Sign up to unlock more features
- Save this deck to your account
- Study flashcards with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from PDFs and documents
- Better text extraction from your PDFs and documents
- Better flashcards with our more advanced AI model
Flashcards in this deck (237)
-
A patient with non-Hodgkin lymphoma receiving chemotherapy should receive annual vaccination for influenza.
internal_medicine step2. -
Influenza can be complicated by lower respiratory tract infections such as pneumonia and bacterial superinfection.
internal_medicine step2. -
internal_medicine step2.
-
internal_medicine step2.
-
The influenza vaccine can be administered as a trivalent or quadrivalent intramuscular injection or as a nasal spray.
internal_medicine step2. -
internal_medicine step2.
-
The symptoms of influenza include fever, chills, myalgias, malaise, headaches, cough, nausea, and vomiting.
internal_medicine step2. -
The measles-mumps-rubella vaccine is a live attenuated vaccine and is contraindicated in severely immunocompromised patients.
internal_medicine step2. -
internal_medicine step2.
-
internal_medicine step2.
-
internal_medicine step2.
-
The influenza vaccine is crucial for patients with high-risk conditions to prevent influenza-related complications.
internal_medicine step2. -
internal_medicine vaccination step2.
-
Influenza can be complicated by lower respiratory tract infection (pneumonia) and bacterial superinfection.
internal_medicine infectious_disease step2. -
Symptoms of influenza include fever, chills, myalgias, malaise, headaches, cough, nausea, and vomiting.
internal_medicine symptoms step2. -
The influenza vaccine can be administered in two forms: trivalent or quadrivalent intramuscular injection of inactivated virus, or as a nasal spray of live attenuated virus.
internal_medicine vaccination step2. -
internal_medicine vaccination immunocompromised step2.
-
Patients who are immunocompromised may be at higher risk for severe illness from influenza if they do not receive vaccination.
internal_medicine immunocompromised step2. -
internal_medicine vaccination step2.
-
The measles-mumps-rubella vaccine is a live attenuated vaccine and is contraindicated in severely immunocompromised patients due to the risk of viral reactivation.
pediatrics vaccination immunocompromised step2. -
The meningococcal vaccine is a conjugate vaccine recommended for all children, with an additional serogroup B vaccine for those at increased risk.
pediatrics infectious_disease step2. -
While meningococcal vaccine can safely be given to immunocompromised patients, boosters are not routinely necessary.
internal_medicine vaccination immunocompromised step2. -
The pneumococcal vaccine is indicated for all adults over 65 years and those with high-risk conditions like chronic heart, renal, or liver disease.
internal_medicine vaccination step2. -
internal_medicine vaccination step2.
-
pediatrics vaccination step2.
-
Zoster vaccine for shingles is recommended for adults greater than 60 years and is also a live attenuated vaccine.
internal_medicine vaccination step2. -
internal_medicine vaccination immunocompromised step2.
-
The educational objective emphasizes that the influenza vaccine is crucial for patients who may be at higher risk for severe illness and complications from influenza.
internal_medicine vaccination step2. -
The most appropriate next step in diagnosis for a patient with recurrent episodes of vaginal candidiasis and genital herpes is HIV testing.
obgyn internal_medicine step2. -
HIV testing is recommended for sexually active individuals over the age of 13, especially for those with high-risk sexual behavior.
obgyn internal_medicine step2. -
Frequent HIV testing is indicated for those who have numerous sexual partners and rarely use barrier protection.
obgyn internal_medicine step2. -
A patient with a history of recurrent genital herpes and vaginal candidiasis is suggested to have underlying immunodeficiency.
obgyn internal_medicine step2. -
If the fourth-generation HIV test is positive, further testing to differentiate between HIV-1 and HIV-2 is indicated.
obgyn internal_medicine step2. -
If the fourth-generation test is positive but antibody testing is negative, measuring the HIV viral load should be performed.
obgyn internal_medicine step2. -
obgyn internal_medicine step2.
