Zapisz talię, zanim zniknie
Te fiszki nie są jeszcze zapisane — znikną, gdy wyjdziesz. Załóż darmowe konto, aby je zachować i odblokować wszystko poniżej.
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
What type of structures are visible on a radiograph?
Which condition is not typically visible on a radiograph?
Periodontitis
Alveolar bone loss
Gingivitis
Changes in bone height
What are the three physical changes to bone that may occur during periodontitis?
What are the three components of a complete periodontal assessment?
How does the shape of the interdental septum differ between front and posterior teeth?
What is the normal distance from the CEJ to the alveolar crest in health?
What anatomical landmark dictates the location of the alveolar bone crest?
In a healthy state, where is the alveolar crest typically located relative to the CEJ line?
Why is the interdental septae the primary focus when evaluating periodontitis via radiographs?
What is the relationship between periodontal attachment loss and radiographic bone levels in periodontitis?
What are the two common methods to describe the amount of bone loss in radiographs?
If a tooth is tilted and not fully erupted, the CEJ position relative to an adjacent tooth can lead to the false appearance of what?
Alveolar bone loss
Root resorption
Increased bone density
Apical periodontitis
What are the two primary anatomical landmarks needed to assess bone loss on a radiograph?
What is the periodontitis stage associated with a radiographic bone loss of 15% - 33% in the coronal third?
Stage IV
Stage III
Stage II
Stage I
What is the periodontitis stage associated with less than 15% radiographic bone loss?
Stage III
Stage I
Stage IV
Stage II
What stage of periodontitis corresponds to bone loss extending to the middle to apical third?
If bone loss is measured to be 2 mm below the CEJ, what percentage of bone loss does this represent?
When assessing periodontal status, what clinical attachment loss is associated with 'Moderate' periodontitis severity?
How is the area for bone loss assessment defined on a radiograph?
In a healthy state, how far is the alveolar bone typically positioned relative to the cemento-enamel junction (CEJ)?
When assessing root length for bone loss calculations, why should 2mm be subtracted from the total root length indicated in standard dental tables?
How is horizontal bone loss radiographically defined relative to the cemento-enamel junction (CEJ)?
If the full length of a tooth root is not visible on a bitewing radiograph, what is the standard method for estimating the root length to determine bone loss percentage?
Use a fixed universal root length of 10mm for all teeth.
Refer to tables providing average root lengths for specific teeth.
Estimate the root length by doubling the crown height.
Calculate the root length based solely on the patient's age.
Which of the following describes the healthy distance of the alveolar bone from the CEJ?
0.5mm
5mm
2mm
10mm
What is the characteristic appearance of vertical or angular bone loss on a radiograph?
How is normal lamina dura observed on a dental radiograph?
When a tooth is missing and adjacent teeth have drifted, what might appear to be vertical bone loss but is actually horizontal bone loss?
When the lamina dura is no longer continuous
When there is an irregular V-shape bone defect
When the bone level follows a parallel path to a line drawn through the CEJs
When the alveolar crest is 5mm below the CEJ
Define the relationship between the alveolar bone and the cementoenamel junction (CEJ) in horizontal bone loss.
What is the microscopic structure of the lamina dura?
What radiographic changes to the lamina dura can indicate the early stages of periodontal disease?
Why is the absence of the lamina dura on a radiograph not always a reliable indicator of disease?
What radiographic sign in the lamina dura might indicate successful periodontal therapy?
In a healthy tooth, how does the furcation area appear on a radiograph?
What are the radiographic indicators for early versus advanced furcation involvement?
Why is furcation involvement often easier to identify on lower molars compared to upper molars?
What is a specific radiographic indicator for identifying furcation involvement in the proximal region?
What radiographic finding suggests the need for further clinical testing with a Nabers probe?
How does clinical furcation involvement typically compare to radiographic findings?
How does the healthy periodontal ligament (PDL) space appear on a radiograph?
