Sign up to unlock more features
- Save this deck to your account
- Study flashcards with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from PDFs and documents
- Better text extraction from your PDFs and documents
- Better flashcards with our more advanced AI model
What does ENT stand for in the context of Otolaryngology?
Ear, Nose, and Throat
Ear, Nose, and Therapy
Ear, Nose, and Transplant
Ear, Nose, and Treatment
Which of the following is NOT a sub-specialty of Otolaryngology?
Rhinology and Endoscopic Sinus Surgery
Paediatric Otolaryngology
Otology/Neurotology and Skull Base Surgery
Facial Plastics
What percentage of general practice is estimated to deal with ENT pathology?
30-40%
10-15%
50-60%
20-30%
What is one of the key skills expected to be performed during the rotation in Otolaryngology?
Neurological Exam
Otoscopy
Cardiac Exam
Dermatological Exam
Which of the following is a necessary clinical skill to learn during the Otolaryngology rotation?
Performing a lumbar puncture
Administering anesthesia
Conducting a physical therapy session
Taking a full ENT history
What is a primary focus of Otolaryngology as a specialty?
Specific organ system
Pharmacology
Genetics
Anatomical region
Which examination is part of the course objectives in Otolaryngology?
Cardiac examination
Abdominal examination
Thyroid examination
Lung examination
What should a student differentiate regarding ENT diseases?
When to prescribe antibiotics
When to refer to a psychologist
When to perform surgery
When a patient requires primary treatment
Which conditions require a specialist ENT opinion?
Common cold
Seasonal allergies
Minor ear infections
Conditions that cannot be managed by a GP
What is necessary for understanding common ENT diseases?
Knowledge of dermatology
Knowledge of pharmacology and toxicology
Knowledge of surgery techniques
Knowledge of pediatrics
What types of referrals are mentioned for ENT conditions?
Immediate hospitalization
Home remedies
Over-the-counter treatment
Routine or urgent referral
What is the most important sense for communication among humans?
Touch
Sight
Hearing
Smell
What do sound waves disturb in the air?
Molecules
Atoms
Electrons
Particles
What part of the ear transmits vibrations to the cochlea?
Inner ear
Middle ear
Outer ear
Eustachian tube
At what decibel level can permanent damage to the inner ear occur?
120dB
80dB
90dB
10dB
Which side of the brain mainly interprets speech?
Both sides
Right side
Left side
Neither side
Which structure in the ear is responsible for balance?
Eustachian tube
Inner ear
Middle ear
Cochlea
What is the function of the cochlea?
Transmit sound waves
Balance
Interpret sound
Regulate pressure
What does the diagram of the ear illustrate?
Function of the ear
Anatomy of the ear
Balance mechanism
Hearing process
What is the quietest sound that can be detected?
10dB
15dB
20dB
5dB
Which part of the ear is involved in transmitting sound vibrations?
Semicircular canals
Auricle
Cochlea
Tympanic membrane
What triggers strong emotional responses related to sound?
Smelling
Seeing
Touching
Hearing
What is the function of the tympanic membrane in the ear?
It stabilizes balance
It transmits nerve impulses
It vibrates in response to sound waves
It contains the cochlea
Which structure contains the organ of Corti?
Cochlea
Semicircular canals
Tympanic membrane
Utricle
What are the three tiny bones in the middle ear called?
Cochlea, Utricle, Saccule
Tympanic, Auditory, Semicircular
Malleus, Incus, Stapes
Vestibule, Cristae, Macula
How do low frequency sound waves affect the cochlea?
They stimulate the apex of the cochlea
They cause the tympanic membrane to vibrate
They stimulate the base of the cochlea
They affect the semicircular canals
What is the role of the vestibular apparatus?
To vibrate in response to sound
To help maintain balance and orientation
To detect sound frequencies
To transmit nerve impulses
What do the semicircular canals provide information about?
Sound frequency
Rotational movement
Linear movement
Posture
Which two chambers are part of the vestibular apparatus?
Utricle and Saccule
Base and Apex
Cochlea and Cristae
Tympanic and Auditory
What type of information does the vestibular system send to the brain?
Information about temperature
Information about sound waves
Information about acceleratory movement
Information about light
What is the function of the organ of Corti?
It stabilizes balance
It transmits sound waves
It is the receptor for hearing
It vibrates in response to pressure
What do sensory hair cells in the cochlea do?
They stimulate nerves that carry sound messages to the brain
They stabilize balance
They vibrate in response to sound waves
They transmit electrical impulses directly
What is the primary function of the utricle and saccule?
To transmit sound waves
To stabilize vision
To detect sound frequencies
To detect linear acceleration
What does the diagram of the cochlea illustrate?
The process of hearing in the brain
How different frequencies of sound waves stimulate different parts of the cochlea
The structure of the tympanic membrane
The function of the semicircular canals
What transmits information about the speed and direction of head movement to the brain?
Maculae
Hair cells
Semicircular canals
Vestibule
What are common manifestations of vestibular disorders?
Hearing loss
Nausea
Tinnitus
Vertigo or ataxia
Which sensory areas in the inner ear contribute to our sense of balance?
Cochlea and utricle
Auditory and visual systems
Semicircular canals and vestibule
Maculae and cristae
What is the role of the vestibular system in maintaining balance?
Processes auditory signals
Integrates sensory information for balance
Controls vision
Regulates heart rate
Which systems contribute to maintaining balance?
Endocrine, muscular, skeletal
Respiratory, circulatory, digestive
Nervous, immune, reproductive
Vestibular, visual, auditory, proprioceptive
What are the tiny hairs that project into the mucous layer of the nose called?
Olfactory bulbs
Odour molecules
Nerve cells
Cilia
Where do the olfactory nerve signals transmit after the olfactory bulb?
Limbic system
Spinal cord
Thalamus
Frontal cortex
What is the role of the limbic system in relation to smell?
Conscious perception of smell
Responsible for emotion
Transmitting signals to the olfactory bulb
Stimulating odour molecules
How many nerve cells are approximately in the olfactory regions?
About 5 million
About 10 million
About 1 million
About 2 million
What does the olfactory bulb transmit signals to?
Other areas deeper in the brain
The spinal cord
The nasal cavity
The throat
What plays a central role in the perception of taste?
Sight
Hearing
Touch
Smell
Where are taste buds primarily located?
In the tonsils
On the surface of the tongue
On the palate
In the throat
How many taste buds are approximately found in the mouth?
Around 15,000
Around 10,000
Around 5,000
Around 20,000
What do the tiny hairs on taste buds respond to?
Colors
Flavours
Textures
Temperatures
What is stimulated when food or drink is consumed?
Taste cells
Touch receptors
Smell cells
Visual receptors
What is the role of saliva in taste perception?
It cools the mouth
It dissolves food and drink
It absorbs flavors
It enhances smell
What type of nerve cells are found in taste buds?
Temperature receptors
Pressure receptors
Pain receptors
Taste-detecting nerve cells
What do taste cells transmit to the brain?
Impulses
Colors
Flavors
Textures
What is depicted in the diagram of the tongue?
Taste receptors only
Taste buds and their anatomy
Taste regions
Saliva glands
What is Otitis Media with Effusion (OME) commonly known as?
Ear Infection
Middle Ear Syndrome
Glue Ear
Swimmer's Ear
What is a significant risk factor for developing OME in children?
Parents who smoke
Lack of exercise
Excessive screen time
High sugar diet
What anatomical feature makes children more susceptible to middle ear disease?
Thicker ear drum
Longer Eustachian tubes
Shorter Eustachian tubes
More vertical Eustachian tubes
What is a potential consequence of untreated OME in children?
Permanent middle ear damage
Enhanced speech
Improved hearing
Increased balance
What characterizes the pathology of OME?
Fluid accumulation in the outer ear
Acute infection
Chronic mucosal inflammation
Thickening of the ear drum
What type of fluid accumulation is associated with OME?
Serum
Mucous
Blood
Pus
Why is early recognition and treatment of OME important?
To prevent impairment of development
To avoid ear surgery
To enhance hearing ability
To reduce allergies
What does the diagram in Figure 8 illustrate?
Earwax buildup
Eardrum rupture
Middle ear infection
Differences in Eustachian tubes with age
What is a symptom of poor auditory function in children?
Enhanced educational progress
Improved listening skills
Delayed language development
Increased speech clarity
Which sign indicates fluid in the middle ear?
Normal hearing test
Dull appearance with radial vessels visible on the tympanic membrane
Visible earwax
Clear tympanic membrane
What test can elucidate conductive deafness?
Audiometry
CT scan
Tuning fork tests
Blood test
What is a treatment option for children with persistent bilateral OME?
Insertion of ventilation tubes (Grommets)
Hearing aids
Physical therapy
Antibiotics
What is a common symptom associated with recurrent ear infections?
Poor educational progress
Strong balance
High academic achievement
Excellent listening skills
What does a flat impedance curve on tympanograms indicate?
Possible middle ear dysfunction
Normal ear function
Inner ear damage
Excessive earwax
What can cause balance problems and clumsiness in children?
Strong muscles
Fluid in the middle ear
Good vision
High intelligence
What is a sign of conductive deafness during testing?
Visible fluid in the outer ear
Clear hearing on audiometry
Normal drum movement
Immobile drum on testing with pneumatic speculum
What is the definition of Acute Otitis Media (AOM)?
Infection of the inner ear.
Acute inflammation of the middle-ear cavity with infection.
Inflammation of the throat.
Chronic inflammation of the outer ear.
What percentage of children have had Acute Otitis Media by 2 years of age?
80%
50%
90%
70%
Which virus is commonly associated with Acute Otitis Media?
HIV
Zika virus
Respiratory syncytial virus
Ebola virus
What is the most common bacterial cause of Acute Otitis Media?
Haemophilus influenzae B
Escherichia coli
Streptococcus pneumoniae
Moraxella catarrhalis
Which bacteria accounts for 25% of Acute Otitis Media cases?
Streptococcus pneumoniae
Haemophilus influenzae B
Staphylococcus aureus
Moraxella catarrhalis
What is a common precursor to Acute Otitis Media?
Earwax buildup
Upper respiratory tract infection (U.R.T.I.)
Allergic rhinitis
Chronic sinusitis
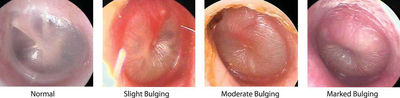
What is indicated by a bulging tympanic membrane?
Otitis media with effusion
Chronic otitis externa
Earwax blockage
Normal tympanic membrane
What part of the ear is affected by Acute Otitis Media?
Inner ear
Outer ear canal
Middle ear cavity
Eustachian tube
What is the first step in the inflammatory process leading to tympanic membrane perforation in ASOM?
Oedema closes the Eustachian Tube
Organisms invade mucous membrane
Desquamation perforation
Bulging of drum, loss of landmarks
Which antibiotic is the drug of choice for treating acute otitis media?
Penicillin
Co-amoxiclav
Amoxicillin
Ibuprofen
What should be done if otorrhoea persists after the acute phase of ASOM?
Continue antibiotics
Administer analgesia
Send a specimen for C & S
Perform myringotomy
What is a common underlying condition associated with recurrent episodic Acute Otitis Media?
Asthma
Trisomy 21
Diabetes
Cleft lip
What is the purpose of grommet insertion in children with recurrent attacks of otitis media?
To treat existing infections
To improve hearing
To break the sequence of recurrent attacks
To prevent tympanic membrane perforation
What is the recommended treatment for a child under 2 years old with acute otitis media?
Analgesia only
Direct to antibiotics
Steroid treatment
Observation for 72 hours
What symptom indicates persistent acute otitis media requiring hospital admission?
Bulging drum with severe symptoms
Clear ear discharge
Fever without ear discharge
Mild ear pain
What is a common cause of recurrent acute otitis media?
Lack of exercise
Underlying immunological defect
Exposure to cold weather
Poor diet
What is the recommended duration of antibiotic treatment for acute otitis media?
Two weeks
Three days
Five days
One week
What is chronic suppurative otitis media (C.S.O.M.) characterized by?
Fluid accumulation without perforation
Normal tympanic membrane appearance
A perforated tympanic membrane with persistent drainage for more than 2-6 weeks
Sudden hearing loss
What are common risk factors for chronic suppurative otitis media?
History of multiple episodes of acute otitis media
Living in isolated conditions
Single child family
No previous ear infections
What is a key feature of chronic suppurative otitis media?
Thickening of the tympanic membrane
Absence of any drainage
Tympanic membrane perforation, usually centrally located
Complete blockage of the Eustachian tube
What can trigger recurrent infections in C.S.O.M.?
Swimming in pools
Exposure to loud noises
High altitude changes
Upper respiratory tract sepsis via the Eustachian Tube
What can occur during a period of quiescence in C.S.O.M.?
Severe pain
Hearing loss
Complete recovery
Fever
Which image shows a normal tympanic membrane?

What can cause tympanic membrane perforation besides C.S.O.M.?
Trauma and previous grommet insertion
Earwax buildup
Cold weather exposure
High altitude flying
What imaging studies are recommended to assess the extent of CSOM disease?
CT or MRI
X-ray
Ultrasound
PET scan
What is a key component of CSOM treatment?
Intravenous fluids
Frequent aural toilet (microsuction)
Oral antibiotics
Corticosteroid injections
What procedure is performed if CSOM treatment fails?
Myringotomy
Tympanomastoidectomy
Cochlear implant
Tympanoplasty
Who is most commonly affected by nasopharyngeal angiofibroma?
Elderly males
Teenage males
Children
Adult females
What symptom is commonly associated with nasopharyngeal angiofibroma?
Prolonged recurrent epistaxis
Chronic cough
Sore throat
Hoarseness
What is the main treatment for enlarging nasopharyngeal angiofibroma?
Antibiotics
Observation
Surgery
Chemotherapy
What imaging technique is used to confirm the presence of angiofibroma?
X-ray
Endoscopy
Ultrasound
CT or MRI scan
What can occur due to the aggressive nature of angiofibroma?
Development of ulcers
Formation of cysts
Erosion of bone
Calcification of tissues
What are adenoids a component of?
Lingual tonsils
Waldeyer's ring of lymphoid tissue
Eustachian tube
Palatine tonsils
What can enlarged adenoids cause?
Chronic cough
Ear infections
Throat swelling
Nasal airway obstruction
What is a common cause of acute tonsillitis?
Staphylococcus
Streptococcus
Influenza virus
E. coli
Which symptom is NOT associated with enlarged adenoids?
Mouth breathing
Nasal congestion
Snoring
Sore throat
What is a common indication for adenoidectomy?
Chronic cough
Earwax buildup
Chronic mouth breathing
Nasal polyps
What can chronic mouth breathing lead to?
Increased appetite
Weight gain
Improved speech
Palatal and dental abnormalities
What age group is most affected by acute tonsillitis?
Teenagers
Elderly
Children under 9
Adults
What symptom might small children exhibit instead of sore throat?
Nasal congestion
Excessive sleeping
Loud crying
Refusal to eat
What is a common symptom of tonsillitis in infants?
Pyrexia
Nasal congestion
Halitosis
Coughing
What is the first choice analgesia for adults with tonsillitis?
Aspirin
Ibuprofen
Naproxen
Paracetamol
What is the antibiotic of choice for severe tonsillitis?
Erythromycin
Amoxicillin
Ciprofloxacin
Penicillin V
How many episodes of tonsillitis in one year indicate tonsillectomy?
10 episodes
7 episodes
5 episodes
3 episodes
What is a complication of recurrent tonsillitis?
Ear infection
Chronic cough
Tonsillectomy
Dehydration
What is a sign of follicular tonsillitis?
Fever
Swollen lymph nodes
Enlarged and hyperaemic tonsils
Sore throat
What should patients with tonsillitis do to prevent dehydration?
Only drink soda
Drink large amounts of juice
Avoid fluids
Drink as much as possible
What condition may cause halitosis?
Flu
Cold
Tonsillitis
Sinusitis
What is a characteristic feature of the pharyngeal mucosa in tonsillitis?
Dryness
Inflammation
Bleeding
Swelling
What is a visual sign of acute follicular tonsillitis?
Normal-sized tonsils
White patches on the tongue
Enlarged, red tonsils with exudate
Small, pale tonsils
What is the first choice analgesia for children with tonsillitis?
Paracetamol
Aspirin
Ibuprofen
Codeine
What is a common symptom of acute mastoiditis?
Nausea
Ringing in the ears
Mild headache
Persistent and severe pain
Which sign is associated with acute mastoiditis?
Tenderness of the mastoid on palpation
Fever
Swollen lymph nodes
Clear nasal discharge
What is a possible complication of acute mastoiditis?
Sinusitis
Subperiosteal abscess over the mastoid antrum
Earwax buildup
Tonsillitis
What is the recommended treatment for acute mastoiditis?
Topical ointments
Home rest
Oral pain relievers
IV antibiotics (Amoxicillin, Metronidazole)
What does the swelling of the post auricular region indicate?
Allergic reaction
Acute mastoiditis
Chronic otitis media
Ear canal infection
What is the appearance of the mastoid region in acute mastoiditis?