-
Fungal culture is unnecessary because vaginal candidiasis can be diagnosed by microscopy of vaginal secretion.
obgyn internal_medicine step2. -
Genital herpes can be diagnosed clinically but requires laboratory confirmation during the first episode.
obgyn internal_medicine step2. -
The gold standard for diagnosing herpes infection is viral culture, although PCR-based tests are preferred.
obgyn internal_medicine step2. -
obgyn internal_medicine step2.
-
obgyn internal_medicine step2.
-
The most appropriate next step in diagnosis for this patient with high-risk sexual behavior and recurrent episodes of vaginal candidiasis is HIV testing.
internal_medicine step2. -
internal_medicine step2.
-
Populations that require more frequent HIV screening include those with numerous sexual partners and injection drug users.
internal_medicine step2. -
The patient's history of recurrent vaginal candidiasis and genital herpes strongly suggests underlying immunodeficiency.
internal_medicine step2. -
internal_medicine step2.
-
If the fourth-generation HIV test is positive, further testing is needed to differentiate between infection with HIV-1 or HIV-2.
internal_medicine step2. -
If antibody testing following a positive fourth-generation test is negative or indeterminate, the next step is to measure the HIV viral load.
internal_medicine step2. -
A positive HIV test should prompt immediate initiation of highly active antiretroviral therapy (HAART).
internal_medicine step2. -
Fungal culture is unnecessary for diagnosing vaginal candidiasis because yeast forms are readily appreciated on microscopy.
obgyn step2. -
Genital herpes infection can be diagnosed clinically in the presence of characteristic lesions, but laboratory confirmation is necessary for the first episode.
obgyn step2. -
The preferred method of screening for HPV infection is cervical cytology alone or together with a PCR-based assay.
obgyn step2. -
obgyn step2.
-
internal_medicine step2.
-
Testing for HIV is prudent for patients exhibiting symptoms such as recurrent vaginal infections, indicating possible HIV infection.
internal_medicine step2. -
The educational objective emphasizes the need for HIV testing using a fourth-generation antigen/antibody test.
internal_medicine step2. -
The patient is a 32-year-old African American man with iron deficiency anemia who has adhered to his medication regimen of ferrous sulfate for 6 months.
internal_medicine step2 -
Laboratory studies showed that the patient's hemoglobin increased from 10.7 g/dL to 10.9 g/dL over 6 months.
internal_medicine step2 -
The patient's red cell distribution width (RDW) is normal despite the anemia, suggesting hemostatic function may not be impaired.
internal_medicine step2 -
The blood smear findings of microcytosis and target cells in this patient are indicative of thalassemia.
internal_medicine step2 -
In this male patient, the absence of bloody vomiting, blood in stool, or blood in urine suggests that occult gastrointestinal bleeding is less likely.
internal_medicine step2 -
The patient's serum iron levels revealed that he had a level of 60 µg/dL with a transferrin saturation of 25% six months ago and a level of 75 µg/dL with a transferrin saturation of 35% today.
internal_medicine step2 -
Thalassemia is the most likely diagnosis for this patient because he has mild microcytic anemia with a normal red cell distribution width (RDW) and normal iron studies.
internal_medicine step2 -
Celiac disease often presents with malabsorption and changes in gut lining rather than solely with anemia, making it less likely in this case.
internal_medicine step2 -
Myelodysplastic syndrome typically involves abnormal blood counts and a high RDW, which is not seen in this patient.
internal_medicine step2 -
Pure red blood cell aplasia would show marked reductions in reticulocyte count and red cells, which are not present here, confirming it's less likely.
internal_medicine step2 -
Occult gastrointestinal bleeding would most likely present with positive stool guaiac tests or significant changes in iron studies, which are absent in this case.
internal_medicine step2 -
Normal iron studies indicate the absence of iron deficiency as a cause of the patient's anemia, leading to the diagnosis of thalassemia.
