogens (e.g., combined oral contraceptive pills) - ciclosporin - erythropoietin - non-steroidal anti-inflammatory drugs - steroids
Most cases of hypertension are asymptomatic.
Severe hypertension may present with: - headache - visual disturbances - evidence of target organ damage

Risk of stroke/CHD increases by 35-40% with every 5 mmHg increase in blood pressure.
Risk of ocular complications (e.g., retinopathy) is doubled with every 10 mmHg increase in blood pressure.
Risk of cardiovascular disease (CVD) doubles for every 20/10 mmHg rise in blood pressure.
There is a 25% increased risk of renal failure with every 5 mmHg increase in blood pressure.
People with increased blood pressure have a 6-fold higher risk of heart failure.
Common clinic blood pressure measurement methods include: - Manual (clinic) - Automatic (clinic)
Ambulatory blood pressure monitoring (ABPM) protocol: use ABPM for 1 day with a minimum of 14 measurements.
Home blood pressure monitoring (HBPM) schedule: measure twice a day for 4-7 days.
Healthcare professionals performing blood pressure measurement must be adequately trained.
BP devices used for measurement must be validated, maintained and calibrated.
To standardise the measurement environment ensure the person is: - quiet - seated - arm outstretched, supported and relaxed
Blood pressure should be measured in both arms using an appropriate cuff size.
When measuring blood pressure, clinicians should take two measurements.
If pulse irregularity is present, take care and measure blood pressure manually.
Patients with type 2 diabetes mellitus should have blood pressure measured annually.
For suspected secondary causes of hypertension, refer for specialist investigations.
When assessing suspected postural hypotension: first measure blood pressure with the person lying on their back (or seated if lying is inconvenient), then measure again after they have been standing for at least 1 minute.
Postural hypotension is defined as a fall in blood pressure on standing of: systolic ≥ 20 mmHg or diastolic ≥ 10 mmHg measured after at least 1 minute standing.
If the systolic fall is ≥ 20 mmHg or diastolic fall ≥ 10 mmHg after 1 minute standing: consider likely causes (eg review medications), manage appropriately (eg fall prevention), measure subsequent blood pressures with the person standing, and consider specialist referral if symptoms persist.
If symptoms suggest postural hypotension but the blood pressure drop is below thresholds and the baseline was taken seated: repeat measurements starting with the person lying on their back.
Consider referring for specialist assessment if blood pressure measurements do not confirm postural hypotension despite suggestive symptoms.
If clinic blood pressure is ≥ 140/90 mmHg, offer ambulatory blood pressure monitoring (ABPM). An alternative is home blood pressure monitoring (HBPM).
While awaiting confirmation of hypertension, clinicians should: - investigate for target organ damage - undertake a cardiovascular risk assessment using QRISK3
If clinic blood pressure is ≥ 180/120 mmHg, refer for same-day specialist review and assessment if any of the following are present: - suspected phaeochromocytoma - signs of retinal haemorrhage or papilloedema - life-threatening symptoms (e.g., new confusion, chest pain, heart failure, acute kidney injury)
Suspected phaeochromocytoma may present with symptoms such as labile or postural hypotension, headache, palpitations, pallor, abdominal pain or diaphoresis.
If clinic BP is ≥ 180/120 mmHg but there are no signs or symptoms for same-day referral, clinicians should: - carry out investigations for target organ damage as soon as possible
After investigations for target organ damage: - If damage is identified: consider starting antihypertensive drug treatment immediately without ABPM/HBPM - If no damage is identified: confirm diagnosis by repeating clinic BP within 7 days or consider ABPM/HBPM
Stage 1 hypertension is defined as: - Clinic BP 140/90 mmHg – 159/99 mmHg (≥ 140/90 mmHg) - ABPM daytime or HBPM average BP 135/85 mmHg – 149/94 mmHg (≥ 135/85 mmHg)
Stage 2 hypertension is defined as: - Clinic BP 160/100 mmHg – 180/120 mmHg (≥ 160/100 mmHg) - ABPM daytime or HBPM average BP ≥ 150/95 mmHg
Stage 3 (severe) hypertension is defined as: - Clinic BP ≥ 180/120 mmHg
For all patients diagnosed with hypertension offer cardiovascular risk assessment (QRISK3).
For all patients diagnosed with hypertension offer a urine sample to measure albumin:creatinine ratio and to test for haematuria.
For all patients diagnosed with hypertension offer a biochemistry sample to measure: - HbA1C - U&Es - creatinine and eGFR - lipid profile
For all patients diagnosed with hypertension offer examination of the fundi to check for the presence of hypertensive retinopathy.
For all patients diagnosed with hypertension perform a 12-lead ECG.
For all patients diagnosed with hypertension discuss cardiovascular risk and discuss different treatment options with the patient.
Weight loss reduces blood pressure by approximately 5-20 mmHg per 10 kg lost.
A healthy diet for BP control is rich in fruit and vegetables, includes low-fat dairy products, and has reduced saturated fats.
Recommended daily salt intake to reduce blood pressure is < 6 g NaCl per day.
Regular aerobic physical activity is advised as an exercise measure to lower blood pressure.
Alcohol guidance: maintain moderate consumption and reduce intake if consumption is excessive.
Caffeine guidance: adopt moderate consumption and reduce intake if consumption is excessive.
Address cardiovascular risk factors by promoting smoking cessation and managing dyslipidaemia.
Effective stress management should be part of blood pressure control and reiterated at all stages of care.
Clinic blood pressure under 140/90 mmHg: check BP at least every 5 years and more often if clinic BP is close to 140/90 mmHg.
If clinic BP is 140/90 to 179/119 mmHg: offer ABPM (or HBPM if ABPM declined or not tolerated), investigate for target organ damage and assess cardiovascular risk.
Average daytime ABPM or HBPM target is under 135/85 mmHg.
Clinic BP 135/85 to 149/94 mmHg (stage 1): offer lifestyle advice and consider drug treatment for these groups: - age ≥80 with clinic BP >150/90 - age <80 with target organ damage, CVD, renal disease, diabetes or 10-year CVD risk ≥10% - age <60 with 10-year CVD risk <10% (consider) - age <40 (consider specialist evaluation)
Clinic BP 150/95 mmHg or more (stage 2): offer lifestyle advice and drug treatment; for age under 40 consider specialist evaluation of secondary causes.
Clinic BP 180/120 mmHg or more: assess for target organ damage as soon as possible; consider starting drug treatment immediately without ABPM/HBPM if target organ damage is present.
Refer for same-day specialist review if accelerated hypertension with retinal haemorrhage or papilloedema, life-threatening symptoms, or suspected pheochromocytoma.
ABPM should be based on average daytime readings, ideally taken spread throughout the day. 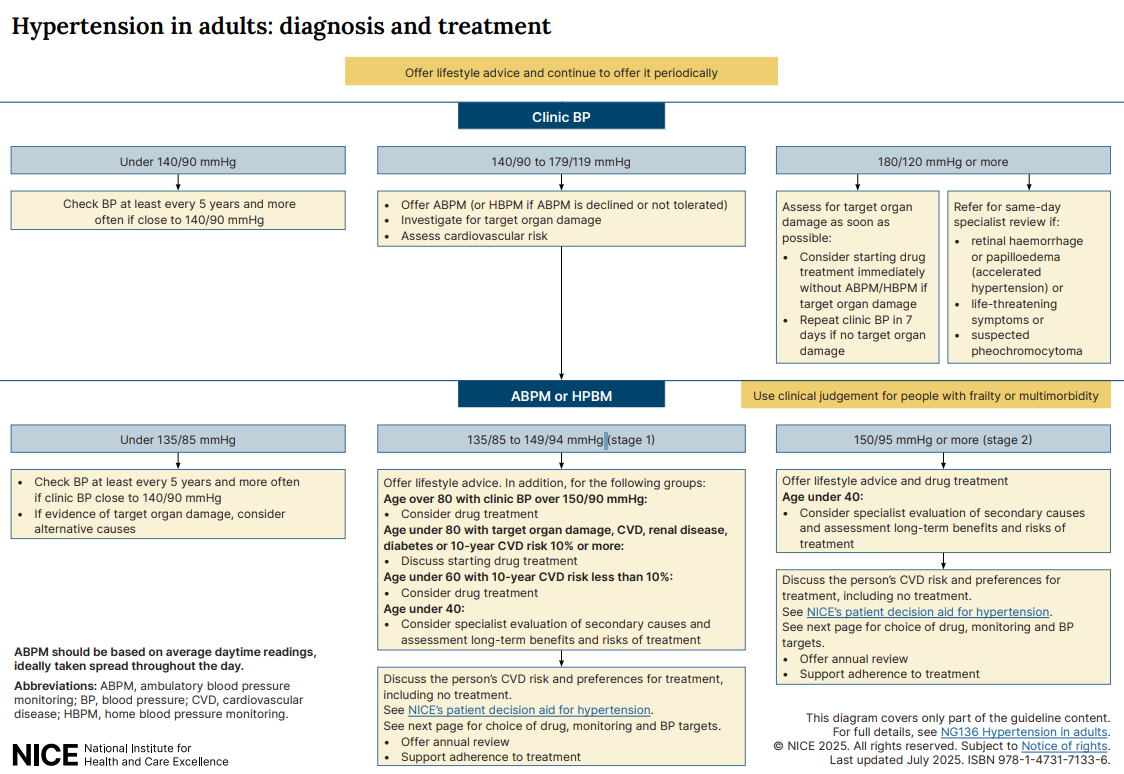
For all stages: offer lifestyle advice throughout, support adherence to treatment and offer annual review when on treatment.
For adults aged < 80 years the BP treatment targets are: - Clinic BP: < 140/90 mmHg - ABPM or HBPM: < 135/85 mmHg
For adults aged ≥ 80 years the BP treatment targets are: - Clinic BP: < 150/90 mmHg - ABPM or HBPM: < 145/85 mmHg
Patients with cardiovascular disease (CVD) should use the same blood pressure thresholds and treatment targets as those without CVD.
For chronic kidney disease (CKD) the BP target is: - < 140/90 mmHg if ACR < 70 mg/mmol - < 130/80 mmHg if ACR ≥ 70 mg/mmol
For type 1 diabetes (T1 DM): - If < 80 years: < 140/90 mmHg if ACR < 70 mg/mmol; < 130/80 mmHg if ACR ≥ 70 mg/mmol - If ≥ 80 years: < 150/90 mmHg regardless of ACR
For type 2 diabetes (T2 DM) the guidance states: the same blood pressure thresholds and treatment targets are used for patients with and without T2 DM.