Pale and cold
Clear and normal
Dry and flaky
Swollen and erythematous
What can happen to the pinna in acute mastoiditis?
It may shrink in size
It may turn blue
It may become detached
It may be pushed forward and downwards
What is a Bezold abscess?
Swelling of the jaw
Pus breaks through the mastoid tip and passes into the neck
Fluid accumulation in the ear
Infection of the throat
In which age group does acute mastoiditis occur most frequently?
Adults
Elderly
Children
Infants
What is a common indication for performing a cortical mastoidectomy?
Presence of a periosteal abscess
Severe headache
Nasal congestion
Hearing loss
What symptom indicates an emergency referral for a sore throat?
Stridor and respiratory difficulty
Sore throat
Cough
Mild fever
What is the typical duration for mouth ulcers to resolve?
7-10 days
2 weeks
1 month
1-3 days
Which of the following is NOT a nutritional deficiency associated with mouth ulcers?
Folic acid
Iron
Vitamin D
Vitamin B12
Which condition is associated with recurrent mouth ulcers?
HIV
Leukaemia
Recurrent Aphthous Stomatitis (RAS)
Chicken Pox
What are the characteristics of oral cavity ulceration?
Lesions with pus
Small painful, shallow and round/oval lesions
Painless lesions
Large deep lesions
Which of the following is a potential infective cause of mouth ulcers?
Crohn's disease
Herpetic Stomatitis
Behcet's disease
Anemia
What is the source of the image depicting mouth ulcers?
A diagram of a throat
A close-up of a tongue with a white ulcer
An x-ray of the jaw
A photograph of a healthy mouth
What is a common cause of mouth ulcers related to cutaneous diseases?
Lupus Erythematous
Mucosal SCC
Denture
Sharp tooth
Which investigation is first line for suspected malignancy in mouth ulcers?
B12 and Folate
Iron studies
FBC
Biopsy
What is a common treatment for mouth ulcers?
Mouth Wash
Radiation
Surgery
Antibiotics
What is the primary aetiology of pharyngitis?
Allergy
Bacterial infection
Neoplasia
Viral infection
Which bacteria is most commonly associated with bacterial pharyngitis?
Escherichia coli
Group A Streptococci
Haemophilus influenzae
Staphylococcus aureus
What symptom is associated with acute tonsillitis and pharyngitis?
Headache
Nausea
Chest pain
Throat pain
What is a common symptomatic treatment for mouth ulcers?
Radiation therapy
Topical steroids
Chemotherapy
Surgery
What symptom is less likely in Group A Strep compared to Viral Pharyngitis?
Vomiting in children
Cough
Sore throat
Fever
What is the score range indicating a 1%-2.5% risk of Streptococcal Infection?
1
2
≤0
3
Which age group receives a score of 1 in the Centor Criteria?
0-2 yr
15-44 yr
45 yr or older
3-14 yr
What is the suggested management for a score of 3 in the Centor Criteria?
Culture all
No further testing
Perform culture
Treat empirically with antibiotics
What is a common symptom of both Group A Strep and Viral Pharyngitis?
Sore throat
Fever
Days of cough/rhinorrhoea
Vomiting in children
What does a score of ≥4 indicate in the Centor Criteria?
11%-17%
51%-53% risk of Streptococcal Infection
1%-2.5%
5%-10%
What are the complications of Group A Streptococcus (GAS) pharyngitis?
Laryngitis and epiglottitis
Rheumatic fever and glomerulonephritis
Pneumonia and bronchitis
Sinusitis and otitis media
What is the sensitivity of rapid streptococcal tests for diagnosing GAS pharyngitis?
Approximately 75%
Approximately 95%
Approximately 100%
Approximately 85%
What is the recommended sampling technique for rapid streptococcal tests?
Gentle samples from the uvula
Swabbing the soft palate only
Vigorous samples of both tonsils and posterior pharynx
Only anterior tonsil samples
What is the typical duration for symptoms of GAS pharyngitis to resolve spontaneously?
5-7 days
1 week
1-2 days
3-4 days
What is the main treatment approach for infectious mononucleosis?
Chemotherapy
Antibiotics
Supportive care
Surgery
Which virus is primarily responsible for infectious mononucleosis?
Cytomegalovirus (CMV)
Herpes Simplex Virus (HSV)
Epstein Barr Virus (EBV)
Human Immunodeficiency Virus (HIV)
What should be avoided in the treatment of infectious mononucleosis due to the risk of rash?
Aspirin
Amoxicillin
Penicillin
Ibuprofen
What is a common non-infectious cause of pharyngitis?
Mouth-breathing due to nasal obstruction
Bacterial infection
Allergy
Viral infection
What symptom is commonly associated with mouth-breathing pharyngitis?
Ear pain
Nasal congestion
Persistent cough
Sore throat worse in the morning
What is a key symptom of infectious mononucleosis?
Chest pain
Marked fatigue
High fever
Joint pain
What is shown in the image related to glandular fever?
Red throat without exudate
Swollen lymph nodes
Normal tonsils
Heavy exudate over entire tonsils
What is a Quinsy?
A peritonsillar abscess
A throat infection
A viral illness
A type of tonsillitis
Which symptom is NOT typically associated with a peritonsillar abscess?
Referred otalgia
Severe dysphagia
Trismus
Foetor
What is a common treatment for a peritonsillar abscess?
Rest and hydration
Cold compresses
Surgery immediately
Antibiotics
What may require drainage in a peritonsillar abscess?
Presence of trismus
Mild sore throat
Normal tonsil size
Absence of fever
What medication is suggested for treating a peritonsillar abscess?
Co-amoxiclav IV
Ibuprofen
Amoxicillin only
Ciprofloxacin
What is a sign of a peritonsillar abscess?
Enlarged lymph nodes
Fever only
Swollen uvula
Medial displacement of the tonsil
How is a peritonsillar abscess generally diagnosed?
Clinical examination
X-ray
Blood test only
MRI
What is the typical age group for a peritonsillar abscess?
Adults
Elderly
Children
Infants
What is one of the symptoms of a peritonsillar abscess?
Lymphadenopathy
Cough
Nausea
Rash
What is the recommended course of antibiotics for a peritonsillar abscess?
Five-day course of oral antibiotics
Only topical antibiotics
One-day course
Ten-day course
What is epiglottitis primarily characterized by?
Acute inflammation in the supraglottic region
Infection of the nasal passages
Chronic inflammation of the lungs
Inflammation of the stomach lining
What is a common position for a patient with epiglottitis?
Leaning to the side
Sitting back in a chair
Lying flat
Tripod position
Which organism is classically associated with epiglottitis in children?
Haemophilus influenzae type b
Staphylococcus aureus
Streptococcus pneumoniae
Escherichia coli
What is a late finding indicating advanced airway obstruction in epiglottitis?
Stridor
Drooling
Cough
Fever
What is the immediate management for an unstable patient with epiglottitis?
Intubation or tracheostomy
Nebulized steroids
Oral antibiotics
IV fluids
What percentage of adult epiglottitis cases are caused by Haemophilus influenzae?
25%
10%
50%
15%
What treatment is given to stable patients with epiglottitis?
Intranasal decongestants
IV steroids and antibiotics
Topical antiseptics
Oral pain relief
What physical finding involves a patient sitting up with their tongue out?
Fowler's position
Supine position
Tripod position
Lateral recumbent position
What is a common symptom of epiglottitis that indicates respiratory distress?
Hypoxia
Fatigue
Nausea
Headache
What should patients suspected of having epiglottitis be referred for?
ENT evaluation
Routine check-up
Blood tests
X-ray imaging
What is the most common cause of sore throat?
Allergic reactions
Viral infections
Bacterial infections
Throat cancer
Which bacteria is a common cause of bacterial pharyngitis?
Group A strep
Escherichia coli
Streptococcus pneumoniae
Staphylococcus aureus
What is a classic symptom of a peritonsillar abscess?
Fever
Sore throat
Cough
Hot potato voice
What does the Modified CENTOR Criteria assess?
Severity of pain
Type of bacteria
Risk of streptococcal infection
Presence of fever
What is the recommended treatment for a confirmed streptococcal infection?
Dexamethasone
Penicillin V
Ibuprofen
Clarithromycin
What complication can arise from untreated streptococcal pharyngitis?
Diabetes
Heart attack
Stroke
Rheumatic fever
Which condition is characterized by a grey membrane in the throat?
Thyroiditis
Quinsy
Diphtheria
Epiglottitis
What is a common analgesic recommended for sore throat?
Paracetamol
Codeine
Aspirin
Ibuprofen
What is the primary investigation for throat issues?
X-ray
Throat swab
Blood test
CT scan
What is a severe sign of sore throat requiring immediate attention?
Sore throat
Mild fever
Nausea
Airway compromise
What should be done if pus is drained from a peritonsillar abscess?
Start antibiotics
Admit and refer to ENT
Schedule a follow-up
Discharge immediately
What is a key symptom of epiglottitis?
Hoarse voice
Severe headache
Nasal congestion
Coughing
What is a sign of infectious mononucleosis?
Fever
Sore throat
Lymphadenopathy
Cough
What is the first-line treatment for a patient with a severe sore throat and suspected EBV?
Paracetamol
Benzylpenicillin
Clarithromycin
Ibuprofen
What should be prepared for a patient with airway compromise?
Difficult airway trolley
Pain relief
Antibiotics
IV fluids
What is the purpose of the flow chart in the management of sore throat?
To guide treatment decisions
To summarize symptoms
To diagnose all conditions
To list medications
What is a common non-suppurative complication of streptococcal infection?
Sinusitis
Glomerulonephritis
Quinsy
Otitis media
What is the age factor in the Modified CENTOR Criteria?
Age 30-44 years +1
Age < 20 years +1
Age > 65 years +2
Age > 44 years -1
What is a common symptom of laryngeal pathology?
Sore throat
Coughing
Dysphonia
Hoarseness
What should be done if dysphonia persists for more than 3 weeks?
Prescribe antibiotics
Advise voice rest
Refer to ENT specialist
Perform a laryngoscopy
What is the main treatment for acute laryngitis?
Conservative treatment
Radiation therapy
Antibiotics
Surgery
What is a contributing factor to chronic laryngitis?
Allergies
Smoking
Hydration
Viral infections
What is the role of speech therapy in chronic laryngitis?
Increase vocal range
Re-educate correct voice use
Cure the infection
Improve lung capacity
Which condition can present with laryngeal complications in up to 30% of patients?
Hypertension
Asthma
Diabetes
GORD
What should be assessed during the examination of a patient with dysphonia?
Risk factors for malignancy
Family history of allergies
Previous surgeries
Travel history
What is the purpose of the flowchart in the diagnosis of dysphonia?
Show treatment options
List medications
Provide patient education
Illustrate differential diagnosis
What is a cholesteatoma?
A type of ear infection
A cystic mass lined with keratin in the middle ear
A fluid-filled sac in the outer ear
A benign tumor in the ear canal
What percentage of cholesteatomas are congenital?
10-15%
1-3%
5-10%
2-5%
What are common presentations of cholesteatoma?
Nasal congestion, sore throat, cough
Otalgia, otorrhoea, deafness
Dizziness, tinnitus, ear ringing
Headaches, facial swelling, fever
What can advanced cholesteatoma cause?
Eustachian tube dysfunction
Hearing improvement
Facial nerve paralysis
Sinus infection
What are the two types of acquired cholesteatoma?
Chronic and acute
Simple and complex
Mild and severe
Primary and secondary
What is a possible complication of cholesteatoma?
Otitis externa
Earwax blockage
Mastoiditis
Tinnitus
What is a primary cause of cholesteatoma?
Earwax buildup
Retraction pocket on tympanic membrane
Allergic rhinitis
Acute otitis media
What is one theory regarding the pathogenesis of cholesteatoma?
Trapping of desquamation material in retraction pockets
Increased earwax production
Viral infection
Allergic reaction
What can advanced cholesteatoma lead to in terms of hearing?
Temporary hearing loss
Complete deafness
Reduced hearing due to ossicular involvement
Improved hearing
What is a common imaging finding in cholesteatoma?
Absence of the cochlea
Fluid in the outer ear
Cystic mass in the middle ear
Thickened tympanic membrane
What is a potential serious infection associated with cholesteatoma?
Sinusitis
Bronchitis
Pharyngitis
Meningitis
What is the histopathological feature of cholesteatoma?
Cystic mass lined with keratin producing squamous epithelium
Fluid-filled sac with no epithelium
Cystic mass with only lymphocytes
Solid mass of connective tissue
What are the components of the cholesteatoma perimatrix?
Epithelial cells and lymphocytes
Only keratinocytes
Fibroblasts, macrophages and capillaries
Osteoblasts and osteoclasts
Which bacteria are commonly associated with aerobic superinfection in cholesteatoma?
E. coli, Klebsiella, Bacillus
Streptococcus, Enterococcus, Clostridium
Bacteroides, Fusobacterium, Peptococcus
Pseudomonas, Staphylococcus, Proteus
What is the mainstay surgical procedure for cholesteatoma treatment?
Mastoidectomy
Myringotomy
Fistula repair
Tympanoplasty
What is a conservative management option for patients unfit for cholesteatoma surgery?
Regular microsuction to remove keratin and debris
Radiation therapy
Antibiotic therapy
Corticosteroid injections
What can enhance the biologic profile of the cholesteatoma perimatrix?
Superinfection
Cholesterol reduction
Surgical intervention
Antibiotic treatment
What is one of the treatment options for bacterial superinfection in cholesteatoma?
Ciprofloxacin
Vancomycin
Amoxicillin
Azithromycin
What is a consequence of the cholesteatoma perimatrix secreting metalloproteinases?
Bone erosion
Decreased inflammation
Increased infection resistance
Bone formation
What are the two main categories of complications arising from middle ear disease?
Intratemporal and Intracranial
Localized and Systemic
Mild and Severe
Acute and Chronic
Which of the following is a sequela of middle ear disease?
Tinnitus
Nasal congestion
Hearing loss
Throat pain
What is one of the clinical features of labyrinthitis?
Ear pain
Vertigo
Ringing in the ears
Fever
What is a common treatment for labyrinthitis?
Antibiotics
Surgery
Pain relievers
Decongestants
Which complication involves the 5th cranial nerve?
Facial nerve paralysis
Petrositis
Mastoiditis
Labyrinthitis
What is a sign of labyrinthitis?
Hearing loss
Facial swelling
Ear discharge
Nystagmus towards the diseased side
What are common systemic effects of subdural/extradural abscesses?
Dizziness
Nausea
Fatigue
Pyrexia
Malaise
Which of the following is a raised intracranial pressure symptom?
Tinnitus
Nausea
Fatigue
Headache
What is the management for subdural/extradural abscess?
Physical therapy
IV Antibiotics and surgical intervention
Oral antibiotics only
Observation only
What should alert a clinician to the possibility of a tumor in facial nerve palsy?
Facial twitching
Ear pain
New onset parotid lump
Headache
What grading system is used for facial nerve dysfunction?
Wong-Baker FACES
Bristol Stool Chart
House Brackmann
Glasgow Coma Scale
What is the most common cause of facial nerve palsy?
Tumor
Trauma
Infection
Idiopathic (Bell's Palsy)
Which type of facial nerve palsy spares the forehead?
Lower motor neuron
Complete paralysis
Partial paralysis
Upper motor neuron
What is a possible aetiology for upper motor neuron palsy?
Bell's Palsy
Mastoiditis
Vascular e.g. aneurysm
Herpes virus
What does a progression beyond 3 weeks or lack of improvement beyond 6 months suggest?
viral infection
bacterial infection
benign condition
malignant cause
Which condition is associated with hearing loss in Ramsay Hunt syndrome?
Meniere's disease
Acoustic neuroma
otitis media
Bell's palsy
What comorbidity is noted to predispose to infection?
Obesity
Asthma
Diabetes
Chronic kidney disease
Which neurological infections can affect the facial nerve?
tuberculosis
HIV
syphilis
meningitis
What is an important consideration for eye care in facial nerve palsy?
eye patching all day
daily eye drops
use of artificial tears
avoidance of light
What is the initial treatment recommended for facial nerve palsy?
antibiotics
high dose steroid
physiotherapy
surgery
Which grading system is used to track facial nerve palsy recovery?
Glasgow Coma Scale
Fugl-Meyer Assessment
Barthel Index
House Brackmann system
What should be done if no resolution occurs after 3 weeks?
consider referral to ENT
perform surgery
start chemotherapy
discontinue treatment
What is the most common form of otitis externa (OE)?
Chronic OE
Necrotizing OE
Otomycosis
Acute diffuse OE
Which type of otitis externa is associated with infection of a hair follicle?
Eczematous OE
Acute localized OE (furunculosis)
Acute diffuse OE
Chronic OE
What is a key characteristic of necrotizing (malignant) otitis externa?
Most common in swimmers
Infection extends into deeper tissues
Caused by fungi
Associated with atopic dermatitis
Which organism is commonly associated with otitis externa?
Streptococcus pneumoniae
Pseudomonas aeruginosa
Staphylococcus aureus
Escherichia coli
What symptom is commonly observed in otitis externa?