internal_medicine step2 -
The management of thalassemia in this patient would focus on monitoring and treating complications rather than immediate iron supplementation due to normal iron levels.
internal_medicine step2 -
In diagnosing microcytic anemia, a key consideration is the patient's iron studies, including serum iron and ferritin levels.
internal_medicine step2 -
Patients with thalassemia often maintain normal iron levels despite chronic anemia, as seen in this patient who presented with a normal RDW.
internal_medicine step2 -
Thalassemia is characterized by one or more alleles of the a- or β-globin genes being rendered nonfunctional.
internal_medicine step2 -
internal_medicine step2
-
In patients with β-thalassemia, the normal HbA cannot be effectively assembled, leading to the formation of insoluble tetramers from excess a-globin chains.
internal_medicine step2 -
Patients with a-thalassemia trait often exhibit minimal decreases in hemoglobin and may be asymptomatic.
internal_medicine step2 -
Microcytosis and the presence of target cells on a peripheral blood smear are characteristic of both a- and β-thalassemia.
internal_medicine step2 -
internal_medicine step2
-
internal_medicine step2
-
Occult gastrointestinal bleeding is associated with iron deficiency anemia that should respond to oral iron therapy.
internal_medicine step2 -
Microcytic anemia associated with myelodysplastic syndrome is typically not isolated, as it presents with cytopenias of various lineages.
internal_medicine step2 -
internal_medicine step2
-
internal_medicine step2
-
Thalassemia is most likely diagnosed in patients with mild microcytic anemia and normal red cell distribution width (RDW).
internal_medicine step2 -
internal_medicine step2
-
Normal adult hemoglobin consists of two α-globin subunits and two β-globin subunits, forming a unique conformation called hemoglobin A (HbA).
internal_medicine step2 -
Patients with β-thalassemia have difficulty assembling the normal HbA molecule, leading to the formation of excess α-globin chains.
internal_medicine step2 -
internal_medicine step2
-
Microcytosis and the presence of target cells on peripheral blood smear are characteristic of both α- and β-thalassemia.
internal_medicine step2 -
Patients with thalassemia trait may be incorrectly diagnosed with iron deficiency anemia because oral iron therapy will have no effect on their hemoglobin concentrations.
internal_medicine step2 -
internal_medicine step2
-
Celiac disease typically presents with microcytic anemia, an increased RDW, and transferrin saturation below 20%.
internal_medicine step2 -
Myelodysplastic syndrome often presents with cytopenias but microcytic anemia in isolation is atypical.
internal_medicine step2 -
Occult gastrointestinal bleeding should respond to oral iron therapy, unlike in patients with thalassemia.
internal_medicine step2 -
Pure red blood cell aplasia results in complete destruction of erythrocyte precursors and presents with profound anemia.
internal_medicine step2 -
Normal human hemoglobin A consists of two α-globin and two β-globin subunits; mutations in these lead to thalassemia.
internal_medicine step2 -
In thalassemia trait or thalassemia minor, patients present with mild microcytic anemia and normal iron studies.
internal_medicine step2 -
internal_medicine step2
-
A 23-year-old man with sickle cell disease presents with low back pain and nausea. He rates the pain as 8 on a 10-point scale.
internal_medicine step2. -
His vital signs are within normal limits, but he has pale conjunctivae and a hemoglobin concentration of 7.2 g/dL.
internal_medicine step2. -
internal_medicine step2.
-
In addition to administration of oxygen and 0.9% saline, the most appropriate next step in pharmacotherapy is intravenous morphine.
internal_medicine step2. -
Patients with sickle cell disease commonly experience acute painful episodes due to vaso-occlusive phenomena.
internal_medicine step2. -
internal_medicine step2.
-
internal_medicine step2.