What changes in the periodontal ligament (PDL) space are indicative of disease?
Besides periodontal disease, what conditions can cause a widening of the periodontal ligament (PDL) space?
What is the recommended method to determine changes in bone height and the progression rate of disease?
When documenting bone loss on a radiograph, why should clinicians use specific quantitative measures instead of subjective descriptors like 'moderate' or 'severe'?
At what age range does crown mineralization typically reach completion?
Based on the provided radiographic case study, what was the estimated bone loss over the 11-year follow-up?
What is the clinical role of radiographic findings in periodontal disease?
Can radiographs replace a thorough assessment of the root surface using an explorer probe?
How sensitive are radiographs at indicating the presence of calculus?
What clinical changes can be observed on radiographs following dental debridement?
What condition suggests a potential violation of the supracrestal attached tissues?
What is a potential clinical consequence of an open or poorly contoured proximal contact?
List three common radiographic signs of periodontal disease.
What aspects of tooth and root morphology can be evaluated via radiographs during periodontitis?
Which of the following is a radiographic sign of periodontal disease?
Root elongation
Increased density of the lamina dura
Decreased root length
Horizontal bone loss
When evaluating restorations on a radiograph, what three clinical issues should be assessed?
What term describes the condition where dental roots appear to fuse together?
How is the root trunk defined in dentistry?
How does the length of the root trunk influence the risk of furcation involvement?
What is the clinical significance of a kink in a tooth root?
What complication might arise when a root is bulbous on the middle third?
What is the main concern when radiographically observing close root proximity between teeth?
Rapid cementum formation
Lack of adequate proximal bone
Increased furcation accessibility
Excessive crown length
What is a potential concern regarding the proximity of periodontal defects in the upper jaw?
Why is it difficult to detect furcation involvement in upper premolars using standard radiographs?
How can endodontic and periodontal diseases interact?
What are two additional pathologies that may be diagnosed alongside common endodontic or periodontal issues?
What radiographic signs are associated with a vertical root fracture?
Why can radiographs be misleading when assessing three-dimensional bone defects?
What is the primary limitation of radiographs regarding current periodontal disease activity?
They provide a continuous, real-time monitoring of disease progression.
They are the gold standard for distinguishing between active and inactive disease phases.
They only show the result of past tissue destruction and do not reveal current activity like bleeding on probing or pus.
They accurately show the internal soft tissue morphology in high detail.
Why must a clinician consider the ALARA principle when choosing to perform a cone beam CT scan?
What is required for a complete periodontal evaluation and accurate defect localization?
At what stage of periodontal disease does evidence of attachment loss typically become obvious on a radiograph?
Which of the following is true about the use of radiographs for monitoring periodontal disease?
They are sufficient on their own for evaluating soft tissue conditions.
They are the most sensitive method for detecting early-stage attachment loss.
They capture the internal morphology of every bone defect.
They provide only a snapshot of the disease state at a specific point in time.
What is the potential discrepancy between the actual alveolar bone crest height and the height observed on radiographs?
How does an OPG (Orthopantomogram) compare to a periapical radiograph regarding the assessment of alveolar bone levels?
OPG is less detailed and lacks the accuracy of periapical radiographs.
OPG provides identical levels of detail as periapical radiographs.
OPG is completely unsuitable for evaluating any bone levels.
OPG is more detailed and accurate than periapical radiographs.
Why are bitewing (BW) radiographs often preferred over periapical (PA) radiographs for evaluating crestal bone height?
What is a major limitation of using bitewing (BW) radiographs to evaluate bone loss?
They cause extreme distortion in all patient cases.
They are only effective for visualizing furcation involvement.
They are unable to visualize bone loss greater than 5mm.
They cannot visualize bone loss of any depth.
What is the primary purpose of employing the cone paralleling technique during dental radiography?
How should a practitioner decide which type of radiograph to take for a periodontal evaluation?