Severe headache
Nausea
Hearing loss
Itching progressing to pain
What type of otitis externa encompasses various dermatologic conditions?
Acute localized OE
Eczematous (eczematoid) OE
Acute diffuse OE
Necrotizing OE
What is a common diagnostic step for otitis externa?
CT scan of the brain
Swab for culture and sensitivity
X-ray of the skull
Blood test for allergies
Which condition is a fungal infection of the ear canal?
Otomycosis
Chronic OE
Acute diffuse OE
Eczematous OE
What is a common finding in the ear canal during examination of otitis externa?
Pus-filled cysts
Diffuse erythema and edema
Presence of wax
Clear fluid
What is the purpose of topical steroids in the treatment of otitis externa?
To reduce oedema
To dry the ear
To treat fungal infections
To numb the pain
Which medication is effective against Pseudomonas aeruginosa?
Ciprofloxacin
Clotrimazole
Gentamicin
Neomycin
What should patients avoid doing while treating otitis externa?
Using cotton buds in the ear
Applying topical antibiotics
Keeping the ear dry
Wearing ear plugs
Which drug is known to cause dose-related deafness if the tympanic membrane is perforated?
Ciprofloxacin
Aminoglycosides
Dexamethasone
Hydrocortisone
What is the role of ENT in severe cases of otitis externa?
Micro suction and cleaning under the microscope
Providing topical treatments
Performing surgery
Prescribing oral antibiotics
What is malignant otitis externa (MOE)?
A rare potentially fatal inflammatory disease of the external auditory canal
A benign growth in the ear
A common ear infection
A type of skin cancer
Which patients are most commonly affected by malignant otitis externa?
Immunocompromised or diabetic patients
Elderly patients only
Healthy individuals
Children under 5 years
What are the common symptoms of malignant otitis externa?
High fever, granulation tissue in EAC, severe pain
Nasal congestion
Mild earache, no fever
Sore throat
What is a major complication of malignant otitis externa?
Otitis media
Tinnitus
Sinusitis
Meningitis
How is malignant otitis externa diagnosed?
Blood pressure measurement
X-ray only
Physical examination alone
Otoscopy, elevated ESR, CT or MRI
What is the emergency treatment for malignant otitis externa?
IV antibiotics +/- surgical debridement
Oral painkillers only
No treatment needed
Topical antibiotics only
What is the aetiology of furunculosis in the external auditory meatus?
Fungal infection
Viral infection
Staphylococcus aureus infection of a hair follicle
Bacterial infection from swimming
What can nasal furunculosis lead to if not treated properly?
Allergic rhinitis
Facial cellulitis and cavernous sinus thrombosis
Earwax buildup
Nasal congestion
What are the symptoms of nasal furunculosis?
Sore throat
Nasal bleeding
Pain, erythema, and oedema
Itching and dryness
What is a common treatment for furunculosis?
Antihistamines
Systemic anti-staphylococcus antibiotics – penicillin
Corticosteroids
Topical antifungals
What is a common cause of traumatic tympanic membrane perforation?
Allergy
Barotrauma
Cold weather
Infection
Which of the following is a possible aetiology for tympanic membrane perforation?
Flu
Foreign bodies
Sinusitis
Earwax
What is a key diagnostic feature of traumatic tympanic membrane perforation?
Smooth edges
Clear fluid
No bleeding
Ragged edges
What type of trauma can lead to tympanic membrane perforation?
Scratching
Falling
Burning
Explosion
Which activity is associated with tympanic membrane perforation due to barotrauma?
Cooking
Water sports
Reading
Walking
What is a symptom of tympanic membrane perforation?
Nasal congestion
Sore throat
Evidence of recent haemorrhage
Coughing
What does figure 24 show?
A perforated tympanic membrane with blood
An ear infection
A foreign body in the ear
A healthy tympanic membrane
What may cause tympanic membrane perforation from a slap on the ear?
Infection
Barotrauma
Cold air
Dust
What is the first step in evaluating a patient with suspected ear perforation?
Performing a hearing test
Administering antibiotics
Scheduling surgery
Examination of the ear
What should be documented if the perforation is clearly seen during an ear examination?
Presence of infection
Size and shape of the perforation
Hearing level
Patient's age
What is a pathognomonic sign of a temporal bone fracture in a patient with a head injury?
CSF leakage
Hearing loss
Ear discharge
Facial nerve palsy
What is the recommended action if the tympanic membrane perforation is contaminated?
Wait for spontaneous healing
Ignore the contamination
Perform immediate surgery
Consider antibiotic treatment
What is the relationship between the size of a tympanic membrane perforation and healing?
Smaller perforations have a greater chance of healing
Size does not affect healing
All perforations heal equally
Larger perforations heal faster
What defines sudden onset sensorineural hearing loss?
Gradual loss of hearing over months
Loss of 10 decibels over one week
Complete hearing loss immediately
Loss of 30 decibels or more over three frequencies within three days
What is the incidence of sudden onset sensorineural hearing loss?
50 per 100,000
8 per 100,000
20 per 100,000
1 per 100,000
Which of the following is a potential infectious cause of sudden onset sensorineural hearing loss?
Diabetes
Acoustic neuroma
Herpes zoster
Multiple sclerosis
What type of hearing loss is defined as sudden onset sensorineural hearing loss?
Permanent hearing loss
Sensorineural hearing loss
Conductive hearing loss
Mixed hearing loss
What is a common treatment strategy for tympanic membrane perforation?
Use earplugs at all times
Keep water out of the ears
Perform self-cleaning of the ear
Apply heat to the ear
What should history focus on when evaluating hearing loss?
Various aetiologies including medications, recent trauma, and infections
Only medical history
Only medications
Only recent trauma
What is a key examination step for conductive hearing loss?
Otoscopy for conductive blockage
Vision test
Neurological examination
Physical examination of the throat
What type of investigation is performed on the day of presentation for hearing loss?
Blood glucose test
MRI of the brain
Audiogram
Hearing test with a tuning fork
Which tests are included in the haematological investigations?
Only FBC
Only Glucose
FBC, ESR, Glucose, HbA1c
Only HbA1c
What is the recommended steroid treatment for idiopathic sensory neural hearing loss?
1mg prednisolone/kg/day for 5 days
10mg prednisolone/kg/day for 10 days
1mg prednisolone/kg/day for 10 days
5mg prednisolone/kg/day for 5 days
What percentage of patients with sudden sensory neural hearing loss spontaneously recover?
25%
10%
50%
75%
What does improvement at 1-2 weeks indicate about hearing loss prognosis?
It guarantees full recovery
It indicates immediate surgery is needed
It does not affect prognosis
It may predict long-term prognosis
What is a caution when using high dose steroids in patients?
Elderly, diabetic, or those with a history of psychosis
Only in elderly
Only in diabetics
Only in pregnant women
What imaging is performed for suspected intracranial pathology?
CT scan of the chest
X-ray of the skull
Ultrasound of the head
MRI of brain and internal acoustic meatus
What is the significance of the audiogram in the treatment of hearing loss?
It is irrelevant to treatment
It shows improvement after steroid treatment
It only shows initial hearing loss
It indicates the need for surgery
What is an acoustic neuroma also known as?
Vestibular schwannoma
Acoustic sarcoma
Cochlear tumor
Neurofibroma
What percentage of intracranial tumors in adults does acoustic neuroma account for?
10%
8%
15%
5%
Which cranial nerve is affected by an acoustic neuroma?
5th cranial nerve
8th cranial nerve
7th cranial nerve
6th cranial nerve
What is a risk factor for developing an acoustic neuroma?
Neurofibromatosis 2 (NF2)
Hypertension
Asthma
Diabetes
What is a common symptom of acoustic neuroma?
Vision loss
Nausea
Asymmetrical sensorineural hearing loss
Memory loss
What examination method is used to test hearing in suspected cases of acoustic neuroma?
Endoscopy
Blood test
Tuning fork
CT scan
Which symptom involves hearing buzzing or repetitive sounds?
Headache
Tinnitus
Vertigo
Facial numbness
What imaging technique is used for diagnosing acoustic neuroma?
MRI Scan
Ultrasound
X-ray
CT scan
What is a red flag symptom for tinnitus that warrants referral to ENT?
Pulsatile tinnitus
Bilateral tinnitus
Chronic headache
Hearing loss
What is the prevalence of tinnitus in the adult population?
20%
10%
15%
5%
Which condition is associated with pulsatile tinnitus?
Meniere's
Vascular pathology
Acoustic trauma
Otosclerosis
What is a common non-troublesome cause of tinnitus?
Otosclerosis
Idiopathic tinnitus
Conductive hearing loss
Vestibular schwannoma
Which medication class is known to cause tinnitus?
Antidepressants
Antihistamines
Ototoxic drugs
Antibiotics
What should be examined in the tympanic membrane during a tinnitus assessment?
Shape of the ear
Color of the membrane
Identifiable cause of conductive hearing loss
Presence of wax
What is a psychosocial impact of tinnitus?
Sleep disturbance
Improved concentration
Hearing enhancement
Increased appetite
Which condition may be suggested by vertigo and sensory neural hearing loss with tinnitus?
Otosclerosis
Acoustic neuroma
Benign intracranial hypertension
Meniere's
What is the most common finding in audiograms related to hearing loss?
Age-related degeneration in hearing (high frequency)
Acoustic neuroma
Ear infection
Sudden hearing loss
What is a common treatment for tinnitus?
Antibiotics
Steroids
Sound therapy
Surgery
Which of the following is a peripheral cause of vertigo?
Migraine
Benign Paroxysmal Positional vertigo (BPPV)
Cerebellar stroke
Multiple sclerosis
What does the mnemonic S.P.I.N.D.A.R help examine?
Visual acuity
Cerebellar system
Hearing ability
Vestibular system
Which condition is characterized by excess fluid in the inner ear?
Meniere's Disease
Acoustic neuroma
BPPV
Labyrinthitis
What type of nystagmus is associated with central causes of vertigo?
Vertical nystagmus
Horizontal nystagmus
Rotatory nystagmus
No nystagmus
What is a common cause of vertigo following a viral infection?
Acoustic neuroma
Infection of the vestibular apparatus
Sinusitis
Middle ear infection
What is a symptom of Benign Paroxysmal Position Vertigo (BPPV)?
Hearing loss
Vertigo lasting for seconds
Severe headache
Vertigo lasting for hours
What does the HINTS mnemonic help assess in a cerebellar examination?
Balance disorders
Vestibulo-ocular reflex
Hearing loss
Nystagmus
What are the symptoms of Meniere's disease?
Nystagmus, vertigo, tinnitus
Dizziness, nausea, headaches, fatigue
Vertigo, tinnitus, hearing loss, aural fullness
Hearing loss only
What is the main treatment for acute attacks of Meniere's disease?
Vestibular sedatives
Hearing aids
Epley manoeuvre
Surgery
What is the cause of BPPV?
Dislodging of otoconia into semicircular canals
Vestibular neuritis
Inner ear infection
Migraine
What maneuver is diagnostic for BPPV?
Cover/uncover test
Dix Hallpike manoeuvre
HINTS test
Epley manoeuvre
What is the primary treatment for BPPV?
Betahistadine
Steroid injections
Vestibular sedatives
Epley manoeuvre
What lifestyle changes are recommended for managing Meniere's disease?
Reduce salt, caffeine, alcohol, and stop smoking
Consume more caffeine
Increase salt intake
Avoid exercise
What does a vertical movement of the eye during the cover/uncover test suggest?
Hearing loss
Normal vestibular function
Central cause of vertigo
Peripheral cause of vertigo
What is the most common cause of vestibular neuritis?
Bacterial infection
Herpes simplex virus
Allergic reaction
Fungal infection
What are common symptoms of vestibular neuritis?
Loss of smell, sore throat, ear pain
Headache, fever, rash
Acute-onset vertigo, nausea, vomiting
Chest pain, cough, fatigue
What is the primary treatment for vestibular neuritis?
Supportive care and vestibular inhibitors
Corticosteroids
Surgery
Antibiotics
What prevents nasal regurgitation of food during swallowing?
Contraction of the diaphragm
Closure of the vocal cords
Opening of the epiglottis
Elevation of the soft palate
How does the nasal cavity help in breathing?
Cleans and humidifies air
Reduces air temperature
Filters out carbon dioxide
Increases air pressure
What lines the respiratory surfaces in the nose and paranasal sinuses?
Simple squamous epithelium
Skin epithelium
Cuboidal epithelium
Respiratory mucous membrane
What is the role of the ciliated columnar epithelium in the nasal cavity?
To facilitate gas exchange
To absorb nutrients
To produce mucus
To help move mucus and debris out of the airways
What is the relationship between rhinitis and asthma?
Asthma only occurs in children
They are completely unrelated
Rhinitis is a symptom of asthma
They should be treated as a unified functional unit
What is Sinusitis?
An infection of the throat
Inflammation of the paranasal sinuses
A skin condition
A type of headache
What is the duration that defines acute Rhinosinusitis?
6 months
1 week
<blockquote>
12 weeks
</blockquote>
<12 weeks
Which of the following is NOT a type of Rhinosinusitis?
Vasomotor
Acute Infective
Allergic
Nasal polyposis
What is a common consequence of a viral common cold?
Acute rhinosinusitis
Sinus cancer
Chronic rhinosinusitis
Nasal polyps
Which condition can lead to primary ciliary abnormality?
Cystic fibrosis
Kartageners syndrome
Allergic rhinitis
Asthma
Which of the following is a clinical feature of Acute Rhinosinusitis?
Weight loss
Nasal congestion
Skin rash
Fever
What is a serious risk associated with Acute Rhinosinusitis?
Common cold
Life-threatening complications
Seasonal allergies
Nasal dryness
What is the one-year prevalence of Acute Rhinosinusitis?
1-5%
50-60%
20-30%
6-15%
What is the main reason for prescribing antibiotics in rhinosinusitis?
To treat viral infections
To alleviate allergies
To reduce inflammation
To manage bacterial infections
What are the paranasal sinuses illustrated in the provided diagram?
Frontal, ethmoid, sphenoid, and maxillary sinuses
Temporal and occipital sinuses
Nasal and oral sinuses
Cranial and thoracic sinuses
What is the location of pain related to in sinogenic pain?
Affected sinus
Ears
Throat
Nasal cavity
Where does sphenoid sinus pain radiate to?
Forehead
Nose
Cheeks
Vertex
Which sinusitis may radiate pain to the teeth?
Maxillary sinusitis
Sphenoid sinusitis
Ethmoidal sinusitis
Frontal sinusitis
What does frontal sinus pain typically present as?
At the vertex
Directly over the affected sinus
Radiating to the teeth
Near the eyes
How many symptoms are needed to diagnose rhinosinusitis?
Three symptoms
One symptom
At least two symptoms
Four symptoms
Which symptom is NOT part of the rhinosinusitis diagnosis criteria?
Cough
Blockage/congestion
Facial pain/pressure
Reduced sense of smell
What is a necessary sign for diagnosing rhinosinusitis?
Nasal bleeding
Fever
Endoscopic signs
Ear pain
What type of imaging is required to confirm sinusitis?
Ultrasound
X-ray
CT imaging
MRI
Where is pus or obstruction primarily found in rhinosinusitis?
Sphenoid sinuses
Middle meatus
Nasal passages
Frontal sinuses
What are mucosal changes in relation to in rhinosinusitis diagnosis?
Osteomeatal complex and/or sinuses
Throat
Nasal cavity
Ears
What does the diagram in Figure 27 illustrate?
Types of sinusitis
Referred pain patterns from different sinuses
Symptoms of rhinosinusitis
Anatomy of the sinuses
What symptom is associated with allergic rhinosinusitis but not infectious rhinosinusitis?
Sneezing
Discharge
Hyposmia
Congestion
Which type of rhinosinusitis may have colored discharge?
Neither type
Allergic rhinosinusitis
Infectious rhinosinusitis
Both types
What is a common treatment for bacterial rhinosinusitis?
Amoxicillin
Antihistamines
Nasal decongestants
Topical steroids
What type of hypersensitivity reaction is involved in allergic rhinitis?
Type 2
Type 4
Type 1
Type 3
Which of the following is NOT a common allergen for allergic rhinitis?
Pollutants
Pollen
House dust mites
Animal dander
What does the EPOS 2020 guidelines focus on regarding acute rhinosinusitis?
Home remedies for sinusitis
Surgical treatments for sinusitis
Management pathways for acute rhinosinusitis
Long-term medication for sinusitis
What is a recommended non-medical treatment for allergic rhinitis?
Take antihistamines
Use nasal sprays
Use decongestants
Remove bedroom carpeting
Which testing method is used to identify specific allergens in allergic rhinitis?
Skin prick testing
X-ray imaging
MRI scanning
Blood pressure testing
What should be done to bed clothes to manage dust mite allergies?
Use fabric softener
Dry clean only
Wash in cold water
Wash at greater than 60 degrees
What is one of the alarm symptoms for acute bacterial rhinosinusitis (ABRS)?