-
Rapid assessment is critical to determine concomitant disorders, including acute chest syndrome, myocardial infarction, and venous thromboembolism.
internal_medicine step2. -
The rapid administration of analgesia, often with opiate medication, is crucial in managing acute pain in sickle cell disease.
internal_medicine step2. -
Patients with sickle cell disease may require higher doses of opiate medications due to chronic exposure.
internal_medicine step2. -
Reversal of hypoxia, hypovolemia, and acid/base disturbances should be prioritized in managing pain crises.
internal_medicine step2. -
Oral medications like celecoxib and oxycodone may not provide sufficient analgesia for acute pain in sickle cell disease.
internal_medicine step2. -
Given the patient's low oral intake, a parenteral route of administration is preferred for analgesia.
internal_medicine step2. -
Incorrect answers to the question included oral celecoxib, oral oxycodone, intramuscular ketorolac, and intravenous meperidine.
step2. internal_medicine -
The most appropriate medication to administer to a patient experiencing an acute painful episode in sickle cell disease is intravenous morphine.
internal_medicine step2 -
internal_medicine step2
-
Acute painful episodes, sometimes referred to as pain crises, are a manifestation of vaso-occlusive phenomena in sickle cell disease.
internal_medicine step2 -
internal_medicine step2
-
internal_medicine step2
-
Rapid assessment of the patient is critical to determine if there are concomitant disorders such as acute chest syndrome, myocardial infarction, venous thromboembolism, or infection.
internal_medicine step2 -
The rapid administration of analgesia is crucial for treating acute painful episodes in sickle cell disease.
internal_medicine step2 -
Patients with sickle cell disease require substantially higher doses of opiate medications due to chronic exposure, compared to opiate-naive patients.
internal_medicine step2 -
Reversal of inciting features such as hypoxia, hypovolemia, and infection should be prioritized in the management of sickle cell pain.
internal_medicine step2 -
Oral medications such as oral celecoxib and oral oxycodone may be appropriate for chronic pain but are not sufficient for acute painful crises in sickle cell patients.
internal_medicine step2 -
Intramuscular ketorolac is not preferred for acute painful episodes in sickle cell disease because it is unlikely to produce the required level of analgesia.
internal_medicine step2 -
Intravenous meperidine is rarely used for acute pain due to its challenging pharmacodynamics and kinetics.
internal_medicine step2 -
The best-next-step in managing an acute painful episode in a patient with sickle cell disease is to promptly administer intravenous opiates.
internal_medicine step2 -
For effective management of pain crises, some centers use an individualized and predefined pain pathway for treatment.
internal_medicine step2 -
Missing key features such as acute chest syndrome at assessment can lead to inadequate treatment of pain in sickle cell disease.
internal_medicine step2 -
The educational objective emphasizes the need for rapid assessment to identify concomitant disorders, which should coincide with administration of intravenous opiates.
internal_medicine step2 -
neurology internal_medicine step2
-
Uncontrolled hypertension is associated with an approximately two-fold increase in the risk for ischemic stroke.
neurology internal_medicine step2 -
neurology internal_medicine step2
-
Lifestyle modifications for stroke prevention include weight loss, dietary modification, smoking cessation, and regular exercise.
neurology internal_medicine step2 -
Abnormal serum lipid concentrations have not been consistently demonstrated as a risk factor for all stroke subtypes.
neurology internal_medicine step2 -
neurology internal_medicine step2
-
Increases in serum glucose concentration are significant for ischemic stroke in the context of diabetes mellitus.
neurology internal_medicine step2 -
While abnormal serum lipid concentrations may play a modest role, hypertension is considered more significant in the development of ischemic strokes.
neurology internal_medicine step2 -
neurology internal_medicine step2
-
neurology internal_medicine step2
-
neurology internal_medicine step2
-
neurology internal_medicine step2
-
Hypertension is the greatest modifiable risk factor for cerebral infarction and contributes to cardiac and renal failure.
neurology internal_medicine step2 -
Uncontrolled hypertension is associated with an approximately two-fold increase in the risk for ischemic stroke.
neurology internal_medicine step2 -
neurology internal_medicine step2
-
Initiation of antihypertensive therapy is important for stroke prevention, along with lifestyle modifications.