When assessing postural hypotension, the BP target should be based on standing BP.
In patients with frailty, target organ damage, or multimorbidity the recommendation is to use clinical judgement when setting BP targets.
SIGN 2017 recommends offering antihypertensive drug treatment to adults with T1 or T2 DM if systolic BP is ≥ 140 mmHg and considering treatment even if systolic BP is < 140 mmHg for those at greatest risk, with a suggested target of 130/80 mmHg.
For people aged under 80 with hypertension (with or without type 2 diabetes), type 1 diabetes with ACR < 70 mg/mmol, or CKD with ACR < 70 mg/mmol, the clinic blood pressure target is below 140/90.
For people aged under 80 with type 1 diabetes with ACR ≥ 70 mg/mmol or CKD with ACR ≥ 70 mg/mmol, the clinic blood pressure target is below 130/80.
For people aged 80 and over with hypertension (with or without type 2 diabetes) or type 1 diabetes (any ACR), the clinic blood pressure target is below 150/90.
For people aged 80 and over with chronic kidney disease and ACR < 70 mg/mmol the clinic blood pressure target is below 140/90, and with ACR ≥ 70 mg/mmol the target is below 130/80.
Antihypertensive treatment can increase life expectancy by up to 5 years compared with individuals with uncontrolled hypertension.
A reduction of 10 mmHg systolic or 5 mmHg diastolic may lead to these relative risk changes: - 20% reduction in all major cardiovascular events - 10-15% reduction in all-cause mortality - 35% reduction in strokes - 20% reduction in coronary events - 40% reduction in heart failure
Main antihypertensive drug classes include: - Thiazide-like diuretic - Angiotensin Converting Enzyme (ACE) inhibitor - Angiotensin Receptor Blocker (ARB) - Calcium Channel Blocker (CCB)
ACE inhibitor stands for Angiotensin Converting Enzyme Inhibitor.
ARB stands for Angiotensin Receptor Blocker.
CCB stands for Calcium Channel Blocker.
A thiazide-like diuretic is listed as a diuretic class among antihypertensive drugs.
The main sequential components of the Renin-Angiotensin-Aldosterone System (RAAS) are: - Angiotensinogen - Renin - Angiotensin I - ACE - Angiotensin II
The primary organs producing key RAAS components are: - Liver (angiotensinogen) - Kidney (renin) - Lung (ACE)
Factors that stimulate renin secretion include: - Decreased blood pressure - Decreased sodium delivery to the macula densa - Increased sympathetic tone
Angiotensin II produces the following effects: - Constricts glomerular efferent arteriole - Increases Na+/H+ exchanger activity - Stimulates ADH secretion - Stimulates thirst - Stimulates aldosterone secretion
A systemic consequence associated with increased angiotensin II activity is hypertension.
Main components of the Renin–Angiotensin–Aldosterone System (RAAS):
- angiotensinogen
- renin
- angiotensin I
- ACE
- angiotensin II
- aldosterone
Three factors that stimulate renal renin secretion are:
- decreased blood pressure
- decreased sodium delivery to the macula densa
- increased sympathetic tone
Key physiological effects of angiotensin II include:
- constriction of the glomerular efferent arteriole
- increased ADH secretion
- increased Na+/H+ exchanger activity
- stimulation of thirst
- stimulation of aldosterone secretion
Sites of action of RAAS drugs (see diagram):
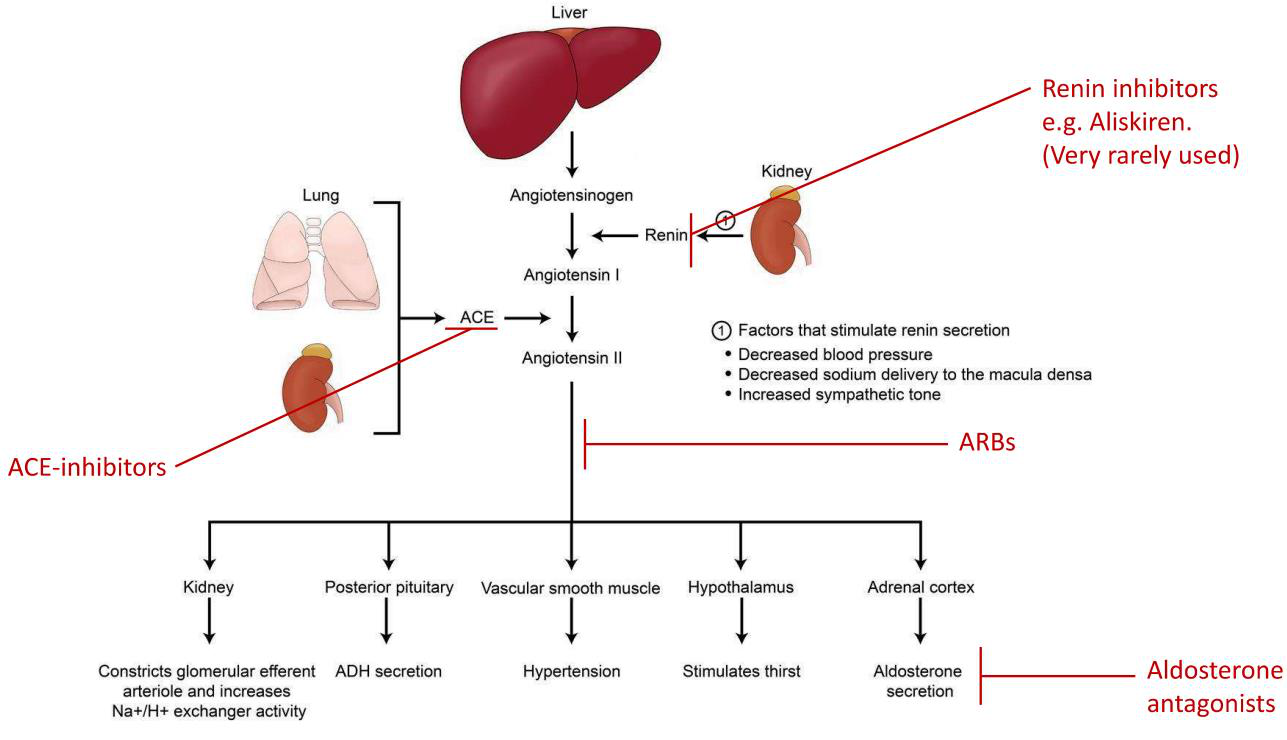
- Renin inhibitors act on renin (blocking formation of angiotensin I)
- ACE inhibitors block ACE (preventing conversion of angiotensin I to II)
- ARBs block the angiotensin II receptor
ACE inhibitors block angiotensin-converting enzyme (ACE), preventing conversion of Angiotensin I to Angiotensin II.
Blocking formation of Angiotensin II reduces a potent vasoconstrictor effect and decreases aldosterone stimulation, leading to lowering of blood pressure.
Before and during ACE inhibitor treatment check CrCl and U&Es at baseline and regularly, including 7-14 days after initiation, after dose increases and if side effects occur.
ACE inhibitors can cause acute kidney injury (AKI), so reduce dose or avoid if CrCl < 30 ml/min.
ACE inhibitors may cause rapid blood pressure reduction; the first dose is often given at bedtime to reduce symptomatic hypotension.
Initiate ACE inhibitors at a low dose and titrate up according to response and tolerance, for example every 2 to 4 weeks.
Common ACE inhibitor examples include ramipril, enalapril and lisinopril; generic drug names typically end with "-pril".
Contraindications to ACE‑inhibitors include: - angioedema - hypersensitivity - pregnancy - renal artery stenosis - concomitant treatment with aliskiren in patients with eGFR < 60 ml/min and DM
Cautions when prescribing ACE‑inhibitors include patients with: - aortic or mitral valve stenosis - hypertrophic cardiomyopathy - concomitant diuretics - Black African or African‑Caribbean origin (may respond less well) - history of anaphylactoid reactions and elderly
Common adverse drug reactions of ACE‑inhibitors include: - hypotension - hyperkalaemia - hyponatraemia
ACE‑inhibitor–related dry cough is due to accumulation of bradykinin.
Angioedema with ACE‑inhibitors is more common in patients of Black African or African‑Caribbean origin and can be delayed.
Drug interactions increasing risk of renal impairment with ACE‑inhibitors include aliskiren and NSAIDs.
Concurrent use of ACE‑inhibitors with potassium‑sparing diuretics increases the risk of hyperkalaemia.
Angiotensin receptor blockers (ARBs) exert their effect by blocking the action of Angiotensin II at the Angiotensin II receptors.
ARBs are used as an alternative to ACE-Inhibitors and have similar properties to ACE-Inhibitors.
Compared with ACE-Inhibitors, ARBs are less likely to cause dry cough and less likely to cause angioedema.
Common examples of ARBs include: - losartan - irbesartan - candesartan
Many ARB drug names share the suffix -artan.
The provided ARB notes state that the list is not exhaustive and advise to see the BNF for full details.
Aldosterone antagonists act by binding to aldosterone receptors at the distal segment of the distal tubule.
Aldosterone antagonists are also known as mineralocorticoid receptor antagonists.
Important adverse effects of aldosterone antagonists include hyperkalaemia, renal impairment, and gynaecomastia.
If a patient develops hyperkalaemia while on an aldosterone antagonist, the drug should be discontinued.
Monitoring for patients on aldosterone antagonists should include CrCl and U&Es (K+).
Aldosterone antagonists can cause acute kidney injury (AKI), so use with care in the elderly.
Examples of aldosterone antagonists include spironolactone and eplerenone.
Renin inhibitors act by blocking renin, which prevents conversion of angiotensinogen to angiotensin I.
An example of a renin inhibitor is aliskiren.
Renin inhibitors have limited use (rare), with notable trials/further reading including Parving et al., 2012 and the ALTITUDE trial.
Avoid combining renin inhibitors with an ACE inhibitor or ARB in patients who have eGFR < 60 ml/min and diabetes mellitus.
Calcium channel blockers (CCBs) act by blocking calcium channels in the peripheral vessels and/or the heart.
Non-dihydropyridine CCBs are rate-limiting and primarily affect the heart by reducing heart rate and cardiac output through inhibition of AV nodal conduction.
Examples: diltiazem and verapamil.
Verapamil (and diltiazem in most cases) should NOT be used in combination with a beta-blocker because of the risk of reduced cardiac output, heart failure and asystole.
Dihydropyridine CCBs reduce blood pressure by causing vascular smooth muscle relaxation, which lowers total peripheral resistance.
Examples: amlodipine, nifedipine and felodipine.