Sneezing
Severe headache
Itchy eyes
Mild congestion
What is one of the complications of acute rhinosinusitis?
Meningitis
Diabetes
Asthma
Hypertension
Which of the following is a surgical treatment indication for allergic rhinitis?
Mild symptoms
Unresponsive to medical treatment
Seasonal allergies
Nasal congestion
What type of abscess can occur as a complication of acute rhinosinusitis?
Lung abscess
Brain abscess
Liver abscess
Kidney abscess
According to ARIA guidelines, what should be considered in the management of allergic rhinitis?
Age of patient
Gender of patient
Severity of symptoms
Geographic location
Which complication of acute rhinosinusitis affects the eyes?
Glaucoma
Retinal detachment
Cataract
Periorbital cellulitis
What is a possible bone complication of acute rhinosinusitis?
Osteoporosis
Osteomyelitis
Rheumatoid arthritis
Bone fracture
What is represented in the flowchart related to allergic rhinitis management?
Diagnosis and management based on symptoms
Management of nasal polyps
Guidelines for sinus surgery
Treatment options for asthma
What is a nasal complication of acute rhinosinusitis?
Deviated septum
Nasal polyp
Septal perforation
Mucocele
What is periorbital cellulitis commonly caused by?
Dacryocystitis
Acute sinusitis
Trauma
Insect bites
What is a major risk associated with untreated post septal cellulitis?
Facial paralysis
Skin necrosis
Blindness
Hearing loss
Which imaging study is urgent in suspected post septal infection?
X-Ray
CT Scan
Ultrasound
MRI
What are the most common pathogens in periorbital cellulitis?
E. coli and Klebsiella
Staphylococci and Streptococci
Pseudomonas and Bacillus
Candida and Aspergillus
What symptoms suggest post septal cellulitis?
Nasal congestion
Reduced visual acuity
Sore throat
Cough
What is a common treatment for periorbital cellulitis?
Topical steroids
Cold compresses
Oral antihistamines
IV antibiotics
What is the significance of the lamina papyracea in periorbital cellulitis?
It prevents infection
It is a type of antibiotic
It is a surgical procedure
It allows direct spread of infection
Which symptom indicates possible optic neuritis?
Nasal bleeding
Reduced colour vision
Ear pain
Fever
What is a possible complication of untreated orbital cellulitis?
Cavernous sinus thrombosis
Diabetes
Hypertension
Asthma
In which demographic is periorbital cellulitis most common?
Children
Elderly
Infants
Adults
What is cavernous sinus thrombosis (CST)?
A type of brain tumor
An infection of the lungs
A stroke
Formation of a blood clot within the cavernous sinus
What are common presentations of cavernous sinus thrombosis?
Loss of vision
Sepsis
High fever
Nausea
Dizziness
Headaches
What is the mortality rate without antibiotics for cavernous sinus thrombosis?
80-100%
50-70%
20-30%
10-15%
What is a common treatment for cavernous sinus thrombosis?
Surgery
Physical therapy
Radiation therapy
Antibiotics
What anticoagulation therapy options are available for CST?
Clopidogrel and rivaroxaban
Enoxaparin and dabigatran
Unfractionated IV heparin and fractionated low-molecular-weight SC heparins
Warfarin and aspirin
What are the symptoms required for a diagnosis of chronic rhinosinusitis?
Nasal obstruction only
Only facial pain
Two or more symptoms including nasal blockage or discharge
Only reduction in smell
How long must symptoms be present to diagnose chronic rhinosinusitis?
6 weeks
Greater than 12 weeks
Less than 4 weeks
8 weeks
What percentage of the general population is affected by chronic rhinosinusitis?
15-20%
5-12%
1-3%
10-15%
What examination method is used for chronic rhinosinusitis?
Nasal endoscopy
Ultrasound
MRI
X-ray
What imaging technique is commonly used in the examination of chronic rhinosinusitis?
PET Scan
X-ray
MRI Scan
CT Scan
Which test may be performed if allergies are suspected in chronic rhinosinusitis?
Blood pressure test
Ultrasound
Skin prick test
X-ray
What does Functional Endoscopic Sinus Surgery (FESS) aim to achieve in chronic rhinosinusitis management?
Restitution of physiology
Only cosmetic improvement
Complete removal of sinuses
Permanent cure of all sinus issues
Which of the following is NOT a criterion for Functional Endoscopic Sinus Surgery (FESS)?
Creates a sinus cavity that incorporates the natural ostium
Allows adequate sinus ventilation
Facilitates instillation of topical therapies
Facilitates mucociliary clearance
What is one of the management steps for chronic rhinosinusitis outlined in the EPOS 2020 care pathways?
Only medication
Self-care
Avoiding all therapies
Immediate surgery
What does FESS facilitate for ongoing care in chronic rhinosinusitis?
Surgical intervention
Instillation of topical therapies
Long-term hospitalization
Use of antibiotics only
What is depicted in the flowchart for chronic rhinosinusitis management?
Historical treatment methods
Surgical techniques
Care pathways for CRS
Dietary recommendations
What is one of the rare inflammatory sinonasal diseases associated with systemic illness?
Epistaxis
Rhinorrhea
Saddle deformity
Granulomatosis with polyangiitis (Wegner's)
Which of the following is NOT a symptom of granulomatous sinonasal disease?
Saddle deformity
Crusting
Rhinorrhea
Congestion
What type of diagnostic test is used for suspected granulomatous sinonasal disease?
Ultrasound
Full blood count
MRI
Liver function tests
Which imaging technique is used in the workup for granulomatous sinonasal disease?
Chest X-Ray
MRI
CT scan of the abdomen
Ultrasound
What is a common symptom of granulomatous sinonasal disease?
Diarrhea
Fever
Mucosal oedema
Nausea
What type of biopsy is performed if the initial investigations are inconclusive?
Histological biopsy
Skin biopsy
Bone marrow biopsy
Liver biopsy
Which systemic organ is commonly affected by granulomatous diseases?
Heart
Lungs
Brain
Liver
What is one of the systemic investigations for granulomatous sinonasal disease?
Blood glucose
Vitamin D levels
ANCA
Thyroid function tests
What is a common nasal sign of granulomatous disease?
Septal perforation
Sinusitis
Nasal polyps
Allergic rhinitis
What does the diagnostic workup for granulomatous sinonasal disease include?
Lipid profile
Chest ultrasound
Urinalysis
Endoscopy
What is Granulomatous with Polyangiitis also known as?
Eosinophilic Granulomatosis
Wegener's
Churg Strauss Syndrome
Granulomatosis with Polyangiitis
What is a characteristic feature of Granulomatous with Polyangiitis?
Eosinophilia
Necrotising granulomas of the respiratory tract
Asthma
Pulmonary infiltrates
What is the mean age of incidence for Granulomatous with Polyangiitis?
30 years
50 years
60 years
40 years
What type of antibodies are associated with Granulomatous with Polyangiitis?
Anti Neutrophil Cytoplasmic Antibody (ANCA)
Anti-DNA Antibodies
Rheumatoid Factor
Anti Nuclear Antibody (ANA)
What percentage of patients with Granulomatous with Polyangiitis experience complete remission with treatment?
75%
90%
50%
65%
Which organ is involved in 20% of Granulomatous with Polyangiitis cases?
Lungs
Skin
Heart
Renal
What is one of the main treatments for Granulomatous with Polyangiitis?
Combination of Steroids + Cyclophosphamides
Radiation therapy
Antibiotics alone
Surgery
What is the triad of symptoms associated with Churg Strauss Syndrome?
Nasal congestion, sneezing, anosmia
Asthma, systemic vasculitis, eosinophilia
Fever, cough, fatigue
Chest pain, dyspnea, wheezing
What is the incidence rate of Churg Strauss Syndrome?
3-4/100,000
5-10/100,000
2-3/100,000
1-2/100,000
What percentage of Churg Strauss Syndrome patients present with nasal symptoms?
50%
90%
70%
80%
What is the definition of sarcoidosis?
A bacterial infection
A type of cancer
A multisystem inflammatory disease with noncaseating granulomas
An autoimmune disorder
What is the incidence rate of sarcoidosis?
30-35 per 100,000
10-15 per 100,000
20-25 per 100,000
5-10 per 100,000
Which demographic has a higher incidence of sarcoidosis?
Caucasians
Asians
Native Americans
Afro-Caribbeans and Scandinavians
What is a common presentation of sarcoidosis?
Nausea and vomiting
Pulmonary complaints like cough and dyspnoea
Headaches
Skin rashes only
What percentage of sarcoid patients experience sinonasal disease?
9%
5%
15%
20%
What treatment is commonly used for sarcoidosis?
Antibiotics
Surgery
Systemic steroids and immune suppression
Radiation therapy
What is a significant histological finding in sarcoidosis?
Caseating granulomas
Necrotising granulomas
Vasculitis
Eosinophilia
Which condition is associated with systemic lupus erythematosus?
Asthma
Chronic rhinosinusitis
Non-granulomatous sinonasal conditions
Nasal polyps
What is a common skin lesion associated with sarcoidosis?
Psoriasis
Acne
Lupus pernio
Eczema
What percentage of sarcoidosis cases are asymptomatic?
5%
20%
10%
15%
What is a potential immune dysregulation finding in sarcoidosis?
High neutrophils
Low T-cells
Decreased antibodies
Raised B-cells
Which age groups are most affected by sarcoidosis?
15-25 and 35-45
25-35 and 45-65
20-30 and 40-50
30-40 and 50-60
What type of granulomas are predominantly found in sarcoidosis?
Caseating granulomas
Noncaseating granulomas
Necrotising granulomas
Eosinophilic granulomas
What systemic complaint is experienced by 45% of sarcoidosis cases?
Headaches
Skin rashes
Joint pain
Fever and anorexia
What is a specific mucosal change associated with sarcoidosis?
Bleeding gums
Granulations and yellow submucosal nodules in the nose
Swelling of the tongue
Nasal congestion
Which of the following is a non-granulomatous sinonasal condition?
Behcet's disease
Chronic rhinosinusitis
Lupus pernio
Sarcoidosis
What is a characteristic feature of eosinophilia?
Decreased white blood cells
Increased neutrophils
Increased eosinophil count in blood
Decreased red blood cells
What is the treatment success rate for sarcoidosis with systemic steroids?
60%
50%
70%
Over 80%
Which systemic condition is NOT associated with sinonasal symptoms?
Behcet's disease
Relapsing polychondritis
NK-cell lymphoma
Lupus pernio
What is the main cause of immune dysregulation in sarcoidosis?
Viral infection
Genetic mutation
Bacterial infection
Unknown aetiology
What does the table in the document list?
Treatment options for sarcoidosis
Types of sarcoidosis
Symptoms of sarcoidosis
Non-granulomatous sinonasal conditions associated with systemic disease
What are the two types of epistaxis based on the location of the bleed?
Left and Right
Internal and External
Acute and Chronic
Anterior and Posterior
Which plexus is associated with anterior epistaxis?
Woodruff's plexus
Sphenopalatine plexus
Kiesselbach's plexus
Ophthalmic plexus
What is the common age distribution for epistaxis?
0 to 5 and 50 to 60 years
20 to 30 and 40 to 50 years
30 to 40 and 60 to 70 years
Younger than 10 and 70 to 79 years
What is the primary blood supply for Kiesselbach's plexus?
Branches from Internal Carotid artery
Branches from External Carotid artery
Branches from Subclavian artery
Branches from Brachiocephalic artery
Which condition is a traumatic cause of epistaxis?
Facial trauma
Hemophilia
Leukemia
Vitamin K deficiencies
What is a common infectious cause of epistaxis?
Polycythemia vera
Aplastic anemia
Thrombocytopenia
Sinusitis
Which of the following is a disorder of hemostasis that can cause epistaxis?
Environmental irritants
Hemophilia
Digital trauma
Upper respiratory infection
What is the most frequent treatment for anterior epistaxis?
General anaesthesia
Cautery under local anaesthesia
Nasal packing
Observation only
Which plexus is associated with posterior epistaxis?
Kiesselbach's plexus
Ophthalmic plexus
Woodruff's plexus
Sphenopalatine plexus
What is one of the major arteries supplying the nasal septum?
Brachiocephalic artery
Subclavian artery
Sphenopalatine artery
Facial artery
What is a common benign tumor that can cause epistaxis?
Metastatic lesions
Juvenile angiofibroma
Nasopharyngeal neoplasms
Benign nasal polyps
What is one of the treatments for posterior epistaxis?
Topical medications
Nasal packing
Cautery under local anaesthesia
Observation only
What is a contributing factor to epistaxis related to environmental exposure?
Aplastic anemia
Thrombocytopenia
Environmental irritants
Leukemia
What is a common age range for epistaxis to occur?
20 to 30 years
50 to 60 years
Younger than 10 and 70 to 79 years
30 to 40 years
What is the role of the greater palatine artery in epistaxis?
It supplies blood to the nasal septum
It is involved in nasal packing
It is a cause of epistaxis
It is used for cauterization
Which of the following is an infectious cause of epistaxis?
Leukemia
Trauma
Environmental irritants
Tuberculosis
What is the primary anatomical challenge in posterior epistaxis?
Duration of bleeding
Age of the patient
Type of bleeding
Anatomical location
What is the most common treatment for posterior epistaxis?
Observation only
Management under general anaesthesia
Cautery under local anaesthesia
Topical medications
What is the relationship between the External Carotid artery and epistaxis?
It supplies both plexuses involved in epistaxis
It is a cause of epistaxis
It only supplies posterior epistaxis
It is irrelevant to epistaxis
What is a key contributing factor to epistaxis in children?
Digital trauma
Vitamin K deficiencies
Hemophilia
Leukemia
What is a common symptom of epistaxis?
Nasal congestion
Facial swelling
Nosebleed
Ear pain
What is the purpose of cautery in treating epistaxis?
To stop the bleeding
To promote healing
To diagnose the cause
To prevent infection
What is depicted in the image related to epistaxis?
Statistics on epistaxis incidence
A list of causes of epistaxis, including trauma, tumors, infections, and disorders of hemostasis.
Anatomical diagrams of the nasal cavity
A treatment guide for epistaxis
What is a common aetiology for epistaxis related to medications?
Anticoagulants medications
Antihistamines
Antidepressants
Antibiotics
Which congenital condition is an uncommon aetiology for epistaxis?
Diabetes
Hypertension
Asthma
Haemophilia
What initial assessment is imperative in managing epistaxis?
ABC Assessment
Blood pressure measurement
CT scan
MRI
Which of the following is a sign to check for during assessment of epistaxis?
Signs of infection
Signs of haemorrhagic shock
Signs of allergy
Signs of dehydration
What should be done to control bleeding in epistaxis?
Use nasal spray
Apply ice pack on forehead
Tilt head back
Apply manual compression on nostrils
What is a method for treating anterior bleeding in epistaxis?
Oral antihistamines
Antibiotic treatment
Nasal packing with gauze
Nasal cautery with silver nitrate
What history taking aspect is vital to rule out contributing factors for epistaxis?
Travel history
Diet history
Medication history
Family history
What should be assessed if trauma is suspected in epistaxis?
Neck injury assessment
Head injury assessment
Chest injury assessment
Abdominal injury assessment
What is the purpose of a nasal tampon in epistaxis management?
To clean the nasal cavity
To prevent infection
To expand in the nasal cavity and apply pressure
To numb the nasal area
Which agent can be prescribed to prevent toxic shock syndrome when nasal packing is used for 24+ hours?
Acetaminophen
Ibuprofen
Amoxicillin
Ciprofloxacin
What is BIPP used for in nasal packing?
To clean the nasal cavity
To anesthetize the area
Advanced nasal packing
To promote healing
What is Floseal used for in epistaxis management?
Preventing infection
Cleaning the nasal cavity
Controlling epistaxis
Numbing the area
What procedure may be required if epistaxis is persistent?
Nasal tampon insertion
Antibiotic administration
Use of nasal spray
Examination Under General Anaesthesia
What is one of the options for controlling epistaxis in centers with Interventional Radiology?
Nasal packing
Use of nasal sprays
Embolization of artery
Electrocauterization
What is the function of the Rapid Rhino device in nasal packing?
To apply pressure to the nasal cavity
To provide anesthesia
To clean the nasal cavity
To administer medication
What is the recommended position for inserting a nasal tampon?
Along the septum
At an angle
Against the palate
Vertically
What is Reinke's oedema primarily caused by?
Viral infection
Emotional stress
Hypothyroidism
Cigarette smoking
What is a common treatment for early stages of Reinke's oedema?
Voice therapy
Surgical intervention
Stopping smoking and voice rest
Antibiotics
What condition can cause hoarseness due to vocal cord oedema?
Reinke's oedema
Muscle tension dysphonia
Hypothyroidism
Vocal cord paralysis
Which nerve is more often affected in unilateral vocal cord paralysis?
Right recurrent laryngeal nerve
Vagus nerve
Phrenic nerve
Left recurrent laryngeal nerve
What is a potential complication of bilateral vocal cord palsy?
Vocal fatigue
Airway compromise
Hoarseness
Dysphagia
What examination can confirm unilateral vocal cord palsy?