Where is the crest of the interdental bone located relative to the CEJ in a normal radiograph?
What are the common radiographic signs of early periodontal bone changes?
What shape do the radiolucent areas at the crest take during early periodontal changes?
What is the primary radiographic change indicating progression of periodontal disease in the interdental septum?
What bone condition is often visible around tooth 32 in advanced periodontal disease?
Describe the radiographic sequence of periodontal bone changes shown in the series of radiographs. 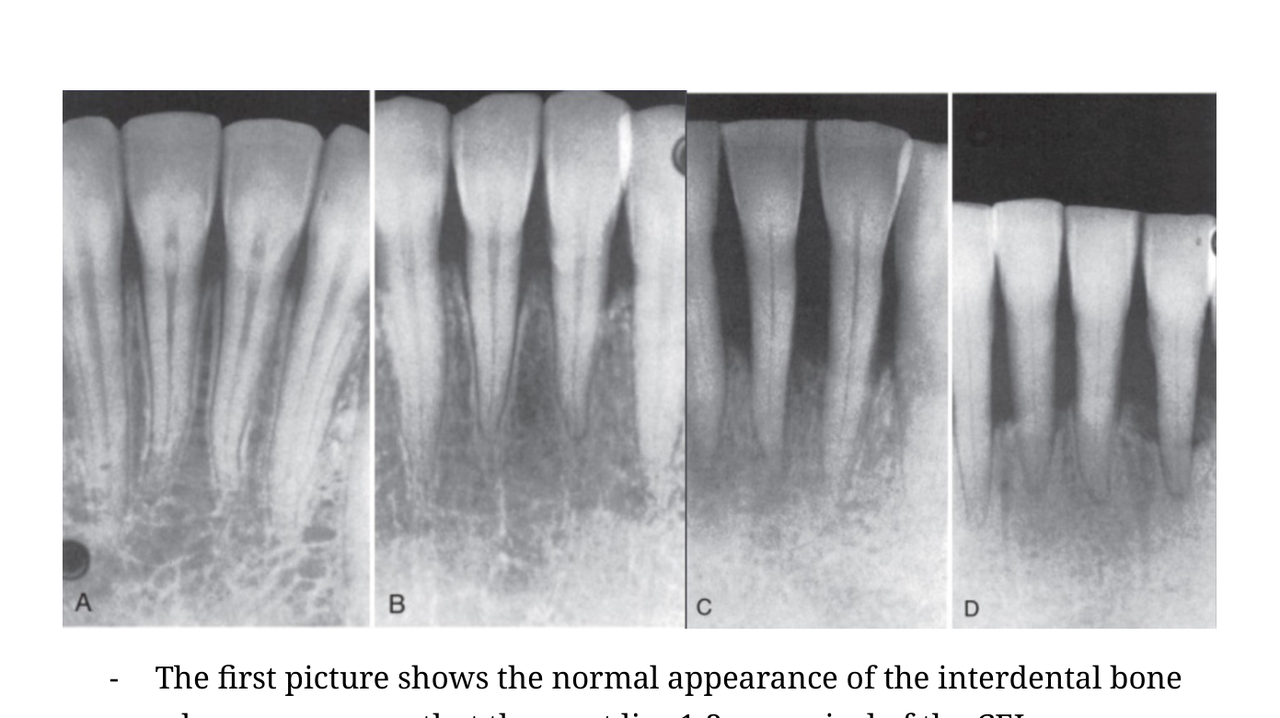
Flashcards in this deck (84)
-
What type of structures are visible on a radiograph?
Calcified structures.
radiology dentistry -
Which condition is not typically visible on a radiograph?
Periodontitis
Alveolar bone loss
Gingivitis
Changes in bone height
diagnosis dentistry -
What are the three physical changes to bone that may occur during periodontitis?
- Bone height
- Radiodensity
- Contour
periodontitis pathology -
What are the three components of a complete periodontal assessment?