For diltiazem and nifedipine preparations: long-acting preparations are preferred; clinicians should prescribe by brand and dispense by brand.
Typical dosing frequencies for prolonged-release diltiazem preparations: - ADIZEM-SR: twice daily - ADIZEM-XL: once daily
Contraindications to calcium channel blockers include: - cardiogenic shock - unstable angina - significant aortic stenosis
Patient groups requiring caution with calcium channel blockers: - elderly - hepatic impairment
Common adverse effects of calcium channel blockers include: - constipation - headache - flushing - palpitations - dizziness - postural hypotension - ankle oedema and swelling
A specific adverse effect associated with calcium channel blockers is gingival hyperplasia.
Drug interaction: grapefruit increases exposure to calcium channel blockers and should be avoided.
Drug interaction: calcium channel blockers can increase exposure to statins; check statin dose adjustments.
Drug interaction: enzyme inducers (e.g. carbamazepine) decrease exposure to calcium channel blockers; check effects.
Thiazide-like diuretics target the sodium-chloride symporter in the distal convoluted tubule.
At lower doses thiazide-like diuretics produce more vasodilation than diuresis, with the diuretic effect becoming more apparent at higher doses.
Before and regularly during treatment with thiazide-like diuretics check CrCl and U&Es (urea and electrolytes).
Thiazide-like diuretics can cause acute kidney injury (AKI) and should be avoided if CrCl < 30 ml/min due to ineffectiveness.
Because thiazide-like diuretics may cause diuresis, patients are advised to take the dose in the morning.
Thiazide-like diuretics are described as "Low-ceiling diuretics" and require care in the elderly.
Examples of thiazide-like diuretics include indapamide and chlortalidone.
The graph comparing loop and thiazide diuretic dose–response shows thiazides reach a lower maximal diuretic response at increasing doses; see illustration: 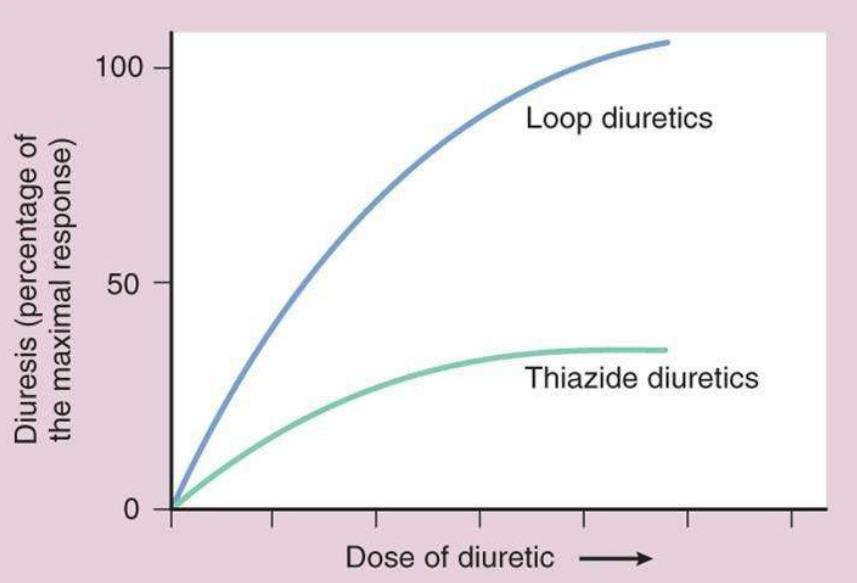
Contraindications for thiazide-like diuretics include: - Addison's disease - severe renal or hepatic impairment - refractory hypokalaemia, hyponatraemia, hypercalcaemia and symptomatic hyperuricaemia
Cautions when prescribing thiazide-like diuretics: - Diabetes - gout - systemic lupus erythematous - These conditions carry a risk of exacerbation.
Common adverse drug reactions of thiazide-like diuretics include: - Hypokalaemia - hyponatraemia - hypercalcaemia - hyperglycaemia - hyperuricaemia
Other adverse effects of thiazide-like diuretics can include: - Postural hypotension, dizziness/light-headedness - Impotence
Reported drug interactions with thiazide-like diuretics include: - NSAIDs which increase the risk of renal impairment (nephrotoxicity) - Lithium - "Torsade de pointes"
The provided profile of thiazide-like diuretics is not exhaustive and advises to see BNF for full details.
When initiating antihypertensive treatment, recheck blood pressure every 4 weeks.
For calcium channel blockers (CCB) monitoring: No specific blood tests are required unless there is a suspected medical problem or side effects.
Before starting ACE-inhibitors, ARBs, or thiazide-like diuretics, check CrCl and U&Es at baseline and then regularly during treatment.
For ACE-inhibitor/ARB/thiazide monitoring schedule: check CrCl and U&Es 1-2 weeks after initiation, after dose increases, if side effects are present, and then annually.
Offer ACE-Inhibitor or ARB treatment if the patient: - has type 2 diabetes mellitus (T2 DM) regardless of age or family origin - is < 55 years old and not of Black African or African-Caribbean origin
Offer calcium channel blocker (CCB) treatment if the patient: - is ≥ 55 years and does not have T2 DM - is of Black African or African-Caribbean origin and does not have T2 DM (any age)
Offer an ARB when: - an ACE-Inhibitor is not tolerated (e.g., due to cough) - it is preferred over an ACE-Inhibitor for adults of Black African or African-Caribbean origin
Offer a thiazide-like diuretic if: - a CCB is not tolerated (e.g., due to oedema) - there is evidence of heart failure
Do not combine an ACE-Inhibitor with an ARB.
If starting or changing diuretic treatment, offer a thiazide-like diuretic (e.g., indapamide) in preference to a conventional thiazide diuretic (e.g., bendroflumethiazide or hydrochlorothiazide).
If a patient is already on a conventional thiazide diuretic and BP is stable and well-controlled, continue current treatment (no need to change to a thiazide-like diuretic).
Before considering the next treatment step, check the patient is taking their medicine as prescribed and support adherence.
Before escalating antihypertensive treatment, review medicines to ensure they are being taken at the optimal tolerated doses and discuss adherence.
If blood pressure is not controlled, offer a combination of: - an ACE-Inhibitor or ARB - a calcium channel blocker (CCB) - a thiazide-like diuretic
Resistant hypertension is defined as blood pressure uncontrolled on optimal tolerated doses of an ACE-Inhibitor or ARB + a CCB + a thiazide-like diuretic.
Patients requiring stage four treatment have resistant hypertension.
Before further treatment for resistant hypertension, confirm and assess by: - Confirm elevated BP with ABPM or HBPM - Assess for postural hypotension - Discuss adherence
For confirmed resistant hypertension, consider seeking specialist advice or adding a fourth antihypertensive drug.
Consider low-dose spironolactone if blood potassium level is ≤ 4.5 mmol/l.
Exercise caution when using spironolactone if there is reduced CrCl because of an increased risk of hyperkalaemia.
When adding further diuretic therapy, monitor BP, Na+, K+ and CrCl within 1 month of initiation and repeat regularly as needed.
If blood potassium level is > 4.5 mmol/l, consider adding an alpha-blocker or beta-blocker.
If blood pressure remains uncontrolled on optimal tolerated doses of four antihypertensive drugs, seek specialist advice.
When assessing hypertension: - Monitor blood pressure - Beware of white‑coat effect and masked hypertension
(See illustration on answer side:  )
)
Essential components of patient support for hypertension include: - Provide training - Provide advice - Provide support
Topics to discuss with a patient who has or may have hypertension: - Lifestyle - Symptoms - Medication
When prescribing antihypertensives, consider offering drugs taken once a day and non-proprietary drugs where appropriate, and minimise costs.
How should isolated systolic hypertension be treated? Treat isolated systolic hypertension the same as systolic and diastolic hypertension.
For choosing antihypertensive treatment in type 1 diabetes, refer to NICE's guideline on type 1 diabetes.
For choosing antihypertensive treatment in chronic kidney disease (CKD), refer to NICE's guideline on chronic kidney disease.
For patients with cardiovascular disease (CVD), follow the recommendations for the disease-specific indications in the NICE guideline for that condition.
Relevant NICE recommendations for antihypertensive management include: - drug therapy for secondary prevention in acute coronary syndromes - treatment after stabilisation in acute heart failure - treating heart failure with reduced ejection fraction - drugs for secondary prevention in stable angina - blood pressure management in type 1 diabetes in adults
If blood pressure remains uncontrolled, offer antihypertensive treatment in line with the recommendations in NICE's guideline on hypertension in adults.
For women of childbearing potential with diagnosed hypertension, offer antihypertensive treatment in line with NICE's guideline on hypertension in adults.
For women who are considering pregnancy, pregnant, or breastfeeding, manage hypertension according to NICE's recommendations on chronic hypertension in pregnancy and antihypertensive treatment while breastfeeding.
ACE inhibitors and ARBs should not be used in pregnant or breastfeeding women or women planning pregnancy unless absolutely necessary, in which case discuss potential risks and benefits.
Follow the MHRA safety advice on ACE inhibitors and angiotensin II receptor antagonists regarding not for use in pregnancy, recommendations for breastfeeding use, and clarification on breastfeeding.
First-line antihypertensive in pregnancy:
- Labetalol
Second-line antihypertensive in pregnancy:
- Nifedipine
Notes: Unlicensed; some brands were specifically contraindicated during pregnancy by the manufacturer in its SmPC (check individual SmPC).
Third-line antihypertensive in pregnancy:
- Methyldopa (Unlicenced)
Choice of antihypertensive in pregnancy should be based on:
- any pre-existing treatment
- side-effect profiles
- risks (including foetal effects)
- woman's preference
Target blood pressure in pregnancy is ≤ 135/85 mmHg.
For breastfeeding women, one recommended ACE inhibitor is enalapril; when prescribing, monitor maternal renal function and serum potassium.
Calcium-channel blockers recommended in breastfeeding include nifedipine and amlodipine; amlodipine is preferred if the woman has previously used it successfully to control blood pressure.
For women of Black African or African-Caribbean origin, consider using nifedipine/amlodipine for blood pressure control while breastfeeding.
If blood pressure is not controlled with a single medicine in breastfeeding women, use combination treatment with enalapril and/or nifedipine/amlodipine.
Use atenolol or labetalol in breastfeeding women if combination treatment is not tolerated or ineffective; you may add one or swap an existing medicine for atenolol/labetalol.
Severe hypertension in pregnancy is defined as blood pressure ≥ 160/110 mmHg.
Severe hypertension in pregnancy requires critical care monitoring and management.