neurology internal_medicine step2 -
Lifestyle modifications for stroke prevention include weight loss, dietary modification, and smoking cessation.
neurology internal_medicine step2 -
Abnormal serum lipid concentrations have not been consistently shown to be a significant risk factor for all stroke subtypes.
neurology internal_medicine step2 -
Family history of cerebral infarction is an important non-modifiable risk factor but not as significant as hypertension.
neurology internal_medicine step2 -
An increase in serum glucose concentration is a significant risk factor for ischemic stroke when associated with diabetes mellitus.
neurology internal_medicine step2 -
Smoking history is an important modifiable risk factor for ischemic stroke, but the relative risk is less than that of hypertension.
neurology internal_medicine step2 -
The American Heart Association states that family history is not as important as hypertension and has not been consistently demonstrated as a risk factor in large studies.
neurology internal_medicine step2 -
Risk factors for cerebral infarction include: hypertension, abnormal serum lipids, family history, and smoking.
neurology internal_medicine step2 -
internal_medicine step2
-
The conversion of arachidonic acid to thromboxane A2 is prevented by aspirin, reducing platelet activation.
internal_medicine step2 -
internal_medicine step2
-
Salicylate poisoning leads to a delayed anion-gap metabolic acidosis due to effects on the electron transport chain.
internal_medicine step2 -
internal_medicine step2
-
Symptoms of acute salicylate toxicity include hyperventilation, gastrointestinal upset, and tinnitus.
internal_medicine step2 -
internal_medicine step2
-
Management of salicylate toxicity involves systemic alkalinization with sodium bicarbonate infusion.
internal_medicine step2 -
Patients with severe altered mental status may require dialysis as part of salicylate toxicity management.
internal_medicine step2 -
Hyponatremia is unlikely in salicylate poisoning, which helps differentiate between causes of metabolic acidosis and patient diagnosis.
internal_medicine step2 -
internal_medicine step2
-
internal_medicine step2
-
internal_medicine step2
-
Choice D indicates hyperkalemia, typically associated with renal insufficiency, not salicylate toxicity.
internal_medicine step2 -
internal_medicine step2
-
internal_medicine step2.
-
internal_medicine step2.
-
internal_medicine step2.
-
internal_medicine step2.
-
internal_medicine step2.
-
Salicylate's decoupling effects on the electron transport chain result in increased anaerobic metabolism.
internal_medicine step2. -
internal_medicine step2.
-
Patients with acute salicylate toxicity may present with hyperventilation and gastrointestinal upset.
internal_medicine step2. -
internal_medicine step2.
-
Mild salicylate toxicity may present with an increased anion gap and compensated metabolic acidosis.
internal_medicine step2. -
Management for salicylate toxicity involves systemic alkalinization using sodium bicarbonate infusion.
internal_medicine step2. -
internal_medicine step2.
-
Salicylate poisoning is unlikely to cause hyponatremia (Choice A), as it does not typically impact sodium levels.
step2. internal_medicine -
Hypokalemia is unlikely in salicylate toxicity (Choice B); it generally does not affect potassium serum concentrations.
internal_medicine step2. -
Salicylate toxicity would not result in hyperkalemia (Choices D and F); hyperkalemia is seen in conditions like renal insufficiency.
internal_medicine step2. -
In salicylate toxicity, the bicarbonate concentration would not be normal or increased (Choices D, E, F).
internal_medicine step2. -
Early stages of salicylate poisoning show respiratory alkalosis but not mild metabolic alkalosis (Choice E).
internal_medicine step2. -
internal_medicine step2.