- Visual/gingival assessment
- Periodontal charting
- Radiograph
assessment periodontics -
How does the shape of the interdental septum differ between front and posterior teeth?
Between front teeth, it is thin and pointed; between posterior teeth, it is flatter or rounded.
anatomy periodontics -
What is the normal distance from the CEJ to the alveolar crest in health?
1-3mm
anatomy periodontics -
What anatomical landmark dictates the location of the alveolar bone crest?
The cemento-enamel junction (CEJ) position.
dentistry anatomy -
In a healthy state, where is the alveolar crest typically located relative to the CEJ line?
It follows a horizontal contour 1-3mm below the line connecting the CEJs of adjacent teeth.
dentistry anatomy -
Why is the interdental septae the primary focus when evaluating periodontitis via radiographs?
Because the density of the root structure obscures the view of the facial and oral bone levels.
dentistry periodontitis -
What is the relationship between periodontal attachment loss and radiographic bone levels in periodontitis?
Bone levels lower progressively as inflammation extends and periodontal attachment is destroyed.
dentistry periodontitis -
What are the two common methods to describe the amount of bone loss in radiographs?
- Millimeters from the normal crest height
- Percentage of the overall root length
dentistry radiology -
If a tooth is tilted and not fully erupted, the CEJ position relative to an adjacent tooth can lead to the false appearance of what?
Alveolar bone loss
Root resorption
Increased bone density
Apical periodontitis
dentistry radiology -
What are the two primary anatomical landmarks needed to assess bone loss on a radiograph?
The cemento-enamel junction (CEJ) and the radiographic apex.
dentistry radiology periodontics -
What is the periodontitis stage associated with a radiographic bone loss of 15% - 33% in the coronal third?
Stage IV
Stage III
Stage II
Stage I
periodontics diagnosis -
What is the periodontitis stage associated with less than 15% radiographic bone loss?
Stage III
Stage I
Stage IV
Stage II
periodontics diagnosis -
What stage of periodontitis corresponds to bone loss extending to the middle to apical third?
Stage III or IV.
periodontics diagnosis -
If bone loss is measured to be 2 mm below the CEJ, what percentage of bone loss does this represent?
20% loss of bone.
periodontics diagnosis -
When assessing periodontal status, what clinical attachment loss is associated with 'Moderate' periodontitis severity?
3-4 mm.
periodontics diagnosis -
How is the area for bone loss assessment defined on a radiograph?
The area is defined by the distance between the cemento-enamel junction (CEJ) and the radiographic apex.
dentistry radiology -
In a healthy state, how far is the alveolar bone typically positioned relative to the cemento-enamel junction (CEJ)?
The alveolar bone is typically 2mm below the CEJ.
dentistry anatomy periodontics -
When assessing root length for bone loss calculations, why should 2mm be subtracted from the total root length indicated in standard dental tables?
To account for the supracrestal attached tissue.
dentistry anatomy radiology -
How is horizontal bone loss radiographically defined relative to the cemento-enamel junction (CEJ)?
It is described as a condition where the bone level is more than 1-3mm lower than the CEJ.
dentistry radiology periodontics -
If the full length of a tooth root is not visible on a bitewing radiograph, what is the standard method for estimating the root length to determine bone loss percentage?
Use a fixed universal root length of 10mm for all teeth.
Refer to tables providing average root lengths for specific teeth.
Estimate the root length by doubling the crown height.
Calculate the root length based solely on the patient's age.
dentistry radiology -
Which of the following describes the healthy distance of the alveolar bone from the CEJ?
0.5mm
5mm
2mm
10mm
dentistry anatomy -
What is the characteristic appearance of vertical or angular bone loss on a radiograph?
It appears as an irregular V-shape where the alveolar crest is more than 1-3mm lower than the CEJ, and the bone level is not parallel to the line between adjacent CEJs.
dentistry periodontology -
How is normal lamina dura observed on a dental radiograph?