Antihypertensive options listed for severe pregnancy hypertension include: - Labetalol (PO/IV) - Nifedipine (PO) - Hydralazine (IV)
At time of publication, some brands of nifedipine were specifically contraindicated during pregnancy by the manufacturer in its SmPC, so refer to the individual SmPC for each preparation.
A hypertensive emergency is severe hypertension defined as ≥ 180/120 mmHg accompanied by target organ damage.
Recommended acute BP reduction in a hypertensive emergency is to lower mean arterial pressure by 20-25% over a few hours (e.g. 2 hours).
IV antihypertensive options for hypertensive emergency include: - labetalol - nicardipine - hydralazine - nitroprusside - glyceryl trinitrate
A hypertensive urgency is severe hypertension defined as ≥ 180/120 mmHg without target organ damage.
Management of hypertensive urgency aims to reduce BP gradually over several hours (e.g. 24 hours), typically using oral agents.
Oral antihypertensive options for hypertensive urgency include: - labetalol - atenolol - long-acting nifedipine - amlodipine
Key counselling actions during consultations include: - discuss and check adherence - provide appropriate counselling and advice
Benefits of counselling to communicate include encouraging: - lifestyle changes - taking antihypertensives - ensuring adherence
A study found that 4 out of 10 patients with CVD would be willing to accept some degree of risk of immediate death rather than having to take a daily pill.
Key counselling questions to cover for prescribed medicines include: - How much to take? - How often to take? - When to take? - What to monitor and follow-up? - How to minimise risk of adverse drug reactions? - How to minimise risk of interactions?
Flashcards in this deck (227)
-
Hypertension in adults is defined as a systolic blood pressure of ≥ 140 mmHg or a diastolic blood pressure of ≥ 90 mmHg.
hypertension definition -
Primary hypertension is described as hypertension that is chiefly of unknown cause or attributable to a pre-existing condition.
hypertension etiology -
Chronic hypertension typically results in thickening and inelasticity of arterial walls and hypertrophy of the left ventricle.
pathology cardiology -
Hypertension is a risk factor for major organ diseases including cerebrovascular disease, cardiovascular disease, kidney disease, and eye disease.
complications risk -
Blood pressure measurement is a clinical procedure; an example image of a clinician measuring BP is shown as supplementary material on the answer side.
What common clinical tool is used to measure arterial blood pressure?
measurement clinical -
The term 'abnormally high arterial blood pressure' refers to sustained elevations in systolic and/or diastolic pressure above defined adult thresholds (e.g., ≥ 140/90 mmHg).
definition terminology -
Blood pressure (BP) is the pressure exerted on the walls of the blood vessels.
hypertension physiology bloodpressure -
Systolic BP: - the maximum blood pressure exerted by the blood against the artery walls - Corresponds to contraction of the ventricles (systole)
hypertension physiology systolic -
Diastolic BP: - the minimum pressure in the main arteries - Corresponds to relaxation of the ventricles (diastole)
hypertension physiology diastolic -
Blood pressure equals cardiac output × systemic vascular resistance.
hypertension physiology bp -
Cardiac factors that influence blood pressure include: - heart rate - contractibility
cardiac physiology bp -
Drugs listed that act on cardiac factors include: - beta blockers - calcium channel blockers - centrally acting adrenergics
drugs cardiac antihypertensive -
Circulating volume influences BP via: - salt - aldosterone
volume physiology bp -
Drugs affecting circulating volume listed are: - ACE inhibitors - diuretics
drugs raas antihypertensive -
Examples of vasodilator or related drug types given include: - vasodilators - prostaglandins - ACE inhibitors - calcium channel blockers - angiotensin II blockers
vasodilation drugs antihypertensive -
Peripheral sympathetic receptor types and related agents: - Alpha: alpha1 blockers - CNS: centrally acting adrenergics (alpha2) - Beta: beta blockers
autonomic receptors drugs -
Name three cardiac factors that influence blood pressure: - heart rate - contractibility - cardiac output (derived)
Illustration:
hypertension illustration bp -
A common blood pressure (BP) diagnostic cutoff is approximately 140/90 mmHg and worldwide prevalence of hypertension is about 30%.
hypertension epidemiology -
Primary (essential) hypertension is characterized by no identifiable cause and accounts for 90-95% of hypertension cases.
hypertension primary -
Secondary hypertension has an identifiable known cause and represents 5-10% of hypertension cases.
hypertension secondary -
Major categories of causes for secondary hypertension include: - renal diseases - endocrine diseases - vascular causes - drugs
hypertension causes -
Endocrine causes of secondary hypertension listed include: - steroid excess (hyperaldosteronism, Cushing's) - growth hormone excess (acromegaly) - catecholamine excess (phaeochromocytoma) - pre-eclampsia
hypertension endocrine -
Vascular causes of secondary hypertension include: - renal artery stenosis (fibromuscular hyperplasia; renal artery atheroma) - coarctation of the aorta
hypertension vascular -
Drugs that can cause or worsen hypertension include: - sympathomimetic amines - oestrogens (e.g., combined oral contraceptive pills) - ciclosporin - erythropoietin - non-steroidal anti-inflammatory drugs - steroids
hypertension drugs media -
Most cases of hypertension are asymptomatic.
hypertension symptoms -
Severe hypertension may present with: - headache - visual disturbances - evidence of target organ damage
hypertension severe symptoms -
Risk of stroke/CHD increases by 35-40% with every 5 mmHg increase in blood pressure.
stroke cardiology hypertension -
Risk of ocular complications (e.g., retinopathy) is doubled with every 10 mmHg increase in blood pressure.
ophthalmology hypertension retinopathy -
Risk of cardiovascular disease (CVD) doubles for every 20/10 mmHg rise in blood pressure.
cardiology cvd hypertension -
There is a 25% increased risk of renal failure with every 5 mmHg increase in blood pressure.
nephrology renal hypertension -
People with increased blood pressure have a 6-fold higher risk of heart failure.
heartfailure cardiology hypertension -
Common clinic blood pressure measurement methods include: - Manual (clinic) - Automatic (clinic)
measurement clinic -
Ambulatory blood pressure monitoring (ABPM) protocol: use ABPM for 1 day with a minimum of 14 measurements.
abpm measurement -
Home blood pressure monitoring (HBPM) schedule: measure twice a day for 4-7 days.
hbpm home measurement -
Healthcare professionals performing blood pressure measurement must be adequately trained.
training measurement -
BP devices used for measurement must be validated, maintained and calibrated.
devices measurement -
To standardise the measurement environment ensure the person is: - quiet - seated - arm outstretched, supported and relaxed
environment measurement -
Blood pressure should be measured in both arms using an appropriate cuff size.
technique measurement -
When measuring blood pressure, clinicians should take two measurements.
protocol measurement -
If pulse irregularity is present, take care and measure blood pressure manually.
arrhythmia measurement -
Patients with type 2 diabetes mellitus should have blood pressure measured annually.
diabetes screening -
For suspected secondary causes of hypertension, refer for specialist investigations.
secondary hypertension -
When assessing suspected postural hypotension: first measure blood pressure with the person lying on their back (or seated if lying is inconvenient), then measure again after they have been standing for at least 1 minute.
postural measurement hypertension -
Postural hypotension is defined as a fall in blood pressure on standing of: systolic ≥ 20 mmHg or diastolic ≥ 10 mmHg measured after at least 1 minute standing.
postural definition thresholds -
If the systolic fall is ≥ 20 mmHg or diastolic fall ≥ 10 mmHg after 1 minute standing: consider likely causes (eg review medications), manage appropriately (eg fall prevention), measure subsequent blood pressures with the person standing, and consider specialist referral if symptoms persist.
postural management treatment -
If symptoms suggest postural hypotension but the blood pressure drop is below thresholds and the baseline was taken seated: repeat measurements starting with the person lying on their back.
postural measurement protocol -
Consider referring for specialist assessment if blood pressure measurements do not confirm postural hypotension despite suggestive symptoms.
postural referral assessment -
If clinic blood pressure is ≥ 140/90 mmHg, offer ambulatory blood pressure monitoring (ABPM). An alternative is home blood pressure monitoring (HBPM).
diagnosis hypertension monitoring -
While awaiting confirmation of hypertension, clinicians should: - investigate for target organ damage - undertake a cardiovascular risk assessment using QRISK3
assessment hypertension qrisk3 -
If clinic blood pressure is ≥ 180/120 mmHg, refer for same-day specialist review and assessment if any of the following are present: - suspected phaeochromocytoma - signs of retinal haemorrhage or papilloedema - life-threatening symptoms (e.g., new confusion, chest pain, heart failure, acute kidney injury)
emergency hypertension referral -
Suspected phaeochromocytoma may present with symptoms such as labile or postural hypotension, headache, palpitations, pallor, abdominal pain or diaphoresis.
symptoms phaeochromocytoma hypertension -
If clinic BP is ≥ 180/120 mmHg but there are no signs or symptoms for same-day referral, clinicians should: - carry out investigations for target organ damage as soon as possible
investigation hypertension management -
After investigations for target organ damage: - If damage is identified: consider starting antihypertensive drug treatment immediately without ABPM/HBPM - If no damage is identified: confirm diagnosis by repeating clinic BP within 7 days or consider ABPM/HBPM
treatment hypertension management -
Stage 1 hypertension is defined as: - Clinic BP 140/90 mmHg – 159/99 mmHg (≥ 140/90 mmHg) - ABPM daytime or HBPM average BP 135/85 mmHg – 149/94 mmHg (≥ 135/85 mmHg)
hypertension diagnosis stage1 bp -
Stage 2 hypertension is defined as: - Clinic BP 160/100 mmHg – 180/120 mmHg (≥ 160/100 mmHg) - ABPM daytime or HBPM average BP ≥ 150/95 mmHg
hypertension diagnosis stage2 bp -
Stage 3 (severe) hypertension is defined as: - Clinic BP ≥ 180/120 mmHg
hypertension diagnosis stage3 bp -
For all patients diagnosed with hypertension offer cardiovascular risk assessment (QRISK3).
hypertension assessment qrisk3 -
For all patients diagnosed with hypertension offer a urine sample to measure albumin:creatinine ratio and to test for haematuria.
hypertension urine acr -
For all patients diagnosed with hypertension offer a biochemistry sample to measure: - HbA1C - U&Es - creatinine and eGFR - lipid profile
hypertension bloods biochemistry -
For all patients diagnosed with hypertension offer examination of the fundi to check for the presence of hypertensive retinopathy.
hypertension retina fundi -
For all patients diagnosed with hypertension perform a 12-lead ECG.
hypertension ecg cardiology -
For all patients diagnosed with hypertension discuss cardiovascular risk and discuss different treatment options with the patient.