MRI brain
CT scan
Cranial nerve examination
Nasendoscopy
Which systemic disease can lead to vocal cord paralysis?
Asthma
Hypertension
Diabetes
COPD
What is a common idiopathic cause of vocal cord paralysis?
Idiopathic
Nuclear palsy
Thyroid malignancy
Vascular injury
What is the most commonly used material for Injection Medialisation Techniques in vocal cord palsy treatment?
Collagen
Glycerin
Hydroxyapatite
Silicone
What is the normal salivary production per day?
0.2 - 0.5 litres
1.5 - 2.5 litres
0.5 - 1.5 litres
1 - 2 litres
What is Sialadenitis?
Tumor in the salivary glands
Inflammation of salivary glands
Infection of the throat
Obstruction of the airway
Which condition can cause bilateral vocal cord palsy?
Chronic bronchitis
Iatrogenic trauma
Asthma
Pneumonia
What are common symptoms of Sialadenitis?
Erythema over the area
Hoarseness
Dry mouth
Difficulty swallowing
What can be a treatment option for airway obstruction in bilateral cord palsy?
Antibiotics
Inhalers
Surgery
Tracheostomy
What is a common cause of Sialadenitis?
Autoimmune disease
Bacterial infection
Allergic reaction
Viral infection
What is the function of salivary glands?
Lubrication of food
Absorption of nutrients
Secretion of hormones
Production of urine
What can be a cause of bilateral vocal cord palsy related to congenital conditions?
Asthma
Hydrocephalus
Tonsillitis
Chronic cough
What is a symptom that worsens during eating in Sialadenitis?
Fatigue
Pain
Dizziness
Nausea
What is the medical management for acute sialadenitis?
Hydration, antibiotics, warm compresses, massage, sialagogues
Surgery, gland excision, radiation therapy
Only hydration and antibiotics
Only warm compresses and massage
Which gland is preferentially affected in Sjögren syndrome?
Sublingual gland
Submandibular gland
Parotid gland
Minor salivary glands
What is a common ENT presentation of Sjögren syndrome?
Throat pain
Xerostomia
Nasal congestion
Hearing loss
What is sialadenosis?
Non-neoplastic noninflammatory swelling with gland hypertrophy
Cancer of the salivary glands
Infection of the salivary glands
Formation of salivary stones
Which laboratory test is used to confirm Sjögren syndrome?
Complete blood count
Liver function test
Thyroid function test
Autoantibodies SS-A and SS-B
What is a potential complication of Sjögren syndrome affecting the CNS?
Stroke
Vasculitis or demyelinating lesions
Alzheimer's disease
Parkinson's disease
What are the major categories of aetiologies for sialadenosis?
Nutritional, endocrine, metabolic, inflammatory/autoimmune, drug induced
Infectious, traumatic, genetic, environmental, metabolic
Viral, bacterial, fungal, autoimmune, drug induced
Only nutritional and endocrine
What is the primary staging system used for head and neck tumours?
UICC (Union for International Cancer Control)
FIGO (International Federation of Gynecology and Obstetrics)
TNM (Tumour, Nodes, Metastasis)
AJCC (American Joint Committee on Cancer)
Which professionals are part of the Head and Neck Oncology Multidisciplinary Team?
Surgeons, General Practitioners, Physiotherapists
ENT, Radiation Oncology, Medical Oncology, Radiology, Pathology, Specialist Nurses, Dieticians, Speech and Language therapists
Oncologists, Pharmacists, Social Workers
Dermatologists, Psychologists, Nutritionists
Which type of tumours is NOT included in head and neck cancers?
Salivary gland
Thyroid
Mucosal
Neurogenic
What is the purpose of the TNM staging system?
Guides management and gives prognostic information
Only for research purposes
To classify tumours by size
To determine treatment costs
What types of tumours are discussed in Head and Neck Oncology MDTs?
Skin, muscle, bone, nerve
Mucosal, thyroid, parathyroid, skin, salivary gland, vascular, neurogenic
Lung, breast, colon, prostate
Brain, liver, kidney, bladder
What does the diagram in Figure 35 illustrate?
Subtypes of head and neck cancers categorized by anatomical location
Statistics on cancer survival rates
Treatment methods for head and neck cancers
Symptoms of head and neck cancers
Which of the following is a common tumour type in the head and neck region?
Bone tumours
Salivary gland tumours
Liver tumours
Breast tumours
What symptom indicates difficulty swallowing in patients with mucosal tumours?
Odynophagia
Dysarthria
Dysphonia
Dysphagia
Which symptom is characterized by a hoarse voice?
Odynophagia
Dysarthria
Dysphonia
Dysphagia
What is referred otalgia related to?
Shared sensory innervation with the upper aerodigestive tract
Infection
Nerve damage
Inflammation
Which symptom describes pain when swallowing?
Dysphagia
Odynophagia
Dysarthria
Dysphonia
What sensation is referred to as globus?
Pain swallowing
Difficulty swallowing
Sensation of mass in throat
Hoarse voice
What should alert clinicians to potential head and neck malignancy?
Only smoking
Only weight loss
Symptoms in conjunction with risk factors
Only age
Which risk factors are mentioned for mucosal tumours?
Genetics
Diet and exercise
Smoking and systemic signs
Age
What is the main focus of the provided text?
Red flag presentations of mucosal tumours
Prevention strategies
Diagnosis methods
Treatment options
What does the diagram illustrate regarding referred otalgia?
Only the throat anatomy
Connections between various head and neck structures and the ear
Only the ear anatomy
Only the nasal anatomy
What is the most common tumor type in head and neck mucosa?
Adenocarcinoma
Squamous Cell Cancer (SCC)
Basal Cell Carcinoma
Melanoma
What are the premalignant lesions associated with SCC?
basal cell carcinoma
leukoplakia and erythroplakia
melanoma
actinic keratosis
What are the boundaries of the oral cavity?
Teeth to gums
Lips to uvula
Lips to junction of hard and soft palate
Tongue to pharynx
What are common causative agents for oral cavity tumors?
radiation and sunlight
tobacco and HPV
alcohol and diet
viral infections
What is a common presentation of oral cavity tumors?
Fever
Nausea and vomiting
Weight loss
Odynophagia and dysphagia
What is the mainstay of treatment for oral cavity tumors?
Chemotherapy only
Radiotherapy only
Immunotherapy
Surgery +/- radiotherapy
What procedure is typically required for the majority of oral cavity tumors?
Tracheostomy
Lymph node sampling
Neck dissection
Biopsy
What is the primary causative agent of oropharyngeal cancer?
Genetic mutations
Tobacco smoking
Human papilloma virus (HPV)
Alcohol consumption
What is a common presentation of oropharyngeal cancer?
Nasal congestion
Painless neck mass
Sore throat
Severe headache
How does HPV mediated oropharyngeal cancer compare to smoking induced cancers in terms of death risk?
Higher death risk
30% reduction in death risk
60% reduction in death risk
No difference in risk
What is a common treatment for oropharyngeal tumours?
Surgery +/- adjuvant radiotherapy
Only radiotherapy
Observation
Only chemotherapy
What is the significance of transoral robotic surgery in treating oropharyngeal tumours?
Eliminates the need for chemotherapy
Decreases recovery time
Increases the efficacy of surgery
Is less effective than traditional surgery
What anatomical boundaries define the oropharynx?
Pharyngeal walls only
Nasal cavity to the soft palate
Junction of soft palate and hard palate to the level of the hyoid bone
Base of skull to the hyoid bone
What are the two types of nasopharyngeal cancers?
Non-keratinising (NKSCC) and keratinising (KSCC) tumours
Benign and malignant tumours
Squamous cell carcinoma and adenocarcinoma
Melanoma and lymphoma
What is a common risk factor for Non-keratinising nasopharyngeal cancer?
Smoking
Epstein Barr Virus (EBV)
Alcohol exposure
Genetic (HLA I)
What is the main treatment for hypopharyngeal tumours?
Surgery
Chemotherapy
Radiotherapy
Immunotherapy
What is a common presentation of hypopharyngeal tumours?
Epistaxis
Nasal obstruction
Dysphagia
Painless neck mass
What is the primary risk factor for hypopharyngeal cancer?
Smoking
Epstein Barr Virus
Nitrosamines
Genetic factors
What is the shape of the nasopharynx?
Rectangular
Cylindrical
Spherical
Cuboid
What is a co-factor associated with hypopharyngeal cancer?
EBV
Alcohol
Genetic predisposition
Nitrosamines
What is the typical presentation of nasopharyngeal cancer?
Hoarseness
Cough
Painless neck mass
Sore throat
What surgical procedure may be required for very advanced hypopharyngeal tumours?
Tonsillectomy
Laryngectomy
Tracheostomy
Pharyngo-laryngo-oesophagectomy (PLO)
What are the primary roles of the larynx?
Movement, balance, coordination
Speech, swallowing, airway protection
Breathing, digestion, circulation
Hearing, taste, smell
What is the term for premalignant tumours in the larynx?
Papilloma
Dysplasia
Carcinoma in situ
Leukoplakia
What is the risk of carcinoma in situ transforming into a malignant tumour?
20%
5%
10%
50%
How are early stage tumours (T1) managed?
Observation
Total laryngectomy
Chemotherapy only
Surgery or radiotherapy
What is the recommended treatment for advanced tumours (T4)?
Surgery only
Total laryngectomy and radiotherapy
Radiotherapy only
Chemotherapy only
What are the subdivisions of the larynx based on the vocal cords?
Anterior, posterior, lateral
Supraglottic, glottic, subglottic
Superior, inferior, medial
Cervical, thoracic, abdominal
What symptoms may present in advanced laryngeal tumours?
Dysphonia, dysphagia, weight loss
Fever, cough, headache
Fatigue, muscle pain, joint pain
Nausea, vomiting, diarrhea
What is the structure that borders the larynx inferiorly?
Oropharynx
Trachea
Esophagus
Hypopharynx
What type of image shows laryngeal cancer?
X-ray of the chest
MRI of the brain
Photograph showing white growths on vocal cords
CT scan of the abdomen
What is a significant benefit of adding chemotherapeutic agents to radiotherapy?
Less need for surgery
Reduced treatment time
Increased pain
Improved local control and overall survival
What is the larynx primarily composed of?
Cartilaginous framework
Bone structure
Muscular tissue
Connective tissue
What is a laryngectomy?
Removal of the trachea
Surgery to repair vocal cords
Insertion of a tracheostomy tube
Removal of the larynx and separation of the airway from the mouth, nose, and esophagus
What is a major consequence of laryngectomy regarding breathing?
The patient requires a ventilator
The patient becomes an obligate neck breather
The patient can breathe normally through the mouth
The patient can still phonate normally
Which of the following is NOT a complication of laryngectomy?
Nerve injury
Chyle leak
Fistulae
Haematoma
What is a common indication for a laryngectomy?
Chronic cough
Allergies
Malignancy
Asthma
What is the purpose of a tracheo-oesophageal puncture?
To improve breathing
To prevent food aspiration
To enhance vocal cord function
To create a passage between the trachea and the esophagus
What device can be used for alaryngeal speech after laryngectomy?
Hearing aid
Respirator
Electrolarynx
Pacemaker
What happens to the vocal cords after a laryngectomy?
They function normally
They are enhanced
They are repaired
They are lost
What is a stoma in the context of laryngectomy?
A type of vocal cord
A surgical tool
An opening created for breathing
A breathing mask
What type of speech will patients have after a laryngectomy?
Alaryngeal speech
Normal speech
Enhanced speech
Whispered speech
What is shown in the diagram comparing normal anatomy with post-laryngectomy anatomy?
The stomach and intestines
The brain and spinal cord
The heart and lungs
The pharynx, larynx, trachea, and esophagus
What device is used to produce speech after a laryngectomy by allowing air from the lungs to pass through it?
Laryngeal mask
Tracheostomy tube
Voice prosthesis
Electrolarynx
What is the purpose of a tracheoesophageal puncture (TEP) in speech production?
To replace vocal cords
To allow airflow from the trachea to the esophagus
To block airflow to the lungs
To enhance sound production
Which part of the body is involved in airflow during the use of an electrolarynx?
Stomach
Kidneys
Lungs
Heart
In airflow with a tracheoesophageal puncture, what does air pass through before entering the esophagus?
The trachea
The vocal cords
The pharynx
A valve
What should all medical personnel be familiar with regarding laryngectomy patients?
Surgical procedures
Speech therapy
Long-term rehabilitation
Emergency management
How should laryngectomy patients be oxygenated or intubated?
They can be intubated via the mouth.
They cannot be intubated or oxygenated from the nose/mouth.
They can use a standard mask.
They can be oxygenated via the nose.
What type of signage should be found at the bedside of laryngectomy patients?
Overbed signs and algorithms
Medication charts
Dietary restrictions
Patient history forms
What information is included on the laryngectomy signage?
Date, tube size, hospital number, notes, emergency contact
Doctor's name, treatment plan, follow-up
Patient's name, age, allergies
Insurance information, family contacts
What is the primary focus of training for laryngectomy patients before discharge?
Physical therapy
Dietary changes
Management of their condition
Psychological counseling
What is the first step in managing a laryngectomy emergency?
Perform tracheal suction
Assess laryngectomy stoma patency
Call for airway expert help
Apply high flow oxygen to face
What should be used to assess the airway if available?
Manual resuscitation bag
Waveform capnography
Oxygen mask
Suction catheter
If the patient is not breathing, what should be done next?
Ventilate via stoma
Perform CPR immediately
Administer medication
Call for help
What should you do if the laryngectomy stoma is patent?
Deflate the cuff
Apply oxygen to the face
Perform tracheal suction
Remove the tube from the stoma
What is a primary emergency oxygenation method for a laryngectomy patient?
Bag-mask ventilation
Nasal cannula
Oxygen via mouth
Paediatric face mask applied to stoma
What should you consider using for intubation of a laryngectomy stoma?
Endotracheal tube without cuff
Laryngeal mask airway
Oral airway
Small tracheostomy tube / 6.0 cuffed ETT
What is a tracheostomy?
A type of lung surgery
A procedure to remove the larynx
The surgical formation of an opening into the trachea through the anterior neck
A method of intubation
What is one indication for performing a tracheostomy?
Chest tube insertion
Short term sedation
Laryngeal surgery
Long term ventilation
Which anesthesia can be used for a surgical tracheostomy?
Sedation only
Only local anesthesia
Local anesthesia (LA) or general anesthesia (GA)
Only general anesthesia
What type of incision can be made for a tracheostomy?
Lateral
Diagonal
Circular
Horizontal or vertical
What is the first step in performing a surgical tracheostomy?
Inserting the tracheostomy tube
Disconnecting the ventilator
Making a skin incision in the anterior neck
Placing a stay suture
What is included in the parts of a tracheostomy tube?
15 mm connector, cuff, flange, shaft, distal tip
Laryngeal mask, connector, shaft
Ventilator, tube, cuff
Endotracheal tube, cuff, balloon
What is a potential complication of a tracheostomy?
Infection at the incision site
Low oxygen levels
High bleeding risk
Pneumonia
What is a potential immediate complication of a tracheostomy?
Vocal cord paralysis
Paratracheal insertion (false passage)
Granulation tissue formation
Tracheomalacia
What are early complications of tracheostomy?
Infection
Tracheo-oesophageal fistula
Delayed stoma closure
Accidental decannulation
Bleeding
Tracheal stenosis
Loss of airway
What is a late complication of tracheostomy?
Accidental decannulation
Tracheomalacia
Subcutaneous emphysema
Aspiration
What is the purpose of the cuff in a tracheostomy tube?
To prevent infection
To enable speech
To prevent aspiration
To allow ventilation (closed circuit created)
What is a disadvantage of using a cuffed tracheostomy tube?
Prevents air reaching vocal cords, hence patients cannot speak
Facilitates swallowing
Allows for better ventilation
Reduces risk of infection
When should a cuffless tube be used after tracheostomy?
Immediately after surgery
Only if the patient requests it
When the patient is fully awake
As soon as ventilation is no longer required and there is no risk of aspiration
How is the cuff of a tracheostomy tube deflated?
By cutting the tube
Using a syringe
Automatically after a set time
By using a needle
What is a risk of failure of decannulation?
Complete recovery
Improved airway function
Reduced risk of infection
Permanent tracheostomy
What is the purpose of fenestrations in a tracheostomy tube?
Promotes airflow through upper airway allowing phonation
Facilitates mucus retention
Increases airway resistance
Prevents aspiration
What is a crucial function of the inner cannula in a tracheostomy tube?
Facilitates cleaning while maintaining the airway
Prevents phonation
Blocks mucus plugs
Increases airflow resistance
What can occur if fenestrations are not properly positioned in the airway?
Increased airflow
Decreased risk of blockage
Aspiration and granulation tissue
Easier phonation
What happens if the tracheostomy becomes blocked with a mucus plug?
The outer cannula must be replaced
The inner cannula can be removed
Airway resistance decreases
Phonation is enhanced
What should be placed above the bed of every patient with a tracheostomy?