-
A 23-year-old woman presents with a lesion on her lip characterized by a grouping of discrete, clear, fluid-filled vesicles that are 5 mm in diameter, indicative of herpes simplex.
internal_medicine neurology step2 -
The prodromal symptoms of herpes labialis may include burning, tingling, and itching before the appearance of vesicular lesions.
internal_medicine neurology step2 -
Herpes simplex virus (HSV) commonly affects the oral-labial margin, often leading to painful ulcers with an erythematous border.
internal_medicine neurology step2 -
The diagnosis of herpes labialis is confirmed with viral culture or polymerase chain reaction testing from the base of the lesion.
internal_medicine neurology step2 -
Reactivation of HSV may occur from latency in the trigeminal ganglion, producing painful vesicles with associated lymphadenopathy.
internal_medicine neurology step2 -
Treatment of herpes labialis includes antiviral agents that inhibit viral DNA polymerase, such as acyclovir, valacyclovir, and famciclovir.
internal_medicine neurology step2 -
Chickenpox is caused by the varicella-zoster virus (VZV), presenting with a diffuse rash of fluid-filled vesicles, unlike the localized lesions seen in herpes simplex.
internal_medicine neurology step2 -
Unlike herpes simplex, erythema multiforme presents with targetoid lesions on palms and soles and is often triggered by drugs and certain infections.
internal_medicine neurology step2 -
Herpes zoster (shingles) manifests with multiple vesicular lesions in a unilateral, dermatomal distribution.
internal_medicine neurology step2 -
The correct diagnosis for a patient presenting with tingling, burning sensation in the lip followed by vesicles is herpes simplex.
internal_medicine neurology step2 -
For herpes simplex treatment, antiviral choices may vary based on severity and include agents such as acyclovir and valacyclovir.
internal_medicine neurology step2 -
Herpes labialis typically begins with the formation of vesicles at the oral-labial margin, which lyse and progress to shallow, painful ulcers with an erythematous border.
internal_medicine neurology step2. -
Many patients with herpes labialis experience prodromal symptoms such as burning, tingling, itching, or pain for several days prior to vesicular lesions.
internal_medicine step2. -
internal_medicine neurology step2.
-
Following initial infection, HSV may be latent in the trigeminal ganglion until reactivation occurs.
internal_medicine neurology step2. -
Reactivation of HSV causes painful vesicles and punched-out erosions on the lip with associated lymphadenopathy.
internal_medicine neurology step2. -
Reactivation of HSV can be triggered by stress, sunlight, or local trauma such as dental procedures.
internal_medicine neurology step2. -
The diagnosis of herpes labialis is confirmed with a viral culture or polymerase chain reaction test from the base of the lesion if uncertain.
internal_medicine step2. -
Treatment for herpes labialis includes antiviral agents that inhibit viral DNA polymerase, such as acyclovir, valacyclovir, and famciclovir.
internal_medicine step2. -
internal_medicine step2.
-
Chickenpox is caused by primary infection with varicella-zoster virus (VZV) and does not present with localized vesicular lesions at the oral-labial margin.
internal_medicine neurology step2. -
Erythema multiforme is characterized by targetoid lesions and may be associated with fever and myalgias.
internal_medicine step2. -
internal_medicine step2.
-
internal_medicine step2.
-
Erythema nodosum may be associated with conditions such as inflammatory bowel disease, sarcoidosis, and bacterial or viral infections.
internal_medicine step2. -
internal_medicine step2.