hypertension communication management -
Weight loss reduces blood pressure by approximately 5-20 mmHg per 10 kg lost.
weight lifestyle -
A healthy diet for BP control is rich in fruit and vegetables, includes low-fat dairy products, and has reduced saturated fats.
diet nutrition -
Recommended daily salt intake to reduce blood pressure is < 6 g NaCl per day.
salt diet -
Regular aerobic physical activity is advised as an exercise measure to lower blood pressure.
exercise lifestyle -
Alcohol guidance: maintain moderate consumption and reduce intake if consumption is excessive.
alcohol lifestyle -
Caffeine guidance: adopt moderate consumption and reduce intake if consumption is excessive.
caffeine lifestyle -
Address cardiovascular risk factors by promoting smoking cessation and managing dyslipidaemia.
risk cardiology -
Effective stress management should be part of blood pressure control and reiterated at all stages of care.
stress lifestyle -
Clinic blood pressure under 140/90 mmHg: check BP at least every 5 years and more often if clinic BP is close to 140/90 mmHg.
hypertension monitoring -
If clinic BP is 140/90 to 179/119 mmHg: offer ABPM (or HBPM if ABPM declined or not tolerated), investigate for target organ damage and assess cardiovascular risk.
hypertension diagnosis abpm -
Average daytime ABPM or HBPM target is under 135/85 mmHg.
hypertension targets abpm -
Clinic BP 135/85 to 149/94 mmHg (stage 1): offer lifestyle advice and consider drug treatment for these groups: - age ≥80 with clinic BP >150/90 - age <80 with target organ damage, CVD, renal disease, diabetes or 10-year CVD risk ≥10% - age <60 with 10-year CVD risk <10% (consider) - age <40 (consider specialist evaluation)
hypertension stage1 treatment -
Clinic BP 150/95 mmHg or more (stage 2): offer lifestyle advice and drug treatment; for age under 40 consider specialist evaluation of secondary causes.
hypertension stage2 treatment -
Clinic BP 180/120 mmHg or more: assess for target organ damage as soon as possible; consider starting drug treatment immediately without ABPM/HBPM if target organ damage is present.
hypertension emergency treatment -
Refer for same-day specialist review if accelerated hypertension with retinal haemorrhage or papilloedema, life-threatening symptoms, or suspected pheochromocytoma.
hypertension referral emergency -
ABPM should be based on average daytime readings, ideally taken spread throughout the day.
abpm monitoring hypertension -
For all stages: offer lifestyle advice throughout, support adherence to treatment and offer annual review when on treatment.
hypertension management lifestyle -
For adults aged < 80 years the BP treatment targets are: - Clinic BP: < 140/90 mmHg - ABPM or HBPM: < 135/85 mmHg
hypertension targets age -
For adults aged ≥ 80 years the BP treatment targets are: - Clinic BP: < 150/90 mmHg - ABPM or HBPM: < 145/85 mmHg
hypertension targets elderly -
Patients with cardiovascular disease (CVD) should use the same blood pressure thresholds and treatment targets as those without CVD.
cvd hypertension targets -
For chronic kidney disease (CKD) the BP target is: - < 140/90 mmHg if ACR < 70 mg/mmol - < 130/80 mmHg if ACR ≥ 70 mg/mmol
ckd targets acr -
For type 1 diabetes (T1 DM): - If < 80 years: < 140/90 mmHg if ACR < 70 mg/mmol; < 130/80 mmHg if ACR ≥ 70 mg/mmol - If ≥ 80 years: < 150/90 mmHg regardless of ACR
t1dm diabetes targets -
For type 2 diabetes (T2 DM) the guidance states: the same blood pressure thresholds and treatment targets are used for patients with and without T2 DM.
t2dm diabetes targets -
When assessing postural hypotension, the BP target should be based on standing BP.
postural hypotension assessment -
In patients with frailty, target organ damage, or multimorbidity the recommendation is to use clinical judgement when setting BP targets.
frailty multimorbidity clinical-judgement -
SIGN 2017 recommends offering antihypertensive drug treatment to adults with T1 or T2 DM if systolic BP is ≥ 140 mmHg and considering treatment even if systolic BP is < 140 mmHg for those at greatest risk, with a suggested target of 130/80 mmHg.
sign2017 diabetes treatment -
For people aged under 80 with hypertension (with or without type 2 diabetes), type 1 diabetes with ACR < 70 mg/mmol, or CKD with ACR < 70 mg/mmol, the clinic blood pressure target is below 140/90.
hypertension targets under80 -
For people aged under 80 with type 1 diabetes with ACR ≥ 70 mg/mmol or CKD with ACR ≥ 70 mg/mmol, the clinic blood pressure target is below 130/80.
hypertension targets under80 -
For people aged 80 and over with hypertension (with or without type 2 diabetes) or type 1 diabetes (any ACR), the clinic blood pressure target is below 150/90.
hypertension targets over80 -
For people aged 80 and over with chronic kidney disease and ACR < 70 mg/mmol the clinic blood pressure target is below 140/90, and with ACR ≥ 70 mg/mmol the target is below 130/80.
hypertension targets over80 ckd -
Antihypertensive treatment can increase life expectancy by up to 5 years compared with individuals with uncontrolled hypertension.
hypertension antihypertensives prognosis -
A reduction of 10 mmHg systolic or 5 mmHg diastolic may lead to these relative risk changes: - 20% reduction in all major cardiovascular events - 10-15% reduction in all-cause mortality - 35% reduction in strokes - 20% reduction in coronary events - 40% reduction in heart failure
hypertension antihypertensives cardiovascular -
Main antihypertensive drug classes include: - Thiazide-like diuretic - Angiotensin Converting Enzyme (ACE) inhibitor - Angiotensin Receptor Blocker (ARB) - Calcium Channel Blocker (CCB)
antihypertensive drugclasses -
ACE inhibitor stands for Angiotensin Converting Enzyme Inhibitor.
ace abbreviation -
ARB stands for Angiotensin Receptor Blocker.
arb abbreviation -
CCB stands for Calcium Channel Blocker.
ccb abbreviation -
A thiazide-like diuretic is listed as a diuretic class among antihypertensive drugs.
diuretic thiazide -
The main sequential components of the Renin-Angiotensin-Aldosterone System (RAAS) are: - Angiotensinogen - Renin - Angiotensin I - ACE - Angiotensin II
raas physiology -
The primary organs producing key RAAS components are: - Liver (angiotensinogen) - Kidney (renin) - Lung (ACE)
raas anatomy -
Factors that stimulate renin secretion include: - Decreased blood pressure - Decreased sodium delivery to the macula densa - Increased sympathetic tone
renal regulation -
Angiotensin II produces the following effects: - Constricts glomerular efferent arteriole - Increases Na+/H+ exchanger activity - Stimulates ADH secretion - Stimulates thirst - Stimulates aldosterone secretion
raas actions -
A systemic consequence associated with increased angiotensin II activity is hypertension.
raas pathology -
Main components of the Renin–Angiotensin–Aldosterone System (RAAS):
- angiotensinogen
- renin
- angiotensin I
- ACE
- angiotensin II
- aldosterone
raas physiology hypertension -
Three factors that stimulate renal renin secretion are:
- decreased blood pressure
- decreased sodium delivery to the macula densa
- increased sympathetic tone
raas kidney physiology -
Key physiological effects of angiotensin II include:
- constriction of the glomerular efferent arteriole
- increased ADH secretion
- increased Na+/H+ exchanger activity
- stimulation of thirst
- stimulation of aldosterone secretion
raas physiology endocrinology -
Sites of action of RAAS drugs (see diagram):
- Renin inhibitors act on renin (blocking formation of angiotensin I)
- ACE inhibitors block ACE (preventing conversion of angiotensin I to II)
- ARBs block the angiotensin II receptor
raas pharmacology hypertension -
ACE inhibitors block angiotensin-converting enzyme (ACE), preventing conversion of Angiotensin I to Angiotensin II.
pharmacology raas -
Blocking formation of Angiotensin II reduces a potent vasoconstrictor effect and decreases aldosterone stimulation, leading to lowering of blood pressure.
physiology bp -
Before and during ACE inhibitor treatment check CrCl and U&Es at baseline and regularly, including 7-14 days after initiation, after dose increases and if side effects occur.
monitoring safety -
ACE inhibitors can cause acute kidney injury (AKI), so reduce dose or avoid if CrCl < 30 ml/min.
renal safety -
ACE inhibitors may cause rapid blood pressure reduction; the first dose is often given at bedtime to reduce symptomatic hypotension.
administration safety -
Initiate ACE inhibitors at a low dose and titrate up according to response and tolerance, for example every 2 to 4 weeks.
dosing titration -
Common ACE inhibitor examples include ramipril, enalapril and lisinopril; generic drug names typically end with "-pril".
drugs examples -
Contraindications to ACE‑inhibitors include: - angioedema - hypersensitivity - pregnancy - renal artery stenosis - concomitant treatment with aliskiren in patients with eGFR < 60 ml/min and DM
pharmacology contraindications ace-inhibitors -
Cautions when prescribing ACE‑inhibitors include patients with: - aortic or mitral valve stenosis - hypertrophic cardiomyopathy - concomitant diuretics - Black African or African‑Caribbean origin (may respond less well) - history of anaphylactoid reactions and elderly
pharmacology cautions ace-inhibitors -
Common adverse drug reactions of ACE‑inhibitors include: - hypotension - hyperkalaemia - hyponatraemia
adverse-effects ace-inhibitors electrolytes -
ACE‑inhibitor–related dry cough is due to accumulation of bradykinin.
adverse-effects ace-inhibitors respiratory -
Angioedema with ACE‑inhibitors is more common in patients of Black African or African‑Caribbean origin and can be delayed.
adverse-effects ace-inhibitors angioedema -
Drug interactions increasing risk of renal impairment with ACE‑inhibitors include aliskiren and NSAIDs.
drug-interactions renal ace-inhibitors -
Concurrent use of ACE‑inhibitors with potassium‑sparing diuretics increases the risk of hyperkalaemia.
drug-interactions electrolytes ace-inhibitors -
Angiotensin receptor blockers (ARBs) exert their effect by blocking the action of Angiotensin II at the Angiotensin II receptors.
pharmacology raas antihypertensive -
ARBs are used as an alternative to ACE-Inhibitors and have similar properties to ACE-Inhibitors.
pharmacology hypertension -
Compared with ACE-Inhibitors, ARBs are less likely to cause dry cough and less likely to cause angioedema.
adverse-effects pharmacology -
Common examples of ARBs include: - losartan - irbesartan - candesartan
drugs pharmacology antihypertensive -
Many ARB drug names share the suffix -artan.