A patient history report
A daily schedule
A list of medications
A sign with details of their procedure, indication, and tube
What is included in the 'Trachy Box' by the bedside?
Necessary supplies for accidental decannulation
Suctioning equipment only
Emergency contact numbers
Patient's medical records
What training do patients receive upon getting a tracheostomy?
Training on physical therapy
Training on suctioning and managing their own tubes
Training on dietary needs
Training on medication management
Why is it important for healthcare professionals to know about tracheostomy management?
To handle emergencies effectively
To prescribe medications
To conduct physical exams
To perform surgeries
What do algorithms developed for tracheostomy management help with?
Conducting routine check-ups
Guiding management in emergency situations
Scheduling patient appointments
Determining medication dosages
What should be done first if a patient with a tracheostomy is breathing?
Remove inner tube
Perform tracheal suction
Apply high flow oxygen
Call Resuscitation Team
What indicates a patent or partially patent airway during assessment?
Blood pressure monitoring
Chest X-ray
Waveform capnography
Pulse oximetry
What should be used to cover the stoma during emergency oxygenation?
Oral airway
Oxygen mask
Swabs or hand
Bag-valve-mask
What is the next step if you cannot pass a suction catheter through the tracheostomy?
Deflate the cuff
Remove inner tube
Call Resuscitation Team
Perform tracheal suction
If the tracheostomy tube is partially obstructed, what should be done?
Attempt oral intubation
Remove the tracheostomy tube
Apply high flow oxygen
Continue ABCDE assessment
What should be done if the patient is not breathing and the tracheostomy tube is patent?
Remove the tracheostomy tube
Ventilate via tracheostomy
Perform CPR
Deflate the cuff
When should the tracheostomy tube be removed?
If the patient is stable
If the patient is not stable or improving
If the tube is patent
If the patient is breathing
Which device can be used for secondary emergency oxygenation?
Oral airway adjuncts
Bag-valve-mask
Supraglottic airway device (e.g. LMA)
Paediatric face mask
What is a potential tool for intubation of the stoma?
Suction catheter
Endotracheal tube
Aintree catheter
Bag-valve-mask
What should be assessed at the mouth and tracheostomy?
Call for help
Apply high flow oxygen
Look, listen & feel
Perform CPR
What is the purpose of using waveform capnography in tracheostomy management?
To measure blood pressure
To assess oxygen saturation
To indicate airway patency
To monitor heart rate
What is the most common location for Acinic cell carcinoma?
Submandibular gland
Parotid
Sublingual gland
Buccal mucosa
What percentage of salivary gland malignancies does Acinic cell carcinoma represent?
15-20%
8-14%
1-5%
20-30%
Which imaging modality is 96% sensitive in diagnosing Adenoid Cystic carcinoma?
PET
CT
MRI
Ultrasound
What is a common presentation symptom of salivary gland malignancies?
Vision changes
Severe headache
Painless mass
Nausea
Which salivary gland malignancy is characterized by slow growth and excellent prognosis?
Lymphoma
Mucoepidermoid
Adenoid Cystic
Acinic cell carcinoma
What is the demographic trend for Adenoid Cystic carcinoma?
Men more than women in 30-40s
Women more than men in 40-60s
More common in children
Equal in both genders
Which imaging technique helps assess infiltration and lymph nodes in salivary gland malignancies?
CT
X-ray
PET
MRI
What is a common association with salivary gland malignancies?
Diabetes
Hypertension
Asthma
Metastatic nodes from Skin Ca
What percentage of salivary tumors does Adenoid Cystic carcinoma represent?
5-10%
10-22%
20-30%
15-25%
What are common symptoms associated with salivary gland malignancies?
CN VII palsy or paralysis
Chest pain
Persistent cough
Severe dizziness
What percentage of patients present with occult metastasis at diagnosis?
33%
50%
20%
24%
Which two locations are most commonly affected by metastasis?
Lung and Bone
Liver and Brain
Kidney and Pancreas
Skin and Muscle
What is the most common type of salivary gland malignancy?
Mucoepidermoid carcinoma
Pleomorphic adenoma
Adenoid cystic carcinoma
Acinic cell carcinoma
What is the survival rate for low/intermediate grade mucoepidermoid carcinoma after surgery?
60-70%
80-90%
40-50%
30-40%
What is the most common benign salivary gland tumor?
Adenoid cystic carcinoma
Pleomorphic adenoma
Mucoepidermoid carcinoma
Warthin's tumor
What percentage of parotid gland tumors are benign?
80%
90%
60%
50%
What is the typical presentation of pleomorphic adenomas?
Rapidly growing painful mass
Firm and fixed lump
Soft and mobile mass
Slow growing painless lump
What is the facial nerve's involvement in pleomorphic adenomas?
Frequently involved
Always affected
Affected in all cases
Very rarely affected
What are the three histological grades of mucoepidermoid carcinoma?
Benign, Malignant, Transitional
Simple, Complex, Mixed
Mild, Moderate, Severe
Low, Intermediate, High
What type of treatment is typically given for high-grade mucoepidermoid carcinoma?
Radiotherapy only
Chemotherapy only
Surgery +/- Selective Nodal Dissection +/- radiotherapy
Surgery alone
What is the risk of pleomorphic adenomas transforming into malignant tumors over 15 years?
5%
15%
20%
10%
What is the prognosis for carcinoma ex-pleomorphic after transformation?
40% 5-year survival
30% 5-year survival
50% 5-year survival
60% 5-year survival
What is the most common treatment for pleomorphic adenomas?
Observation
Radiation therapy
Chemotherapy
Parotidectomy
What is the incidence of thyroid cancer in women per 100,000?
10
5
2
20
What is the survival rate for differentiated thyroid cancer (DTC) over 10 years?
60-65%
92-98%
80-85%
70-75%
What is the modality of choice for investigating thyroid nodules?
Ultrasound (US)
MRI
CT scan
X-ray
What clinical feature indicates a higher risk of thyroid cancer?
Small size
Painless mass
Firm nodule
Soft nodule
What should be checked in haematology for medullary thyroid cancer?
Free T4
Calcitonin/CEA
Thyroglobulin
TSH
What classification is used for ultrasound assessment of thyroid nodules?
A Classification
B Classification
C Classification
U Classification
Which of the following is a characteristic of benign thyroid nodules?
Intra-nodular vascularity
Solid hypo-echoic
Lobulated outline
Peripheral vascularity
What is a feature of suspicious thyroid nodules?
Peripheral vascularity
Solid, hypo-echoic
Micro-cystic
Cystic change
Which thyroid cancer subtype is most common?
Anaplastic
Medullary
Follicular
Papillary
What is a feature of malignant thyroid nodules?
Cystic change
Solid, hypo-echoic, lobulated outline
Peripheral egg shell calcification
Iso-echoic
What does 'de-differentiation' refer to in thyroid tumors?
The location of metastasis
The degree of carcinoma deviation from normal cells
The size of the tumor
The type of cancer
What is a characteristic associated with papillary thyroid cancer?
High aggressiveness
No metastasis
Poor prognosis
Good prognosis
What is the first step in the investigation of thyroid nodules if suspicious?
US guided FNA if nodule >10mm
TFTS
Clinical exam
Document cytology score
What does a Thy 1 cytology score indicate?
Benign
Indeterminate/equivocal
Non-diagnostic
Suspicious
What is the most common treatment for thyroid cancer?
US guided FNA
Total thyroidectomy
Radioactive iodine
Diagnostic hemi-thyroidectomy
Which of the following is NOT a criterion for a completion thyroidectomy?
Clinically negative lymphadenopathy in neck
Tumours > 4cm
Low risk
Multifocal
What is the purpose of radioactive iodine in adjuvant treatment?
Increase hormone levels
Reduce tumor size
Prevent recurrence
Destroy metastasis and residual tissue
What is the effective method for monitoring local recurrence in thyroid cancers?
MRI
US neck
X-ray
CT scan
What biological marker is used for monitoring papillary and follicular thyroid cancers?
Calcitonin
T3
TSH
Thyroglobulin
What percentage of thyroid malignancies does follicular thyroid cancer account for?
15%
10%
20%
5%
Follicular thyroid cancer arises from which type of cells?
Thyroid follicular cells
Thyroid C cells
Thyroid parafollicular cells
Thyroid medullary cells
What is the initial surgery for patients with follicular neoplasms?
Thyroid lobectomy
Hurtle cell removal
External beam radiotherapy
Total thyroidectomy
Which type of thyroid cancer is more likely to develop lung and bone metastases?
Medullary thyroid cancer
Papillary thyroid cancer
Hurtle cell cancer
Follicular thyroid cancer
What percentage of patients with FTC have metastases beyond cervical or mediastinal areas on initial presentation?
25%
20%
5%
11%
What treatment is indicated for aggressive or advanced follicular thyroid cancer?
Adjuvant Radioactive iodine
Observation
Chemotherapy
Hormone therapy
What is the significance of a RET mutation in medullary thyroid cancer?
RET mutation has no significance
Less RET mutation = more aggressive tumor
RET mutation indicates benign tumor
More RET mutation = more aggressive tumor
Which symptoms are associated with medullary thyroid cancer?
Flushing and diarrhea
Hair loss and skin rash
Nausea and vomiting
Weight gain and fatigue
What is the recommended treatment if invasive FTC is found on the final histologic section?
Adjuvant chemotherapy
Only observation
No further treatment
Completion of thyroidectomy
What is the monitoring approach for follicular thyroid cancer?
Same as papillary thyroid cancer
More frequent imaging
Only blood tests
No monitoring needed
What is the classification of medullary thyroid cancer in terms of prevalence?
0.5-1% of thyroid malignancies
1-3% of thyroid malignancies
5-10% of thyroid malignancies
10-15% of thyroid malignancies
When is external beam radiotherapy (EBRT) indicated?
For all thyroid cancers
Only for benign conditions
If all gross disease cannot be resected
When the patient refuses surgery
What is measured to investigate Medullary thyroid cancer?
Serum Calcium & PTH
Calcitonin & CEA
24 urinary Catecholamines
RET proto-oncogene
What is the primary management for Medullary thyroid cancer?
Palliative care
Chemotherapy only
Total Thyroidectomy & level VI neck dissection
Observation
What is the prognosis for Anaplastic thyroid cancer?
Average prognosis is six months
Average prognosis is nine months
Average prognosis is one year
Average prognosis is two years
Which imaging techniques are used for monitoring Medullary thyroid cancer?
Endoscopy
US, MRI, CT scanning
X-ray
PET scan
What is required if local metastatic lymph nodes are present in Medullary thyroid cancer?
Neck dissections of these and adjacent lymphatic nodal beds
Radiation therapy
Observation only
Chemotherapy
What should be monitored hematologically in Medullary thyroid cancer?
Thyroid hormones
Calcitonin levels
Blood glucose
Calcium levels
What is the primary function of parathyroid hormone (PTH)?
Insulin secretion
Protein synthesis
Blood pressure regulation
Calcium homeostasis
Which of the following is NOT a physiological function of calcium?
Neuromuscular transmission
Protein synthesis
Cardiac automaticity
Coagulation
What does parathyroid hormone do to renal calcium reabsorption?
Decreases renal calcium reabsorption
Increases renal phosphate excretion
Increases renal calcium reabsorption
Has no effect on renal calcium reabsorption
How does parathyroid hormone affect vitamin D3 production?
Increases renal production of Vitamin D3
Has no effect on Vitamin D3
Increases intestinal absorption of Vitamin D3
Decreases renal production of Vitamin D3
Which of the following processes is regulated by calcium?
Blood filtration
Digestion
Smooth muscle contraction
Hormone secretion
What is the effect of parathyroid hormone on phosphate levels?
Increases phosphaturia
Increases phosphate absorption
Decreases phosphaturia
Has no effect on phosphate levels
What role does calcium play in nerve function?
Regulates blood pressure
Facilitates nerve transmission
Has no role in nerve function
Inhibits nerve transmission
What is the source of calcium released into the bloodstream by parathyroid hormone?
Bone
Kidneys
Liver
Muscles
What is one of the roles of calcium in cell division?
Inhibits cell division
Promotes protein synthesis
Has no effect on cell division
Regulates cell movement
What does the diagram illustrate regarding calcium homeostasis?
Calcium absorption only
Kidney filtration
Bone structure
Regulation by parathyroid hormone and organs
What are common neuro-psychiatric symptoms of hypercalcaemia?
Depression
Constipation
Hypertension
Bone pain
What is the most common cause of secondary hyperparathyroidism?
Chronic hypocalcaemia
Vitamin D deficiency
Parathyroid carcinoma
Parathyroid adenoma
What percentage of hyperparathyroidism cases are due to parathyroid adenoma?
~80%
10-15%
50%
1-5%
What is a common gastrointestinal symptom of hypercalcaemia?
Arrhythmias
Fatigue
Muscle weakness
Abdominal pain
What is the male to female ratio in primary hyperparathyroidism?
3:1
1:1
2:1
1:3
What is the incidence rate of primary hyperparathyroidism?
100/100,000
21/100,000
10/100,000
50/100,000
What musculo-skeletal symptom is associated with hypercalcaemia?
Kidney stones
Hypertension
Osteoporosis
Anorexia
What is a renal symptom of hypercalcaemia?
Anorexia
Fracture
Frequent urination
Abdominal pain
What is tertiary hyperparathyroidism caused by?
Parathyroid adenoma
Chronic overstimulation of hyperplastic glands
Renal stones
Vitamin D deficiency
What percentage of hyperparathyroidism cases are due to parathyroid carcinoma?
50%
1-5%
80%
10-15%
What conditions should be ruled out in diagnostic considerations for hyperparathyroidism?
MEN1, MEN2a
Cushing's Syndrome
Diabetes Mellitus
Hyperthyroidism
What does elevated calcium in the absence of normal PTH suggest?
Vitamin D deficiency
Malignancy
Kidney stones
Hyperparathyroidism
What is one cause of lithium-induced hypercalcemia?
Thyroid medication
Lithium medication
Corticosteroids
High calcium diet
Which blood tests are essential for diagnosing hyperparathyroidism?
Creatinine, Uric Acid, Electrolytes
Lipid profile, Liver enzymes, Thyroid hormones
PTH, Calcium, Vitamin D levels
Glucose, Insulin, Hemoglobin
What imaging techniques are used in the investigation of hyperparathyroidism?
U/S, Sestamibi, 4D-CT
CT scan, Ultrasound, Bone scan
X-ray, MRI, PET scan
Echocardiogram, Angiogram, Fluoroscopy
What is the treatment of choice for primary hyperparathyroidism?
Dietary phosphate restriction
Surgical resection of the adenoma
Phosphate binders
Vitamin D analogues
What causes secondary hyperparathyroidism?
Vitamin D overdose
Surgical resection
Chronic abnormal stimulus
Genetic mutation
Which laboratory finding is expected in secondary hyperparathyroidism due to renal insufficiency?
High serum calcium
Low serum calcium
Normal serum phosphate
High serum phosphate
What is a common treatment for secondary hyperparathyroidism?
High-dose Vitamin D
Dietary phosphate restriction
Calcium restriction
Surgical resection
What characterizes tertiary hyperparathyroidism?
Low serum calcium
Normal secretion of PTH
Continued excessive secretion of PTH despite normal or high serum calcium
Absence of parathyroid hypertrophy
What is the effect of bisphosphonates in tertiary hyperparathyroidism?
Increased serum calcium
Increased urinary calcium
Decreased PTH levels
Increased BMD in spine and hip
What is the most common cause of hypercalcaemia in hospitalised patients?
Parathyroid hormone-related peptide
Local osteolytic metastatic lesions
Overproduction of Vitamin D
Granulomatous disease
What is the primary diagnosis indicator for hypercalcaemia of malignancy?
Elevated Vitamin D
HIGH PTH
Normal PTH
LOW PTH
Which type of cancer is most commonly associated with hypercalcaemia of malignancy?
Breast cancer
Ovarian cancer
Squamous cell lung cancer
Multiple myeloma
What percentage of hypercalcaemia cases in malignancy are due to solid tumors without metastasis?
80%
20%
100%
50%
Which skin cancer is described as slow-growing and locally invasive?
Melanoma
Merkel Cell Carcinoma
Basal Cell Carcinoma
Squamous Cell Carcinoma
What disciplines are involved in the management of sun-induced skin cancers?
Internal Medicine, Cardiology, Dermatology
Oncology, Radiology, Pathology
Dermatology, Plastic surgery, ENT
Pediatrics, Neurology, Psychiatry
What age group is most affected by Basal Cell Carcinoma?
9th Decade
4th Decade
7th Decade
2nd Decade
What is a common cause of increased serum calcium levels besides malignancy?
Obesity
Hypertension
Diabetes
Granulomatous disease
What is one of the humoral factors produced by tumors that can lead to hypercalcaemia?
Insulin
Cortisol
PTH-rP
Adrenaline
Where do sun-induced skin cancers commonly occur?
Head and neck
Arms
Back
Legs
What is a predisposing factor for basal cell carcinoma (BCC)?
High blood pressure
Obesity
Diabetes
Exposure to UV radiation
Which subtype of basal cell carcinoma is considered aggressive?