It appears as a white, radiopaque, and continuous line.
dentistry radiology -
When a tooth is missing and adjacent teeth have drifted, what might appear to be vertical bone loss but is actually horizontal bone loss?
When the lamina dura is no longer continuous
When there is an irregular V-shape bone defect
When the bone level follows a parallel path to a line drawn through the CEJs
When the alveolar crest is 5mm below the CEJ
dentistry radiology -
Define the relationship between the alveolar bone and the cementoenamel junction (CEJ) in horizontal bone loss.
The alveolar bone level is parallel to the line drawn between the adjacent CEJs.
dentistry periodontology -
What is the microscopic structure of the lamina dura?
It is not a compact bone; it is a perforated structure containing many small holes that allow for the passage of blood vessels and nerves between the periodontal ligament (PDL) space and the bone.
dentistry radiology -
What radiographic changes to the lamina dura can indicate the early stages of periodontal disease?
- A break in the integrity of the lamina dura
- An irregular shape
- Increased radiolucency
dentistry periodontology -
Why is the absence of the lamina dura on a radiograph not always a reliable indicator of disease?
Because radiographic artifacts can occur that simulate the absence of the lamina dura.
dentistry radiology -
What radiographic sign in the lamina dura might indicate successful periodontal therapy?
Increased lengthening of the lamina dura.
dentistry therapy -
In a healthy tooth, how does the furcation area appear on a radiograph?
It appears as a bone-filled area.
dentistry anatomy -
What are the radiographic indicators for early versus advanced furcation involvement?
- Early involvement: A small black spot or slight thickening of the periodontal ligament space in the furcation.
- Advanced involvement: A large radiolucency between the roots.
dentistry radiology -
Why is furcation involvement often easier to identify on lower molars compared to upper molars?
On upper molars, the superimposition of palatal roots can mask the signs of furcation involvement.
dentistry radiology -
What is a specific radiographic indicator for identifying furcation involvement in the proximal region?
A triangular-shaped radiolucent lesion.
dentistry radiology -
What radiographic finding suggests the need for further clinical testing with a Nabers probe?
When the bone level is observed to be below the furcation entrance.
dentistry periodontics diagnostics -
How does clinical furcation involvement typically compare to radiographic findings?
Clinically, the furcation involvement is often much greater than what is visible on a radiograph.
dentistry periodontics diagnostics -
How does the healthy periodontal ligament (PDL) space appear on a radiograph?
As a fine, black, radiolucent line.
dentistry periodontics anatomy -
What changes in the periodontal ligament (PDL) space are indicative of disease?
A widening of the space, especially in the coronal part, or a complete thickening along the entire root surface.
dentistry periodontics pathology -
Besides periodontal disease, what conditions can cause a widening of the periodontal ligament (PDL) space?
- Occlusal trauma
- Vertical root fractures
- Periapical pathologies
dentistry periodontics pathology -
What is the recommended method to determine changes in bone height and the progression rate of disease?
Comparing two radiographs taken at different time points.
dentistry periodontics diagnostics -
When documenting bone loss on a radiograph, why should clinicians use specific quantitative measures instead of subjective descriptors like 'moderate' or 'severe'?
Using specific numbers (e.g., 60% or two-thirds) provides a more accurate understanding of the extent and severity of the bone loss.
dentistry periodontics documentation -
At what age range does crown mineralization typically reach completion?
Between 12 and 16 years.
dentistry development -
Based on the provided radiographic case study, what was the estimated bone loss over the 11-year follow-up?
More than 4mm.
dentistry periodontology -
What is the clinical role of radiographic findings in periodontal disease?
They may be recognized as a local contributing factor.
dentistry periodontology -
Can radiographs replace a thorough assessment of the root surface using an explorer probe?
No, radiographs cannot replace this assessment.
dentistry diagnostics -
How sensitive are radiographs at indicating the presence of calculus?