nomenclature pharmacology -
The provided ARB notes state that the list is not exhaustive and advise to see the BNF for full details.
resources guidance -
Aldosterone antagonists act by binding to aldosterone receptors at the distal segment of the distal tubule.
pharmacology raas -
Aldosterone antagonists are also known as mineralocorticoid receptor antagonists.
pharmacology terminology -
Important adverse effects of aldosterone antagonists include hyperkalaemia, renal impairment, and gynaecomastia.
adverse-effects safety -
If a patient develops hyperkalaemia while on an aldosterone antagonist, the drug should be discontinued.
management safety -
Monitoring for patients on aldosterone antagonists should include CrCl and U&Es (K+).
monitoring renal -
Aldosterone antagonists can cause acute kidney injury (AKI), so use with care in the elderly.
safety geriatrics -
Examples of aldosterone antagonists include spironolactone and eplerenone.
examples drugs -
Renin inhibitors act by blocking renin, which prevents conversion of angiotensinogen to angiotensin I.
pharmacology raas -
An example of a renin inhibitor is aliskiren.
drugs renin -
Renin inhibitors have limited use (rare), with notable trials/further reading including Parving et al., 2012 and the ALTITUDE trial.
clinical evidence -
Avoid combining renin inhibitors with an ACE inhibitor or ARB in patients who have eGFR < 60 ml/min and diabetes mellitus.
safety renal -
Calcium channel blockers (CCBs) act by blocking calcium channels in the peripheral vessels and/or the heart.
hypertension pharmacology ccb -
Non-dihydropyridine CCBs are rate-limiting and primarily affect the heart by reducing heart rate and cardiac output through inhibition of AV nodal conduction.
Examples: diltiazem and verapamil.
hypertension pharmacology ccb non-dihydropyridine -
Verapamil (and diltiazem in most cases) should NOT be used in combination with a beta-blocker because of the risk of reduced cardiac output, heart failure and asystole.
hypertension safety drug-interactions -
Dihydropyridine CCBs reduce blood pressure by causing vascular smooth muscle relaxation, which lowers total peripheral resistance.
Examples: amlodipine, nifedipine and felodipine.
hypertension pharmacology ccb dihydropyridine -
For diltiazem and nifedipine preparations: long-acting preparations are preferred; clinicians should prescribe by brand and dispense by brand.
hypertension prescribing formulations -
Typical dosing frequencies for prolonged-release diltiazem preparations: - ADIZEM-SR: twice daily - ADIZEM-XL: once daily
hypertension dosing diltiazem -
Contraindications to calcium channel blockers include: - cardiogenic shock - unstable angina - significant aortic stenosis
pharmacology ccb contraindications -
Patient groups requiring caution with calcium channel blockers: - elderly - hepatic impairment
pharmacology ccb caution -
Common adverse effects of calcium channel blockers include: - constipation - headache - flushing - palpitations - dizziness - postural hypotension - ankle oedema and swelling
pharmacology ccb adverse -
A specific adverse effect associated with calcium channel blockers is gingival hyperplasia.
pharmacology ccb adverse -
Drug interaction: grapefruit increases exposure to calcium channel blockers and should be avoided.
pharmacology ccb interactions -
Drug interaction: calcium channel blockers can increase exposure to statins; check statin dose adjustments.
pharmacology ccb interactions -
Drug interaction: enzyme inducers (e.g. carbamazepine) decrease exposure to calcium channel blockers; check effects.
pharmacology ccb interactions -
Thiazide-like diuretics target the sodium-chloride symporter in the distal convoluted tubule.
pharmacology diuretics -
At lower doses thiazide-like diuretics produce more vasodilation than diuresis, with the diuretic effect becoming more apparent at higher doses.
pharmacology dose-dependence -
Before and regularly during treatment with thiazide-like diuretics check CrCl and U&Es (urea and electrolytes).
monitoring renal -
Thiazide-like diuretics can cause acute kidney injury (AKI) and should be avoided if CrCl < 30 ml/min due to ineffectiveness.
adverse-effects renal -
Because thiazide-like diuretics may cause diuresis, patients are advised to take the dose in the morning.
administration practical -
Thiazide-like diuretics are described as "Low-ceiling diuretics" and require care in the elderly.
classification geriatrics -
Examples of thiazide-like diuretics include indapamide and chlortalidone.
examples drugs -
The graph comparing loop and thiazide diuretic dose–response shows thiazides reach a lower maximal diuretic response at increasing doses; see illustration:
graph pharmacodynamics -
Contraindications for thiazide-like diuretics include: - Addison's disease - severe renal or hepatic impairment - refractory hypokalaemia, hyponatraemia, hypercalcaemia and symptomatic hyperuricaemia
pharmacology diuretics contraindications -
Cautions when prescribing thiazide-like diuretics: - Diabetes - gout - systemic lupus erythematous - These conditions carry a risk of exacerbation.
pharmacology diuretics cautions -
Common adverse drug reactions of thiazide-like diuretics include: - Hypokalaemia - hyponatraemia - hypercalcaemia - hyperglycaemia - hyperuricaemia
pharmacology diuretics adverse-effects -
Other adverse effects of thiazide-like diuretics can include: - Postural hypotension, dizziness/light-headedness - Impotence
pharmacology diuretics adverse-effects -
Reported drug interactions with thiazide-like diuretics include: - NSAIDs which increase the risk of renal impairment (nephrotoxicity) - Lithium - "Torsade de pointes"
pharmacology diuretics interactions -
The provided profile of thiazide-like diuretics is not exhaustive and advises to see BNF for full details.
pharmacology diuretics reference -
When initiating antihypertensive treatment, recheck blood pressure every 4 weeks.
hypertension monitoring -
For calcium channel blockers (CCB) monitoring: No specific blood tests are required unless there is a suspected medical problem or side effects.
ccb monitoring -
Before starting ACE-inhibitors, ARBs, or thiazide-like diuretics, check CrCl and U&Es at baseline and then regularly during treatment.
ace arb diuretic monitoring -
For ACE-inhibitor/ARB/thiazide monitoring schedule: check CrCl and U&Es 1-2 weeks after initiation, after dose increases, if side effects are present, and then annually.
ace arb diuretic schedule -
Offer ACE-Inhibitor or ARB treatment if the patient: - has type 2 diabetes mellitus (T2 DM) regardless of age or family origin - is < 55 years old and not of Black African or African-Caribbean origin
hypertension pharmacology ace_arb -
Offer calcium channel blocker (CCB) treatment if the patient: - is ≥ 55 years and does not have T2 DM - is of Black African or African-Caribbean origin and does not have T2 DM (any age)
hypertension pharmacology ccb -
Offer an ARB when: - an ACE-Inhibitor is not tolerated (e.g., due to cough) - it is preferred over an ACE-Inhibitor for adults of Black African or African-Caribbean origin
hypertension pharmacology arb -
Offer a thiazide-like diuretic if: - a CCB is not tolerated (e.g., due to oedema) - there is evidence of heart failure
hypertension pharmacology diuretics -
Do not combine an ACE-Inhibitor with an ARB.
hypertension safety raas -
If starting or changing diuretic treatment, offer a thiazide-like diuretic (e.g., indapamide) in preference to a conventional thiazide diuretic (e.g., bendroflumethiazide or hydrochlorothiazide).
hypertension diuretics guidelines -
If a patient is already on a conventional thiazide diuretic and BP is stable and well-controlled, continue current treatment (no need to change to a thiazide-like diuretic).
hypertension diuretics management -
Before considering the next treatment step, check the patient is taking their medicine as prescribed and support adherence.
hypertension adherence management -
Before escalating antihypertensive treatment, review medicines to ensure they are being taken at the optimal tolerated doses and discuss adherence.
hypertension treatment adherence -
If blood pressure is not controlled, offer a combination of: - an ACE-Inhibitor or ARB - a calcium channel blocker (CCB) - a thiazide-like diuretic
hypertension pharmacology treatment -
Resistant hypertension is defined as blood pressure uncontrolled on optimal tolerated doses of an ACE-Inhibitor or ARB + a CCB + a thiazide-like diuretic.
hypertension definition management -
Patients requiring stage four treatment have resistant hypertension.
hypertension staging -
Before further treatment for resistant hypertension, confirm and assess by: - Confirm elevated BP with ABPM or HBPM - Assess for postural hypotension - Discuss adherence
hypertension assessment measurement -
For confirmed resistant hypertension, consider seeking specialist advice or adding a fourth antihypertensive drug.
hypertension management specialist -
Consider low-dose spironolactone if blood potassium level is ≤ 4.5 mmol/l.
hypertension pharmacology diuretics -
Exercise caution when using spironolactone if there is reduced CrCl because of an increased risk of hyperkalaemia.
hypertension safety renal -
When adding further diuretic therapy, monitor BP, Na+, K+ and CrCl within 1 month of initiation and repeat regularly as needed.
hypertension monitoring -
If blood potassium level is > 4.5 mmol/l, consider adding an alpha-blocker or beta-blocker.
hypertension pharmacology electrolytes -
If blood pressure remains uncontrolled on optimal tolerated doses of four antihypertensive drugs, seek specialist advice.
hypertension management specialist -
When assessing hypertension: - Monitor blood pressure - Beware of white‑coat effect and masked hypertension
(See illustration on answer side:
)hypertension monitoring -
Essential components of patient support for hypertension include: - Provide training - Provide advice - Provide support
hypertension patientcare -
Topics to discuss with a patient who has or may have hypertension: - Lifestyle - Symptoms - Medication
hypertension communication -
When prescribing antihypertensives, consider offering drugs taken once a day and non-proprietary drugs where appropriate, and minimise costs.
hypertension prescribing cost -
How should isolated systolic hypertension be treated? Treat isolated systolic hypertension the same as systolic and diastolic hypertension.
hypertension classification -
For choosing antihypertensive treatment in type 1 diabetes, refer to NICE's guideline on type 1 diabetes.
diabetes nice -
For choosing antihypertensive treatment in chronic kidney disease (CKD), refer to NICE's guideline on chronic kidney disease.
ckd nice -
For patients with cardiovascular disease (CVD), follow the recommendations for the disease-specific indications in the NICE guideline for that condition.
cvd nice management -
Relevant NICE recommendations for antihypertensive management include: - drug therapy for secondary prevention in acute coronary syndromes - treatment after stabilisation in acute heart failure - treating heart failure with reduced ejection fraction - drugs for secondary prevention in stable angina - blood pressure management in type 1 diabetes in adults
nice cardiology secondary_prevention -
If blood pressure remains uncontrolled, offer antihypertensive treatment in line with the recommendations in NICE's guideline on hypertension in adults.