Morphoeic
Nodular
Cystic
Superficial
What is the gold standard treatment for basal cell carcinoma?
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
What is the recommended surgical margin for a 0-2 cm basal cell carcinoma?
1-2mm
10-12mm
4-5mm
8-10mm
What is the 5-year cure rate for primary lesions treated with radiotherapy?
70%
95%
80%
90%
Which feature is NOT a high-risk feature for basal cell carcinoma?
Poorly defined margins
Immunosuppression
Tumour size
Tumour site
Which subtype of basal cell carcinoma is characterized by infiltrative growth?
Keratotic
Infiltrative
Pigmented
Nodular
Which condition is contraindicated for radiotherapy?
Gorlin's Syndrome
Squamous cell carcinoma
Basal cell carcinoma
Melanoma
What is the definition of squamous cell carcinoma (SCC)?
A benign tumor of the skin
Locally invasive malignant tumor from keratinizing cells of the epidermis
A type of melanoma
A tumor that only occurs in the lungs
What is the second most common skin cancer?
Melanoma
Basal cell carcinoma
Dermatofibroma
Squamous cell carcinoma (SCC)
Which of the following is a predisposing factor for SCC?
Hypertension
Chronic UV light exposure
High cholesterol
Diabetes
What size of SCC tumors is three times more likely to metastasize?
Tumors > 5cm
Tumors > 2cm
Tumors = 1cm
Tumors < 1cm
Which histological differentiation subtype of SCC has a worse prognosis?
Poorly differentiated
Atypical
Well differentiated
Mildly differentiated
Which area has the greatest risk for SCC metastasis?
Back
Inner thigh
Non-sun exposed sites
Sun exposed area
What is a common environmental factor that can predispose someone to SCC?
Vitamin D deficiency
High sugar diet
Arsenic exposure
Low protein diet
Which condition is associated with a higher risk of SCC due to immunosuppression?
Diabetes
Recurrent disease
High blood pressure
Asthma
What is the histological subtype of SCC that is characterized by spindle cells?
Well differentiated subtype
Desmoplastic subtype
Acantholytic subtype
Spindle subtype
What type of skin is more likely to develop SCC?
Dark skin
Fair skin
Oily skin
Combination skin
What is the recommended surgical margin for well-defined, low-risk tumors less than 2 cm in size?
8 mm
2 mm
6 mm
4 mm
For tumors larger than 2 cm, what is the required surgical margin?
4 mm
8 mm
2 mm
<blockquote>
6 mm
</blockquote>
What is a reason to use radiotherapy instead of surgery?
Patient unfit for surgery
Patient prefers surgery
Low risk of metastasis
Small tumor size
What percentage of melanomas are superficial spreading?
70%
10%
25%
5%
What is the incidence of melanoma in the USA?
21 per 100,000
7.9 per 100,000
30 per 100,000
15 per 100,000
Which melanoma subtype is associated with higher rates of local recurrence?
Desmoplastic melanoma
Melanomas of the face and scalp
Acral lentiginous
Nodular melanomas
Desmoplastic melanoma is more common in which region?
Lower lid
Trunk
Extremities
Head and neck
What is the primary cell type involved in melanoma?
Cutaneous melanocyte
Keratinocyte
Fibroblast
Lymphocyte
What is an indication for radiotherapy in melanoma treatment?
Only for patients over 60
Adjuvant treatment of nodal metastasis
Only for small tumors
All melanoma cases
What subtype of melanoma accounts for less than 1%?
Acral lentiginous
Lentigo maligna
Superficial spreading
Nodular melanomas
What is a risk factor for melanoma related to the number of moles?
More than 100 normal moles
Exactly 100 normal moles
Less than 50 normal moles
Only 1 normal mole
Which type of melanoma is characterized by dark skin lesions on the sole of the foot?
Nodular melanoma
Lentigo maligna
Acral lentiginous melanoma
Superficial spreading melanoma
What hair or skin type is considered a risk factor for melanoma?
Brown hair and olive skin
Blonde hair and tanned skin
Black hair and dark skin
Red hair or skin that burns in the sun
What family history is a risk factor for melanoma?
No cases of melanoma in the family
One case of melanoma in second-degree relatives
Three or more cases of melanoma in distant relatives
Two or more cases of melanoma in first-degree relatives
What type of melanoma is depicted in the image with a close-up of a dark skin lesion?
Nodular melanoma
Lentigo maligna
Superficial spreading melanoma
Acral lentiginous melanoma
What is the recommended surgical margin for melanoma in situ?
2cm margin
1cm margin
No margin required
5mm margin
What thickness of melanoma requires a 1cm surgical margin?
Thickness ≤ 1mm
Thickness < 1mm
Thickness ≥ 2mm
Thickness ≥ 1mm
What thickness of melanoma requires a 2cm surgical margin?
Thickness < 1mm
Thickness ≥ 1mm
Thickness = 1mm
Thickness ≤ 1mm
What is the purpose of a Sentinel Lymph Node Biopsy (SLN Bx)?
Prevention of melanoma
Diagnosis of melanoma
Treatment of melanoma
Accurate staging of melanoma
Which patients are indicated for imaging?
Stage IB patients
Stage I patients
Stage IA patients
Stage IIC patients without SLN bx
What is Vemurafenib used for?
Chemotherapy for all cancers
Targeted treatment for BRAF v600 positive cancers
Immunotherapy for all cancers
Radiation therapy for melanoma
Flashcards in this deck (759)
-
What does ENT stand for in the context of Otolaryngology?
Ear, Nose, and Transplant
Ear, Nose, and Treatment
Ear, Nose, and Therapy
Ear, Nose, and Throat
-
Which of the following is NOT a sub-specialty of Otolaryngology?
Paediatric Otolaryngology
Otology/Neurotology and Skull Base Surgery
Facial Plastics
Rhinology and Endoscopic Sinus Surgery
-
What percentage of general practice is estimated to deal with ENT pathology?
20-30%
30-40%
10-15%
50-60%
-
What is one of the key skills expected to be performed during the rotation in Otolaryngology?
Dermatological Exam
Neurological Exam
Cardiac Exam
Otoscopy
-
Which of the following is a necessary clinical skill to learn during the Otolaryngology rotation?
Taking a full ENT history
Performing a lumbar puncture
Conducting a physical therapy session
Administering anesthesia
-
What is a primary focus of Otolaryngology as a specialty?
Pharmacology
Anatomical region
Genetics
Specific organ system
-
Which examination is part of the course objectives in Otolaryngology?
Cardiac examination
Abdominal examination
Thyroid examination
Lung examination
-
What should a student differentiate regarding ENT diseases?
When a patient requires primary treatment
When to perform surgery
When to prescribe antibiotics
When to refer to a psychologist
-
Which conditions require a specialist ENT opinion?
Minor ear infections
Common cold
Seasonal allergies
Conditions that cannot be managed by a GP
-
What is necessary for understanding common ENT diseases?
Knowledge of pharmacology and toxicology
Knowledge of surgery techniques
Knowledge of dermatology
Knowledge of pediatrics
-
What types of referrals are mentioned for ENT conditions?
Over-the-counter treatment
Home remedies
Immediate hospitalization
Routine or urgent referral
-
-
-
What part of the ear transmits vibrations to the cochlea?
Outer ear
Middle ear
Eustachian tube
Inner ear
-
-
-
-
-
What does the diagram of the ear illustrate?
Function of the ear
Anatomy of the ear
Balance mechanism
Hearing process
-
-
Which part of the ear is involved in transmitting sound vibrations?
Auricle
Cochlea
Tympanic membrane
Semicircular canals
-
-
What is the function of the tympanic membrane in the ear?
It transmits nerve impulses
It stabilizes balance
It contains the cochlea
It vibrates in response to sound waves
-
-
What are the three tiny bones in the middle ear called?
Malleus, Incus, Stapes
Cochlea, Utricle, Saccule
Tympanic, Auditory, Semicircular
Vestibule, Cristae, Macula
-
How do low frequency sound waves affect the cochlea?
They affect the semicircular canals
They cause the tympanic membrane to vibrate
They stimulate the base of the cochlea
They stimulate the apex of the cochlea
-
What is the role of the vestibular apparatus?
To help maintain balance and orientation
To detect sound frequencies
To transmit nerve impulses
To vibrate in response to sound
-
What do the semicircular canals provide information about?
Posture
Linear movement
Sound frequency
Rotational movement
-
Which two chambers are part of the vestibular apparatus?
Utricle and Saccule
Tympanic and Auditory
Cochlea and Cristae
Base and Apex
-
What type of information does the vestibular system send to the brain?
Information about light
Information about sound waves
Information about acceleratory movement
Information about temperature
-
What is the function of the organ of Corti?
It transmits sound waves
It vibrates in response to pressure
It stabilizes balance
It is the receptor for hearing
-
What do sensory hair cells in the cochlea do?
They vibrate in response to sound waves
They transmit electrical impulses directly
They stabilize balance
They stimulate nerves that carry sound messages to the brain
-
What is the primary function of the utricle and saccule?
To stabilize vision
To detect linear acceleration
To transmit sound waves
To detect sound frequencies
-
What does the diagram of the cochlea illustrate?
The function of the semicircular canals
How different frequencies of sound waves stimulate different parts of the cochlea
The process of hearing in the brain
The structure of the tympanic membrane
-
What transmits information about the speed and direction of head movement to the brain?
Semicircular canals
Hair cells
Maculae
Vestibule
-
What are common manifestations of vestibular disorders?
Nausea
Tinnitus
Hearing loss
Vertigo or ataxia
-
Which sensory areas in the inner ear contribute to our sense of balance?
Cochlea and utricle
Semicircular canals and vestibule
Auditory and visual systems
Maculae and cristae
-
What is the role of the vestibular system in maintaining balance?
Integrates sensory information for balance
Regulates heart rate
Processes auditory signals
Controls vision
-
Which systems contribute to maintaining balance?
Endocrine, muscular, skeletal
Vestibular, visual, auditory, proprioceptive
Nervous, immune, reproductive
Respiratory, circulatory, digestive
-
What are the tiny hairs that project into the mucous layer of the nose called?
Odour molecules
Nerve cells
Cilia
Olfactory bulbs
-
Where do the olfactory nerve signals transmit after the olfactory bulb?
Frontal cortex
Spinal cord
Thalamus
Limbic system
-
What is the role of the limbic system in relation to smell?
Conscious perception of smell
Stimulating odour molecules
Responsible for emotion
Transmitting signals to the olfactory bulb
-
How many nerve cells are approximately in the olfactory regions?
About 5 million
About 10 million
About 1 million
About 2 million
-
What does the olfactory bulb transmit signals to?
The nasal cavity
Other areas deeper in the brain
The throat
The spinal cord
-
-
Where are taste buds primarily located?
In the throat
On the surface of the tongue
On the palate
In the tonsils
-
How many taste buds are approximately found in the mouth?
Around 15,000
Around 20,000
Around 10,000
Around 5,000
-
-
What is stimulated when food or drink is consumed?
Taste cells
Visual receptors
Touch receptors
Smell cells
-
What is the role of saliva in taste perception?
It enhances smell
It absorbs flavors
It cools the mouth
It dissolves food and drink
-
What type of nerve cells are found in taste buds?
Pain receptors
Temperature receptors
Taste-detecting nerve cells
Pressure receptors
-
-
What is depicted in the diagram of the tongue?
Saliva glands
Taste receptors only
Taste regions
Taste buds and their anatomy
-
What is Otitis Media with Effusion (OME) commonly known as?
Ear Infection
Middle Ear Syndrome
Swimmer's Ear
Glue Ear
-
What is a significant risk factor for developing OME in children?
Lack of exercise
High sugar diet
Parents who smoke
Excessive screen time
-
What anatomical feature makes children more susceptible to middle ear disease?
Thicker ear drum
Longer Eustachian tubes
Shorter Eustachian tubes
More vertical Eustachian tubes
-
What is a potential consequence of untreated OME in children?
Permanent middle ear damage
Improved hearing
Enhanced speech
Increased balance
-
What characterizes the pathology of OME?
Fluid accumulation in the outer ear
Acute infection
Chronic mucosal inflammation
Thickening of the ear drum
-
-
Why is early recognition and treatment of OME important?
To avoid ear surgery
To prevent impairment of development
To reduce allergies
To enhance hearing ability
-
What does the diagram in Figure 8 illustrate?
Earwax buildup
Differences in Eustachian tubes with age
Eardrum rupture
Middle ear infection
-
What is a symptom of poor auditory function in children?
Delayed language development
Improved listening skills
Enhanced educational progress
Increased speech clarity
-
Which sign indicates fluid in the middle ear?
Normal hearing test
Clear tympanic membrane
Visible earwax
Dull appearance with radial vessels visible on the tympanic membrane
-
-
What is a treatment option for children with persistent bilateral OME?
Antibiotics
Hearing aids
Physical therapy
Insertion of ventilation tubes (Grommets)
-
What is a common symptom associated with recurrent ear infections?
Strong balance
Excellent listening skills
High academic achievement
Poor educational progress
-
What does a flat impedance curve on tympanograms indicate?
Inner ear damage
Excessive earwax
Normal ear function
Possible middle ear dysfunction
-
What can cause balance problems and clumsiness in children?
Strong muscles
Fluid in the middle ear
High intelligence
Good vision
-
What is a sign of conductive deafness during testing?
Visible fluid in the outer ear
Immobile drum on testing with pneumatic speculum
Normal drum movement
Clear hearing on audiometry
-
What is the definition of Acute Otitis Media (AOM)?
Inflammation of the throat.
Acute inflammation of the middle-ear cavity with infection.
Chronic inflammation of the outer ear.
Infection of the inner ear.
-
-
Which virus is commonly associated with Acute Otitis Media?
Zika virus
HIV
Ebola virus
Respiratory syncytial virus
-
What is the most common bacterial cause of Acute Otitis Media?
Streptococcus pneumoniae
Escherichia coli
Haemophilus influenzae B
Moraxella catarrhalis
-
Which bacteria accounts for 25% of Acute Otitis Media cases?
Streptococcus pneumoniae
Staphylococcus aureus
Moraxella catarrhalis
Haemophilus influenzae B
-
What is a common precursor to Acute Otitis Media?
Earwax buildup
Chronic sinusitis
Upper respiratory tract infection (U.R.T.I.)
Allergic rhinitis
-
What is indicated by a bulging tympanic membrane?
Chronic otitis externa
Otitis media with effusion
Earwax blockage
Normal tympanic membrane
-
What part of the ear is affected by Acute Otitis Media?
Inner ear
Eustachian tube
Middle ear cavity
Outer ear canal
-
What is the first step in the inflammatory process leading to tympanic membrane perforation in ASOM?
Oedema closes the Eustachian Tube
Organisms invade mucous membrane
Desquamation perforation
Bulging of drum, loss of landmarks
-
Which antibiotic is the drug of choice for treating acute otitis media?
Amoxicillin
Co-amoxiclav
Ibuprofen
Penicillin
-
What should be done if otorrhoea persists after the acute phase of ASOM?
Administer analgesia
Send a specimen for C & S
Perform myringotomy
Continue antibiotics
-
What is a common underlying condition associated with recurrent episodic Acute Otitis Media?
Trisomy 21
Cleft lip
Diabetes
Asthma
-
What is the purpose of grommet insertion in children with recurrent attacks of otitis media?
To treat existing infections
To improve hearing
To prevent tympanic membrane perforation
To break the sequence of recurrent attacks
-
What is the recommended treatment for a child under 2 years old with acute otitis media?
Observation for 72 hours
Steroid treatment
Direct to antibiotics
Analgesia only
-
What symptom indicates persistent acute otitis media requiring hospital admission?
Fever without ear discharge
Bulging drum with severe symptoms
Mild ear pain
Clear ear discharge
-
What is a common cause of recurrent acute otitis media?
Exposure to cold weather
Poor diet
Lack of exercise
Underlying immunological defect
-
What is the recommended duration of antibiotic treatment for acute otitis media?
Five days
Two weeks
One week
Three days
-
What is chronic suppurative otitis media (C.S.O.M.) characterized by?
Fluid accumulation without perforation
Sudden hearing loss
Normal tympanic membrane appearance
A perforated tympanic membrane with persistent drainage for more than 2-6 weeks
-
What are common risk factors for chronic suppurative otitis media?
Living in isolated conditions
No previous ear infections
History of multiple episodes of acute otitis media
Single child family
-
What is a key feature of chronic suppurative otitis media?
Complete blockage of the Eustachian tube
Tympanic membrane perforation, usually centrally located
Thickening of the tympanic membrane
Absence of any drainage
-
What can trigger recurrent infections in C.S.O.M.?
Upper respiratory tract sepsis via the Eustachian Tube
Exposure to loud noises
High altitude changes
Swimming in pools
-
What can occur during a period of quiescence in C.S.O.M.?
Fever
Complete recovery
Severe pain
Hearing loss
-
-
What can cause tympanic membrane perforation besides C.S.O.M.?