-
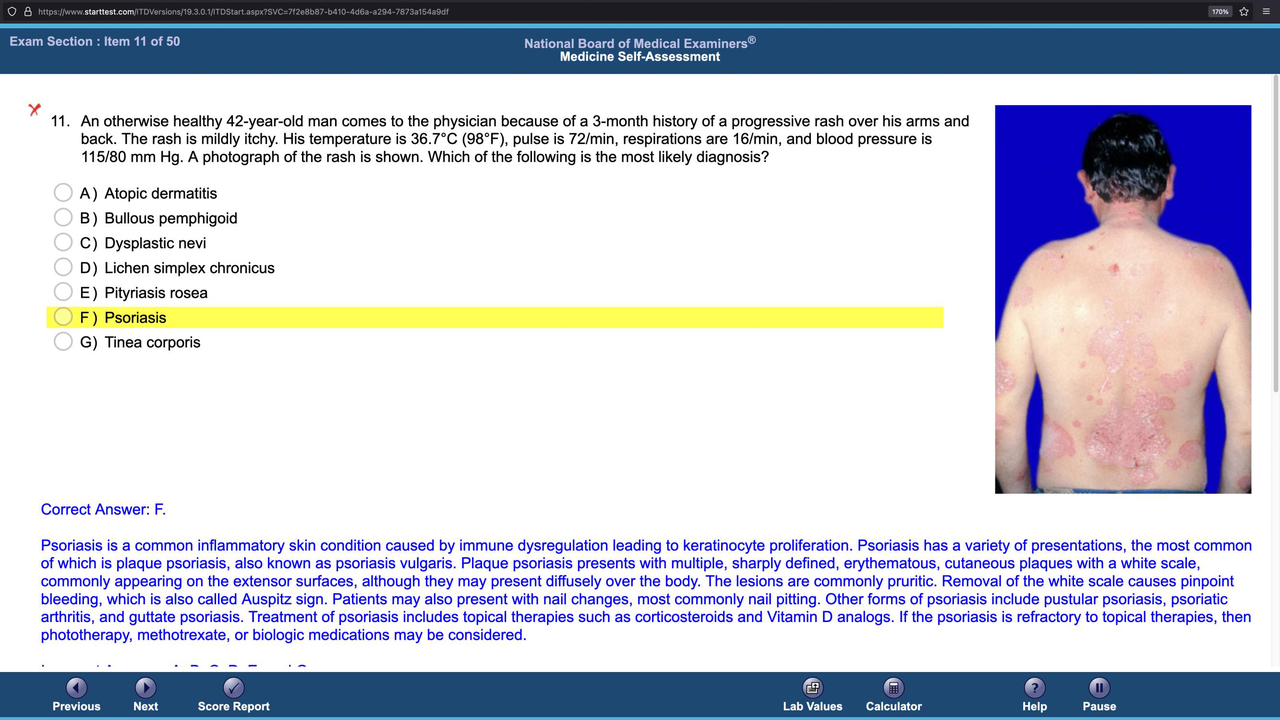
An otherwise healthy 42-year-old man presents with a progressive rash over his arms and back. The rash is likely to be psoriasis.
internal_medicine step2 -
internal_medicine step2
-
internal_medicine step2
-
internal_medicine step2
-
In psoriasis, removal of the white scale causes Auspitz sign, which is characterized by pinpoint bleeding.
internal_medicine step2 -
internal_medicine step2
-
If psoriasis is refractory to topical therapies, potential management options include phototherapy, methotrexate, and biologic medications.
internal_medicine step2 -
The correct answer for a rash that is mildly itchy and has a characteristic appearance is F) Psoriasis.
internal_medicine step2 -
Why is atopic dermatitis incorrect for this presentation? It typically presents with pruritic eczema rather than plaque-like lesions.
internal_medicine step2 -
Bullous pemphigoid is not the diagnosis here because it present with blisters instead of well-defined plaques.
internal_medicine step2 -
internal_medicine step2
-
Tinea corporis, or ringworm, would present with a scaling ring rather than patches seen in psoriasis.
internal_medicine step2 -
What distinguishes the rash of psoriasis from pityriasis rosea? Psoriasis has sharply defined edges compared to less clear borders in pityriasis rosea.
internal_medicine step2 -
Psoriasis is a common inflammatory skin condition caused by immune dysregulation leading to keratinocyte proliferation.
internal_medicine dermatology step2. -
internal_medicine dermatology step2.
-
Plaque psoriasis presents with multiple, sharply defined, erythematous cutaneous plaques with a white scale.
internal_medicine dermatology step2. -
The lesions in plaque psoriasis are commonly pruritic and removal of the white scale causes pinpoint bleeding (Auspitz sign).
internal_medicine dermatology step2. -
internal_medicine dermatology step2.