hypertension nice treatment -
For women of childbearing potential with diagnosed hypertension, offer antihypertensive treatment in line with NICE's guideline on hypertension in adults.
hypertension guidelines nice -
For women who are considering pregnancy, pregnant, or breastfeeding, manage hypertension according to NICE's recommendations on chronic hypertension in pregnancy and antihypertensive treatment while breastfeeding.
hypertension pregnancy breastfeeding nice -
ACE inhibitors and ARBs should not be used in pregnant or breastfeeding women or women planning pregnancy unless absolutely necessary, in which case discuss potential risks and benefits.
acei arbs pregnancy breastfeeding risks -
Follow the MHRA safety advice on ACE inhibitors and angiotensin II receptor antagonists regarding not for use in pregnancy, recommendations for breastfeeding use, and clarification on breastfeeding.
mhra acei arbs breastfeeding pregnancy -
First-line antihypertensive in pregnancy:
- Labetalol
pregnancy antihypertensive labetalol -
Second-line antihypertensive in pregnancy:
- Nifedipine
Notes: Unlicensed; some brands were specifically contraindicated during pregnancy by the manufacturer in its SmPC (check individual SmPC).
pregnancy antihypertensive nifedipine -
Third-line antihypertensive in pregnancy:
- Methyldopa (Unlicenced)
pregnancy antihypertensive methyldopa -
Choice of antihypertensive in pregnancy should be based on:
- any pre-existing treatment
- side-effect profiles
- risks (including foetal effects)
- woman's preference
pregnancy treatment choice -
Target blood pressure in pregnancy is ≤ 135/85 mmHg.
pregnancy targets bloodpressure -
For breastfeeding women, one recommended ACE inhibitor is enalapril; when prescribing, monitor maternal renal function and serum potassium.
antihypertensives breastfeeding enalapril -
Calcium-channel blockers recommended in breastfeeding include nifedipine and amlodipine; amlodipine is preferred if the woman has previously used it successfully to control blood pressure.
antihypertensives breastfeeding calciumchannel -
For women of Black African or African-Caribbean origin, consider using nifedipine/amlodipine for blood pressure control while breastfeeding.
antihypertensives ethnicity breastfeeding -
If blood pressure is not controlled with a single medicine in breastfeeding women, use combination treatment with enalapril and/or nifedipine/amlodipine.
antihypertensives combination breastfeeding -
Use atenolol or labetalol in breastfeeding women if combination treatment is not tolerated or ineffective; you may add one or swap an existing medicine for atenolol/labetalol.
antihypertensives atenolol labetalol breastfeeding -
Severe hypertension in pregnancy is defined as blood pressure ≥ 160/110 mmHg.
obstetrics hypertension pregnancy definition -
Severe hypertension in pregnancy requires critical care monitoring and management.
obstetrics management criticalcare -
Antihypertensive options listed for severe pregnancy hypertension include: - Labetalol (PO/IV) - Nifedipine (PO) - Hydralazine (IV)
obstetrics drugs pharmacology -
At time of publication, some brands of nifedipine were specifically contraindicated during pregnancy by the manufacturer in its SmPC, so refer to the individual SmPC for each preparation.
obstetrics safety nifedipine -
A hypertensive emergency is severe hypertension defined as ≥ 180/120 mmHg accompanied by target organ damage.
hypertension emergency definition -
Recommended acute BP reduction in a hypertensive emergency is to lower mean arterial pressure by 20-25% over a few hours (e.g. 2 hours).
hypertension management targets -
IV antihypertensive options for hypertensive emergency include: - labetalol - nicardipine - hydralazine - nitroprusside - glyceryl trinitrate
hypertension medications emergency -
A hypertensive urgency is severe hypertension defined as ≥ 180/120 mmHg without target organ damage.
hypertension urgency definition -
Management of hypertensive urgency aims to reduce BP gradually over several hours (e.g. 24 hours), typically using oral agents.
hypertension management urgency -
Oral antihypertensive options for hypertensive urgency include: - labetalol - atenolol - long-acting nifedipine - amlodipine
hypertension medications urgency -
Key counselling actions during consultations include: - discuss and check adherence - provide appropriate counselling and advice
counselling adherence -
Benefits of counselling to communicate include encouraging: - lifestyle changes - taking antihypertensives - ensuring adherence
benefits hypertension -
A study found that 4 out of 10 patients with CVD would be willing to accept some degree of risk of immediate death rather than having to take a daily pill.
study patient-preferences -
Key counselling questions to cover for prescribed medicines include: - How much to take? - How often to take? - When to take? - What to monitor and follow-up? - How to minimise risk of adverse drug reactions? - How to minimise risk of interactions?
counselling medication
Overview
- Hypertension (HTN): persistent, abnormally high arterial blood pressure; major risk factor for stroke, heart disease, kidney disease and eye disease.
- Diagnostic clinic threshold: clinic BP of \(\ge 140/90\ \text{mmHg}\).
Key definition and physiology
- Blood pressure (BP): pressure blood exerts on vessel walls; varies with cardiac cycle.
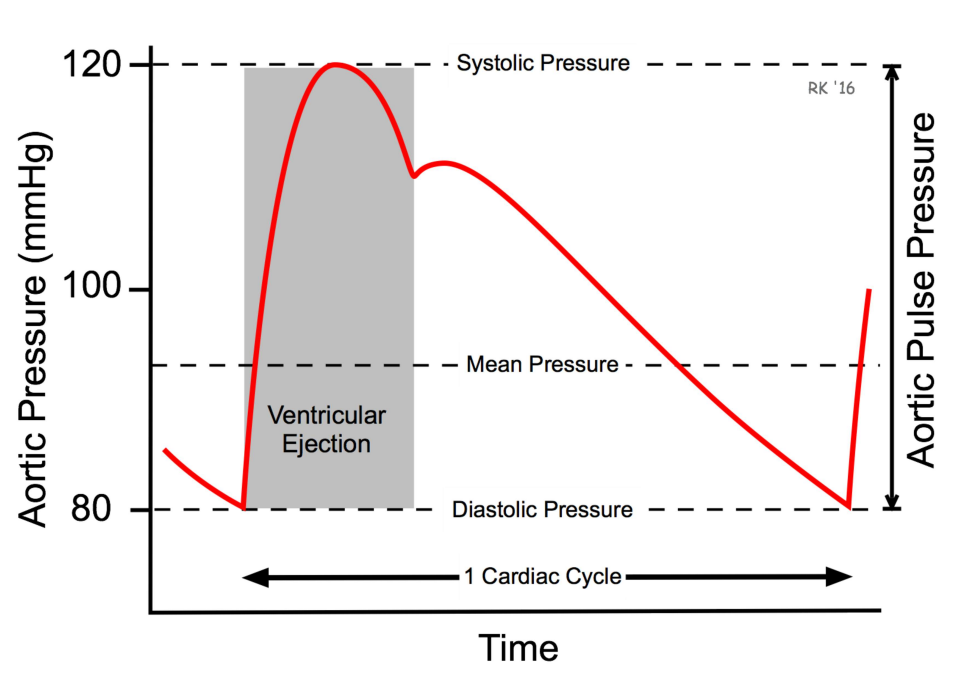 Alt: Blood pressure waveform showing systolic and diastolic pressures
Alt: Blood pressure waveform showing systolic and diastolic pressures
- Systolic BP: peak during ventricular systole.
- Diastolic BP: minimum during ventricular diastole.
- Fundamental relation: \(\(BP = CO \times SVR\)\) where \(CO\) = cardiac output and \(SVR\) = systemic vascular resistance.
BP control — major determinants
- Cardiac factors: heart rate, contractility (affect CO).
- Blood volume and hormones: salt, aldosterone, ADH (affect circulating volume).
- Vascular tone: sympathetic activity, vasodilators/vasoconstrictors (affect SVR).
Alt: Flowchart: BP = CO × SVR and contributing factors
Causes of hypertension
- Primary (essential) HTN: 90–95% — no single identifiable cause.
- Secondary HTN: 5–10% — identifiable causes: renal disease, endocrine disorders (primary hyperaldosteronism, Cushing's, pheochromocytoma), renal artery stenosis, drugs (NSAIDs, corticosteroids, OCPs, erythropoietin), coarctation.
Alt: Causes of hypertension: primary and secondary causes
Clinical features
- Most patients are asymptomatic.
- Symptoms in severe HTN: headache, visual disturbances, signs of target-organ damage (neurological deficit, chest pain, acute kidney injury).
Risks and benefits
- Small BP reductions yield large benefits: e.g. a 10 mmHg drop in SBP reduces major cardiovascular events by ~20% and strokes by ~35%.
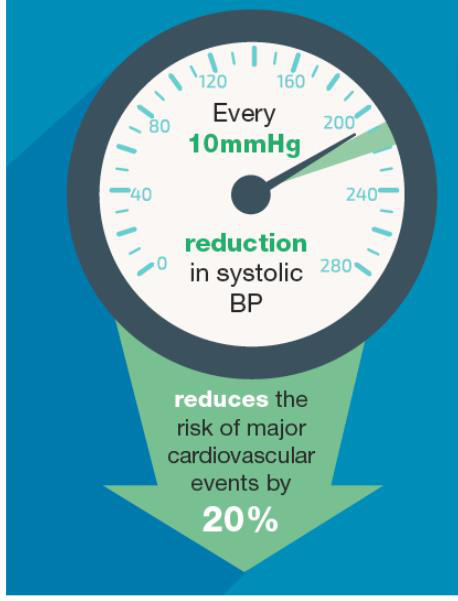 Alt: Infographic showing reduced CVD risk with BP reduction
Alt: Infographic showing reduced CVD risk with BP reduction
Measurement of BP — practical points
- Use validated, calibrated devices; staff must be trained.
- Standardise: person rested, seated, arm supported, correct cuff size, measure in both arms initially.
- Take at least two measurements and consider manual measurement if pulse irregular.
- Measurement methods: clinic (manual/automatic), home BP monitoring (HBPM), ambulatory BP monitoring (ABPM — daytime average from multiple readings).
Alt: Doctor measuring blood pressure with manual cuff
Postural hypotension
- Check lying and after standing ≥1 minute if symptomatic or high risk (elderly, T2DM).
- Significant drop: systolic fall ≥ 20 mmHg or diastolic fall ≥ 10 mmHg.
Diagnosis and staging
- If clinic BP \(\ge 140/90\ \text{mmHg}\), confirm with ABPM (preferred) or HBPM.