They are not a very sensitive indicator for the presence of calculus.
dentistry diagnostics -
What clinical changes can be observed on radiographs following dental debridement?
- Removal of gross calculus
- Changes indicating healing
dentistry treatment -
What condition suggests a potential violation of the supracrestal attached tissues?
A crown margin placed directly or in close proximity to the crestal bone.
dentistry periodontics -
What is a potential clinical consequence of an open or poorly contoured proximal contact?
It allows for food impaction.
dentistry restoration -
List three common radiographic signs of periodontal disease.
- Loss of lamina dura
- Horizontal bone loss
- Fuzziness in the crest
dentistry periodontitis -
What aspects of tooth and root morphology can be evaluated via radiographs during periodontitis?
- Root length
- Number of roots
dentistry periodontitis -
Which of the following is a radiographic sign of periodontal disease?
Root elongation
Increased density of the lamina dura
Decreased root length
Horizontal bone loss
dentistry periodontitis -
When evaluating restorations on a radiograph, what three clinical issues should be assessed?
- Overhangs
- Open proximal contacts
- Violation of supracrestal tissues
dentistry restoration -
What term describes the condition where dental roots appear to fuse together?
Convergent.
dentistry anatomy -
How is the root trunk defined in dentistry?
The dimension between the CEJ (cementoenamel junction) and the root furcation entrance.
dentistry anatomy -
How does the length of the root trunk influence the risk of furcation involvement?
Teeth with a very short root trunk tend to experience furcation involvement earlier than those with a long root trunk.
dentistry periodontics -
What is the clinical significance of a kink in a tooth root?
- Potential for future mobility loss
- Increased difficulty during extraction
- Increased difficulty for endodontic procedures (due to the need to bypass the kink)
dentistry endodontics -
What complication might arise when a root is bulbous on the middle third?
It may cause technical difficulties if the tooth needs to be extracted.
dentistry surgery -
What is the main concern when radiographically observing close root proximity between teeth?
Rapid cementum formation
Lack of adequate proximal bone
Increased furcation accessibility
Excessive crown length
dentistry radiography -
What is a potential concern regarding the proximity of periodontal defects in the upper jaw?
Periodontal defects can occur in close proximity to the sinus floor.
dentistry periodontics -
Why is it difficult to detect furcation involvement in upper premolars using standard radiographs?
The buccal and palatal roots often align with the x-ray beam, which can obscure the visibility of the furcation.
dentistry radiology -
How can endodontic and periodontal diseases interact?
The endodontium and periodontium communicate via the apex, allowing for potential interaction between pathologies in both systems.
dentistry endodontics periodontics -
What are two additional pathologies that may be diagnosed alongside common endodontic or periodontal issues?
- Resorption
- Root fracture
dentistry pathology -
What radiographic signs are associated with a vertical root fracture?
- Periapical radiolucency
- PDL widening
- Bone defects
dentistry radiology -
Why can radiographs be misleading when assessing three-dimensional bone defects?
Radiographs provide a two-dimensional image that can obscure details, such as an existing lingual bone plate covering a buccal bone defect.
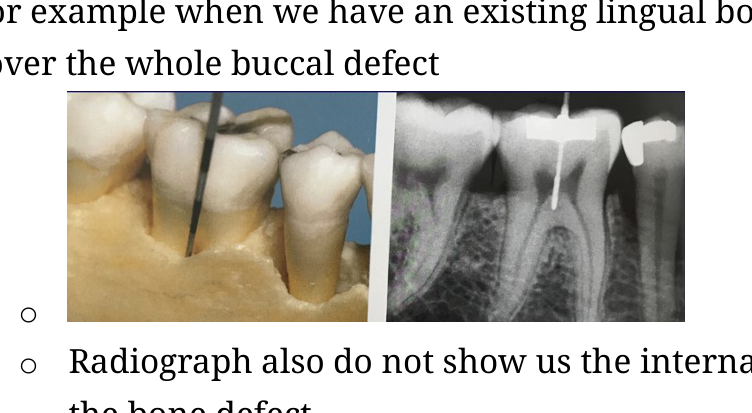 periodontics radiology
periodontics radiology -
What is the primary limitation of radiographs regarding current periodontal disease activity?