-
internal_medicine dermatology step2.
-
internal_medicine dermatology step2.
-
If psoriasis is refractory to topical therapies, then phototherapy, methotrexate, or biologic medications may be considered.
internal_medicine dermatology step2. -
internal_medicine dermatology step2.
-
internal_medicine dermatology step2.
-
Bullous pemphigoid is characterized by antibodies against hemidesmosome and presents with tense bullae.
internal_medicine dermatology step2. -
internal_medicine dermatology step2.
-
internal_medicine dermatology step2.
-
Pityriasis rosea often follows a viral infection and is characterized by the acute onset of a pruritic patch.
internal_medicine dermatology step2. -
internal_medicine dermatology step2.
-
internal_medicine dermatology step2.
Risk Factors for Cerebral Infarction
Patient Overview
- 72-year-old man with poorly controlled hypertension
- Family history of cerebral infarction; vital signs: 150/105 mm Hg
Risk Factor Assessment
- A) Abnormal serum lipid concentrations
- B) Family history of cerebral infarction
- C) Hypertension
- D) Increase in serum glucose concentration
- E) Smoking history
Correct Answer: C) Hypertension
Rationale:
- Major modifiable risk factor for stroke; needs control through lifestyle changes and medications.
Incorrect Options:
- A) Abnormal serum lipid:
- Less prominent risk compared to hypertension.
- B) Family history:
- Important but not as critical as hypertension.
- D) Increased glucose:
- Significant in cases of diabetes but secondary to hypertension.
- E) Smoking:
- Important modifiable factor but less impactful than hypertension.
Management of Salicylate Toxicity
Patient Overview
- 77-year-old woman taking aspirin for degenerative arthritis; experiencing ringing in ears and pain
Laboratory Findings
What is most likely to be present? - A) Na+: 112 - B) Na+: 132 - C) Na+: 140 - D) Na+: 154 - E) Na+: 154
Correct Answer: C) Na+: 132
Rationale:
- Salicylate toxicity often leads to respiratory alkalosis followed by metabolic acidosis due to increased anaerobic metabolism.
Incorrect Options:
- A) Na+: 112: Low sodium unlikely in this context.
- B) Na+: 132: Not compatible with expected findings.
- D) Na+: 154: Too high; unlikely seen in salicylate toxicity context.
- E) Na+: 154: Similar rationale as above for not being plausible.
Diagnosis of Oral Lesions
Patient Overview
- 23-year-old woman presents with lesions on lip, burning sensation
Differential Diagnosis
- A) Chickenpox
- B) Erythema multiforme
- C) Erythema nodosum
- D) Herpes simplex
- E) Herpes zoster
Correct Answer: D) Herpes Simplex
Rationale:
- Characterized by vesicles that progress to shallow ulcers with burning/tingling precursors.
Incorrect Options:
- A) Chickenpox: Not localized to lips.
- B) Erythema multiforme: Presents differently.
- C) Erythema nodosum: Nodal presentation, not vesicular.
- E) Herpes zoster: Systemic presentation, not localized oral lesions.
Psoriasis Overview
Patient Presentation
- 42-year-old male with itchy rash over arms and back
Differential Diagnosis
- A) Atopic dermatitis
- B) Bullous pemphigoid
- C) Dysplastic nevi
- D) Lichen simplex chronicus
- E) Pityriasis rosea
- F) Psoriasis
- G) Tinea corporis
Correct Answer: F) Psoriasis
Rationale:
- Characterized by well-defined plaques with scaling; commonly on extensor surfaces.
Incorrect Options:
- A) Atopic dermatitis: Flexural lesions.
- B) Bullous pemphigoid: Not typically in younger adults.
- C) Dysplastic nevi: Not consistent presentation.
- D) Lichen simplex chronicus: Associated with irritation, not widespread.
- E) Pityriasis rosea: More seasonal and viral correlated rash.
- G) Tinea corporis: Fungal infection, usually with rings.