- Urgent referral if clinic BP \(\ge 180/120\ \text{mmHg}\) with life‑threatening features or signs of end‑organ damage.
Staging (clinic and out-of-office averages): - Stage 1: Clinic \(140/90\)–\(159/99\ \text{mmHg}\); ABPM/HBPM daytime average \(\ge 135/85\ \text{mmHg}\). - Stage 2: Clinic \(\ge 160/100\ \text{mmHg}\); ABPM/HBPM daytime average \(\ge 150/95\ \text{mmHg}\). - Stage 3 / Severe: Clinic \(\ge 180/120\ \text{mmHg}\).
Alt: Flowchart: hypertension diagnosis and initial management
Assessment after diagnosis
- Evaluate for target-organ damage: urine ACR, haematuria, renal function (U&Es, eGFR), HbA1c, lipids, 12‑lead ECG, fundoscopy.
- Perform cardiovascular risk assessment (QRISK3) and discuss risks and treatment options with the patient.
Non‑pharmacological management (always important)
- Weight loss (approx. 5–20 mmHg reduction per 10 kg lost), DASH-like diet, reduce salt (<6 g/day), regular aerobic exercise, limit alcohol and caffeine, stop smoking, stress management.
BP treatment targets
- Adults < 80 years: clinic target \(<140/90\ \text{mmHg}\); ABPM/HBPM target \(<135/85\ \text{mmHg}\).
- Adults ≥ 80 years: clinic target \(<150/90\ \text{mmHg}\); ABPM/HBPM target \(<145/85\ \text{mmHg}\).
- Chronic kidney disease or albuminuria: lower targets may apply (e.g. clinic \(<130/80\ \text{mmHg}\) if ACR ≥ 70 mg/mmol).
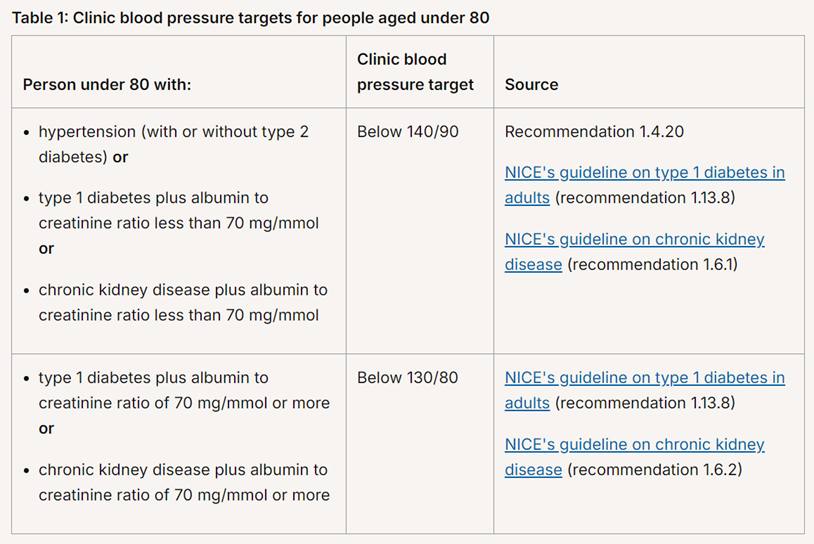 Alt: Clinic blood pressure targets for people under 80 years
Alt: Clinic blood pressure targets for people under 80 years
Pharmacological classes — quick reference
- ACE inhibitors ("-pril"): inhibit conversion of Ang I → Ang II; reduce vasoconstriction and aldosterone. Monitor renal function and K+ at baseline and within 1–2 weeks. Avoid in pregnancy and history of angioedema.
- ARBs ("-artan"): block Ang II receptors; alternative to ACEi (less cough, lower angioedema risk).
- Calcium channel blockers (CCBs): dihydropyridines (amlodipine, nifedipine) vasodilate; non‑dihydropyridines (verapamil, diltiazem) slow AV conduction — avoid combining with beta‑blockers.
- Thiazide‑like diuretics (indapamide, chlortalidone): reduce BP via vasodilation at low doses and diuresis at higher doses; monitor electrolytes and renal function.
- Aldosterone antagonists (spironolactone, eplerenone): useful in resistant HTN; risk of hyperkalaemia and gynaecomastia (spironolactone).
- Renin inhibitors (aliskiren): rarely used; avoid combined use with ACEi/ARB in diabetes with reduced eGFR.
RAAS summary (site of drug actions)
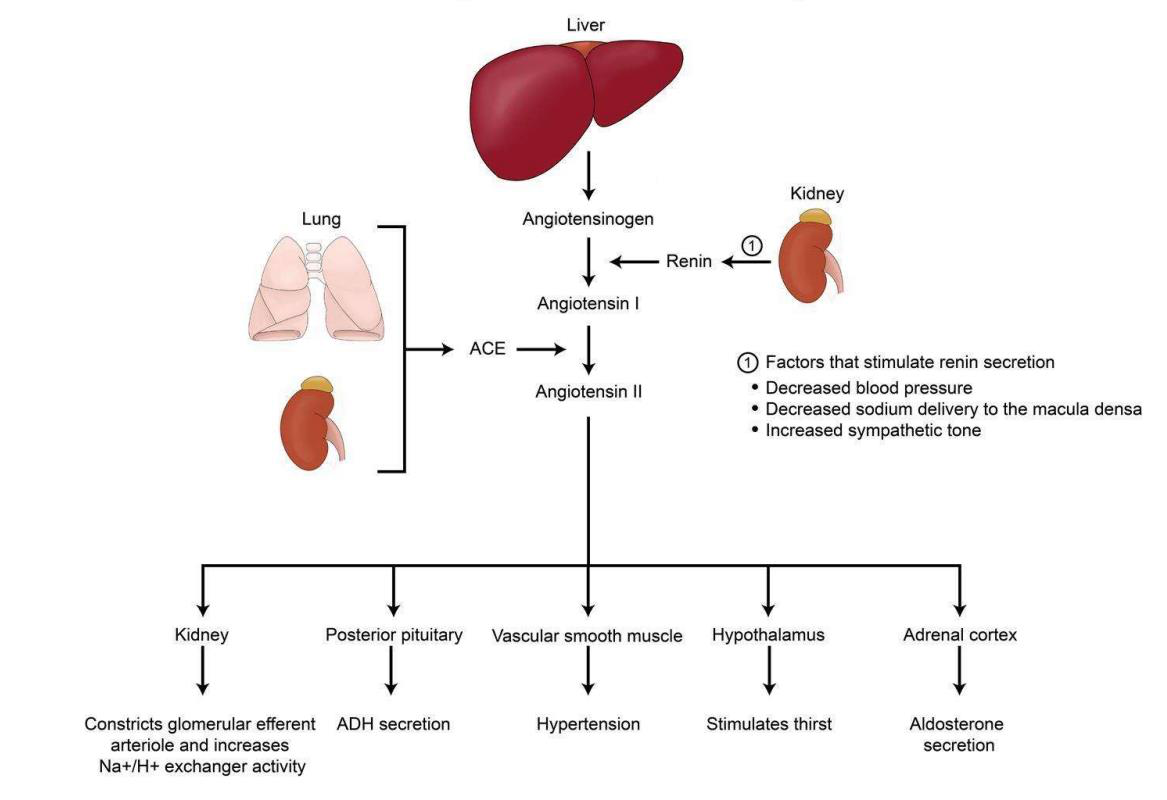 Alt: RAAS cascade showing angiotensinogen → Ang I → Ang II and drug sites
Alt: RAAS cascade showing angiotensinogen → Ang I → Ang II and drug sites
- Renin (kidney) converts angiotensinogen → Ang I; ACE (lung) converts Ang I → Ang II; Ang II causes vasoconstriction and aldosterone release.
- ACE inhibitors, ARBs, renin inhibitors and aldosterone antagonists act at different points to lower BP.
Treatment strategy (NICE condensed)
- Step 1: Choose initial drug by age and ethnicity
- <55 years (non‑Black): ACE‑inhibitor or ARB.
- ≥55 years or Black African/Caribbean: CCB.
- If intolerant to ACEi, use ARB.
- Step 2: If single drug insufficient, combine (ACEi/ARB + CCB or thiazide‑like diuretic).
- Step 3: If not controlled, use triple therapy (ACEi/ARB + CCB + thiazide‑like diuretic).
-
Step 4 (resistant HTN): consider adding low‑dose spironolactone if K+ ≤ 4.5 mmol/L; otherwise consider alpha or beta blocker and seek specialist input.
-
Recheck BP every ~4 weeks when titrating; monitor renal function and electrolytes when using ACEi/ARB, diuretics or aldosterone antagonists.
Hypertensive crises
- Hypertensive emergency: severe HTN (\(\ge 180/120\ \text{mmHg}\)) with target‑organ damage; lower BP by ~20–25% over a few hours with IV agents (labetalol, nicardipine, hydralazine, nitroprusside).
- Hypertensive urgency: severe HTN without organ damage; gradually reduce BP over 24 hours using oral agents (e.g. oral labetalol, long‑acting nifedipine).
Pregnancy and breastfeeding
- Avoid ACE inhibitors and ARBs in pregnancy and breastfeeding unless strictly necessary; discuss risks and alternatives.
- First-line in pregnancy: labetalol; second-line nifedipine (some products unlicensed), third-line methyldopa; aim for BP ≤ 135/85 mmHg in pregnancy.
Monitoring, adherence and counselling
- Annual review of BP and cardiovascular risk; reinforce lifestyle changes and adherence.
- Use once‑daily and generic options where appropriate to improve adherence and reduce cost.
- Educate about side effects, when to seek help (symptoms of hypotension, hyperkalaemia, angioedema) and importance of regular blood tests when on RAAS inhibitors or diuretics.
When to seek specialist input
- Confirmed resistant hypertension on optimal doses of three drugs.
- Suspected secondary causes (e.g. young age, abrupt onset, refractory HTN, severe hypertension in pregnancy).
- Complex comorbidity (CKD with high albuminuria, heart failure requiring specialist care).
Quick reference formulas and thresholds
- BP relation: \(\(BP = CO \times SVR\)\)
- Diagnostic trigger: clinic BP \(\ge 140/90\ \text{mmHg}\) → confirm with ABPM/HBPM.
- Severe threshold: clinic BP \(\ge 180/120\ \text{mmHg}\) (consider urgent referral).
Practical tips for exams/clinics
- Always confirm with out-of-office monitoring before labelling someone hypertensive unless immediate danger signs.
- Record arm used, cuff size, position and whether readings averaged.
- Before stepping up therapy, check adherence, side effects and correct dosing.