They provide a continuous, real-time monitoring of disease progression.
They are the gold standard for distinguishing between active and inactive disease phases.
They only show the result of past tissue destruction and do not reveal current activity like bleeding on probing or pus.
They accurately show the internal soft tissue morphology in high detail.
periodontics radiology -
Why must a clinician consider the ALARA principle when choosing to perform a cone beam CT scan?
While CBCT provides more detailed information than standard radiographs, it results in increased X-ray exposure for the patient, which must be justified.
radiology safety -
What is required for a complete periodontal evaluation and accurate defect localization?
A combination of clinical periodontal charting and radiographic assessment.
periodontics diagnosis -
At what stage of periodontal disease does evidence of attachment loss typically become obvious on a radiograph?
Radiographic evidence usually appears only after the disease has already progressed into a more moderate or advanced stage, making early detection dependent on clinical examination.
periodontics diagnosis -
Which of the following is true about the use of radiographs for monitoring periodontal disease?
They are sufficient on their own for evaluating soft tissue conditions.
They are the most sensitive method for detecting early-stage attachment loss.
They capture the internal morphology of every bone defect.
They provide only a snapshot of the disease state at a specific point in time.
periodontics radiology -
What is the potential discrepancy between the actual alveolar bone crest height and the height observed on radiographs?
The height can differ by up to 1.6mm, often leading to an underestimation of bone loss.
radiography periodontics diagnostic -
How does an OPG (Orthopantomogram) compare to a periapical radiograph regarding the assessment of alveolar bone levels?
OPG is less detailed and lacks the accuracy of periapical radiographs.
OPG provides identical levels of detail as periapical radiographs.
OPG is completely unsuitable for evaluating any bone levels.
OPG is more detailed and accurate than periapical radiographs.
radiography comparison -
Why are bitewing (BW) radiographs often preferred over periapical (PA) radiographs for evaluating crestal bone height?
BW radiographs provide better projection geometry for accurate visualization of crestal bone height.
radiography diagnostic -
What is a major limitation of using bitewing (BW) radiographs to evaluate bone loss?
They cause extreme distortion in all patient cases.
They are only effective for visualizing furcation involvement.
They are unable to visualize bone loss greater than 5mm.
They cannot visualize bone loss of any depth.
radiography limitations -
What is the primary purpose of employing the cone paralleling technique during dental radiography?
To prevent extreme image distortion.
radiography technique -
How should a practitioner decide which type of radiograph to take for a periodontal evaluation?
The choice must be individualized and tailored to the unique diagnostic needs of the patient.
radiography clinical -
Where is the crest of the interdental bone located relative to the CEJ in a normal radiograph?
The crest lies 1-2 mm apical to the CEJ.
dentistry radiography periodontics -
What are the common radiographic signs of early periodontal bone changes?
- Fuzziness
- A break in the continuity of the lamina dura
- Widening of the PDL
dentistry radiography periodontics -
What shape do the radiolucent areas at the crest take during early periodontal changes?
They appear as little wedge-shaped radiolucent areas.
dentistry radiography -
What is the primary radiographic change indicating progression of periodontal disease in the interdental septum?
The height of the interdental septum is progressively reduced.
dentistry radiography periodontics -
What bone condition is often visible around tooth 32 in advanced periodontal disease?
A bone crater.
dentistry radiography -
Describe the radiographic sequence of periodontal bone changes shown in the series of radiographs.
The progression is marked by: - Normal appearance (crest 1-2mm apical of CEJ) - Fuzziness and loss of lamina dura continuity - Reduced height of the interdental septum - Bone cratering
dentistry radiography periodontics