Trauma and previous grommet insertion
High altitude flying
Cold weather exposure
Earwax buildup
-
What imaging studies are recommended to assess the extent of CSOM disease?
PET scan
Ultrasound
CT or MRI
X-ray
-
What is a key component of CSOM treatment?
Oral antibiotics
Intravenous fluids
Corticosteroid injections
Frequent aural toilet (microsuction)
-
What procedure is performed if CSOM treatment fails?
Cochlear implant
Tympanoplasty
Myringotomy
Tympanomastoidectomy
-
Who is most commonly affected by nasopharyngeal angiofibroma?
Elderly males
Children
Adult females
Teenage males
-
What symptom is commonly associated with nasopharyngeal angiofibroma?
Prolonged recurrent epistaxis
Hoarseness
Chronic cough
Sore throat
-
What is the main treatment for enlarging nasopharyngeal angiofibroma?
Chemotherapy
Antibiotics
Observation
Surgery
-
What imaging technique is used to confirm the presence of angiofibroma?
Endoscopy
CT or MRI scan
Ultrasound
X-ray
-
What can occur due to the aggressive nature of angiofibroma?
Development of ulcers
Formation of cysts
Calcification of tissues
Erosion of bone
-
What are adenoids a component of?
Palatine tonsils
Waldeyer's ring of lymphoid tissue
Eustachian tube
Lingual tonsils
-
What can enlarged adenoids cause?
Ear infections
Nasal airway obstruction
Throat swelling
Chronic cough
-
-
Which symptom is NOT associated with enlarged adenoids?
Nasal congestion
Mouth breathing
Snoring
Sore throat
-
What is a common indication for adenoidectomy?
Chronic mouth breathing
Chronic cough
Nasal polyps
Earwax buildup
-
What can chronic mouth breathing lead to?
Weight gain
Increased appetite
Improved speech
Palatal and dental abnormalities
-
-
What symptom might small children exhibit instead of sore throat?
Nasal congestion
Refusal to eat
Excessive sleeping
Loud crying
-
-
What is the first choice analgesia for adults with tonsillitis?
Ibuprofen
Naproxen
Paracetamol
Aspirin
-
What is the antibiotic of choice for severe tonsillitis?
Penicillin V
Amoxicillin
Ciprofloxacin
Erythromycin
-
How many episodes of tonsillitis in one year indicate tonsillectomy?
10 episodes
5 episodes
7 episodes
3 episodes
-
What is a complication of recurrent tonsillitis?
Dehydration
Ear infection
Tonsillectomy
Chronic cough
-
What is a sign of follicular tonsillitis?
Sore throat
Enlarged and hyperaemic tonsils
Fever
Swollen lymph nodes
-
What should patients with tonsillitis do to prevent dehydration?
Avoid fluids
Drink as much as possible
Drink large amounts of juice
Only drink soda
-
-
What is a characteristic feature of the pharyngeal mucosa in tonsillitis?
Dryness
Inflammation
Bleeding
Swelling
-
What is a visual sign of acute follicular tonsillitis?
Enlarged, red tonsils with exudate
Normal-sized tonsils
Small, pale tonsils
White patches on the tongue
-
What is the first choice analgesia for children with tonsillitis?
Aspirin
Codeine
Ibuprofen
Paracetamol
-
What is a common symptom of acute mastoiditis?
Persistent and severe pain
Ringing in the ears
Nausea
Mild headache
-
Which sign is associated with acute mastoiditis?
Fever
Tenderness of the mastoid on palpation
Swollen lymph nodes
Clear nasal discharge
-
What is a possible complication of acute mastoiditis?
Earwax buildup
Sinusitis
Subperiosteal abscess over the mastoid antrum
Tonsillitis
-
What is the recommended treatment for acute mastoiditis?
Topical ointments
Oral pain relievers
IV antibiotics (Amoxicillin, Metronidazole)
Home rest
-
What does the swelling of the post auricular region indicate?
Acute mastoiditis
Ear canal infection
Chronic otitis media
Allergic reaction
-
What is the appearance of the mastoid region in acute mastoiditis?
Dry and flaky
Clear and normal
Swollen and erythematous
Pale and cold
-
What can happen to the pinna in acute mastoiditis?
It may turn blue
It may shrink in size
It may be pushed forward and downwards
It may become detached
-
What is a Bezold abscess?
Pus breaks through the mastoid tip and passes into the neck
Fluid accumulation in the ear
Swelling of the jaw
Infection of the throat
-
-
What is a common indication for performing a cortical mastoidectomy?
Hearing loss
Severe headache
Presence of a periosteal abscess
Nasal congestion
-
What symptom indicates an emergency referral for a sore throat?
Mild fever
Stridor and respiratory difficulty
Sore throat
Cough
-
-
Which of the following is NOT a nutritional deficiency associated with mouth ulcers?
Folic acid
Vitamin D
Iron
Vitamin B12
-
Which condition is associated with recurrent mouth ulcers?
Recurrent Aphthous Stomatitis (RAS)
Chicken Pox
Leukaemia
HIV
-
What are the characteristics of oral cavity ulceration?
Small painful, shallow and round/oval lesions
Large deep lesions
Lesions with pus
Painless lesions
-
Which of the following is a potential infective cause of mouth ulcers?
Behcet's disease
Crohn's disease
Herpetic Stomatitis
Anemia
-
What is the source of the image depicting mouth ulcers?
An x-ray of the jaw
A photograph of a healthy mouth
A close-up of a tongue with a white ulcer
A diagram of a throat
-
What is a common cause of mouth ulcers related to cutaneous diseases?
Sharp tooth
Denture
Mucosal SCC
Lupus Erythematous
-
Which investigation is first line for suspected malignancy in mouth ulcers?
Iron studies
FBC
B12 and Folate
Biopsy
-
-
-
Which bacteria is most commonly associated with bacterial pharyngitis?
Haemophilus influenzae
Group A Streptococci
Staphylococcus aureus
Escherichia coli
-
What symptom is associated with acute tonsillitis and pharyngitis?
Chest pain
Throat pain
Headache
Nausea
-
What is a common symptomatic treatment for mouth ulcers?
Topical steroids
Chemotherapy
Surgery
Radiation therapy
-
What symptom is less likely in Group A Strep compared to Viral Pharyngitis?
Sore throat
Cough
Vomiting in children
Fever
-
-
Which age group receives a score of 1 in the Centor Criteria?
3-14 yr
0-2 yr
15-44 yr
45 yr or older
-
What is the suggested management for a score of 3 in the Centor Criteria?
Culture all
Treat empirically with antibiotics
Perform culture
No further testing
-
What is a common symptom of both Group A Strep and Viral Pharyngitis?
Days of cough/rhinorrhoea
Fever
Vomiting in children
Sore throat
-
What does a score of ≥4 indicate in the Centor Criteria?
1%-2.5%
51%-53% risk of Streptococcal Infection
5%-10%
11%-17%
-
What are the complications of Group A Streptococcus (GAS) pharyngitis?
Sinusitis and otitis media
Laryngitis and epiglottitis
Rheumatic fever and glomerulonephritis
Pneumonia and bronchitis
-
What is the sensitivity of rapid streptococcal tests for diagnosing GAS pharyngitis?
Approximately 85%
Approximately 95%
Approximately 100%
Approximately 75%
-
What is the recommended sampling technique for rapid streptococcal tests?
Gentle samples from the uvula
Vigorous samples of both tonsils and posterior pharynx
Swabbing the soft palate only
Only anterior tonsil samples
-
What is the typical duration for symptoms of GAS pharyngitis to resolve spontaneously?
1-2 days
5-7 days
1 week
3-4 days
-
What is the main treatment approach for infectious mononucleosis?
Chemotherapy
Antibiotics
Supportive care
Surgery
-
Which virus is primarily responsible for infectious mononucleosis?
Epstein Barr Virus (EBV)
Cytomegalovirus (CMV)
Herpes Simplex Virus (HSV)
Human Immunodeficiency Virus (HIV)
-
What should be avoided in the treatment of infectious mononucleosis due to the risk of rash?
Ibuprofen
Aspirin
Amoxicillin
Penicillin
-
What is a common non-infectious cause of pharyngitis?
Mouth-breathing due to nasal obstruction
Viral infection
Bacterial infection
Allergy
-
What symptom is commonly associated with mouth-breathing pharyngitis?
Nasal congestion
Persistent cough
Sore throat worse in the morning
Ear pain
-
-
What is shown in the image related to glandular fever?
Red throat without exudate
Swollen lymph nodes
Normal tonsils
Heavy exudate over entire tonsils
-
-
Which symptom is NOT typically associated with a peritonsillar abscess?
Severe dysphagia
Trismus
Referred otalgia
Foetor
-
What is a common treatment for a peritonsillar abscess?
Cold compresses
Rest and hydration
Antibiotics
Surgery immediately
-
What may require drainage in a peritonsillar abscess?
Presence of trismus
Mild sore throat
Absence of fever
Normal tonsil size
-
What medication is suggested for treating a peritonsillar abscess?
Amoxicillin only
Co-amoxiclav IV
Ciprofloxacin
Ibuprofen
-
What is a sign of a peritonsillar abscess?
Enlarged lymph nodes
Fever only
Swollen uvula
Medial displacement of the tonsil
-
-
-
-
What is the recommended course of antibiotics for a peritonsillar abscess?
Ten-day course
Only topical antibiotics
One-day course
Five-day course of oral antibiotics
-
What is epiglottitis primarily characterized by?
Acute inflammation in the supraglottic region
Inflammation of the stomach lining
Infection of the nasal passages
Chronic inflammation of the lungs
-
What is a common position for a patient with epiglottitis?
Lying flat
Tripod position
Sitting back in a chair
Leaning to the side
-
Which organism is classically associated with epiglottitis in children?
Streptococcus pneumoniae
Escherichia coli
Staphylococcus aureus
Haemophilus influenzae type b
-
What is a late finding indicating advanced airway obstruction in epiglottitis?
Drooling
Cough
Fever
Stridor
-
What is the immediate management for an unstable patient with epiglottitis?
Nebulized steroids
Intubation or tracheostomy
IV fluids
Oral antibiotics
-
-
What treatment is given to stable patients with epiglottitis?
Oral pain relief
Intranasal decongestants
Topical antiseptics
IV steroids and antibiotics
-
What physical finding involves a patient sitting up with their tongue out?
Fowler's position
Tripod position
Lateral recumbent position
Supine position
-
What is a common symptom of epiglottitis that indicates respiratory distress?
Headache
Hypoxia
Nausea
Fatigue
-
What should patients suspected of having epiglottitis be referred for?
Routine check-up
X-ray imaging
Blood tests
ENT evaluation
-
What is the most common cause of sore throat?
Throat cancer
Allergic reactions
Bacterial infections
Viral infections
-
Which bacteria is a common cause of bacterial pharyngitis?
Streptococcus pneumoniae
Staphylococcus aureus
Escherichia coli
Group A strep
-
-
What does the Modified CENTOR Criteria assess?
Type of bacteria
Presence of fever
Risk of streptococcal infection
Severity of pain
-
What is the recommended treatment for a confirmed streptococcal infection?
Penicillin V
Clarithromycin
Ibuprofen
Dexamethasone
-
What complication can arise from untreated streptococcal pharyngitis?
Stroke
Diabetes
Heart attack
Rheumatic fever
-
Which condition is characterized by a grey membrane in the throat?
Thyroiditis
Quinsy
Diphtheria
Epiglottitis
-
-
-
What is a severe sign of sore throat requiring immediate attention?
Sore throat
Airway compromise
Mild fever
Nausea
-
What should be done if pus is drained from a peritonsillar abscess?
Discharge immediately
Start antibiotics
Schedule a follow-up
Admit and refer to ENT
-
-
-
What is the first-line treatment for a patient with a severe sore throat and suspected EBV?
Paracetamol
Clarithromycin
Ibuprofen
Benzylpenicillin
-
What should be prepared for a patient with airway compromise?
Antibiotics
Difficult airway trolley
Pain relief
IV fluids
-
What is the purpose of the flow chart in the management of sore throat?
To list medications
To summarize symptoms
To diagnose all conditions
To guide treatment decisions
-
What is a common non-suppurative complication of streptococcal infection?
Quinsy
Glomerulonephritis
Otitis media
Sinusitis
-
What is the age factor in the Modified CENTOR Criteria?
Age < 20 years +1
Age 30-44 years +1
Age > 65 years +2
Age > 44 years -1
-
-
What should be done if dysphonia persists for more than 3 weeks?
Advise voice rest
Perform a laryngoscopy
Prescribe antibiotics
Refer to ENT specialist
-
What is the main treatment for acute laryngitis?
Radiation therapy
Conservative treatment
Surgery
Antibiotics
-
-
What is the role of speech therapy in chronic laryngitis?
Improve lung capacity
Increase vocal range
Re-educate correct voice use
Cure the infection
-
Which condition can present with laryngeal complications in up to 30% of patients?
GORD
Diabetes
Asthma
Hypertension
-
What should be assessed during the examination of a patient with dysphonia?
Travel history
Family history of allergies
Previous surgeries
Risk factors for malignancy
-
What is the purpose of the flowchart in the diagnosis of dysphonia?
Provide patient education
Illustrate differential diagnosis
List medications
Show treatment options
-
What is a cholesteatoma?
A benign tumor in the ear canal
A fluid-filled sac in the outer ear
A type of ear infection
A cystic mass lined with keratin in the middle ear
-
-
What are common presentations of cholesteatoma?
Headaches, facial swelling, fever
Dizziness, tinnitus, ear ringing
Otalgia, otorrhoea, deafness
Nasal congestion, sore throat, cough
-
What can advanced cholesteatoma cause?
Sinus infection
Eustachian tube dysfunction
Hearing improvement
Facial nerve paralysis
-
What are the two types of acquired cholesteatoma?
Primary and secondary
Mild and severe
Chronic and acute
Simple and complex
-
What is a possible complication of cholesteatoma?
Tinnitus
Mastoiditis
Earwax blockage
Otitis externa
-
What is a primary cause of cholesteatoma?
Earwax buildup
Retraction pocket on tympanic membrane
Acute otitis media
Allergic rhinitis
-
What is one theory regarding the pathogenesis of cholesteatoma?
Allergic reaction
Viral infection
Increased earwax production
Trapping of desquamation material in retraction pockets
-
What can advanced cholesteatoma lead to in terms of hearing?
Improved hearing
Temporary hearing loss
Complete deafness
Reduced hearing due to ossicular involvement
-
What is a common imaging finding in cholesteatoma?
Thickened tympanic membrane
Absence of the cochlea
Cystic mass in the middle ear
Fluid in the outer ear
-
What is a potential serious infection associated with cholesteatoma?
Pharyngitis
Meningitis
Sinusitis
Bronchitis
-
What is the histopathological feature of cholesteatoma?
Cystic mass with only lymphocytes
Cystic mass lined with keratin producing squamous epithelium
Fluid-filled sac with no epithelium
Solid mass of connective tissue
-
What are the components of the cholesteatoma perimatrix?
Epithelial cells and lymphocytes
Fibroblasts, macrophages and capillaries
Osteoblasts and osteoclasts
Only keratinocytes
-
Which bacteria are commonly associated with aerobic superinfection in cholesteatoma?
E. coli, Klebsiella, Bacillus
Bacteroides, Fusobacterium, Peptococcus
Streptococcus, Enterococcus, Clostridium
Pseudomonas, Staphylococcus, Proteus
-
What is the mainstay surgical procedure for cholesteatoma treatment?
Fistula repair
Mastoidectomy
Myringotomy
Tympanoplasty
-
What is a conservative management option for patients unfit for cholesteatoma surgery?
Antibiotic therapy
Corticosteroid injections
Regular microsuction to remove keratin and debris
Radiation therapy
-
What can enhance the biologic profile of the cholesteatoma perimatrix?
Surgical intervention
Cholesterol reduction
Superinfection
Antibiotic treatment
-
What is one of the treatment options for bacterial superinfection in cholesteatoma?
Amoxicillin
Vancomycin
Azithromycin
Ciprofloxacin
-
What is a consequence of the cholesteatoma perimatrix secreting metalloproteinases?
Bone erosion
Decreased inflammation
Bone formation
Increased infection resistance
-
What are the two main categories of complications arising from middle ear disease?
Intratemporal and Intracranial
Mild and Severe
Acute and Chronic
Localized and Systemic
-
Which of the following is a sequela of middle ear disease?
Throat pain
Hearing loss
Nasal congestion
Tinnitus
-
-
-
Which complication involves the 5th cranial nerve?
Labyrinthitis
Mastoiditis
Facial nerve paralysis
Petrositis
-
What is a sign of labyrinthitis?
Hearing loss
Ear discharge
Facial swelling
Nystagmus towards the diseased side
-
What are common systemic effects of subdural/extradural abscesses?
Fatigue
Pyrexia
Malaise
Nausea
Dizziness
-
-
What is the management for subdural/extradural abscess?
Observation only
IV Antibiotics and surgical intervention
Oral antibiotics only
Physical therapy
-
What should alert a clinician to the possibility of a tumor in facial nerve palsy?
Headache
New onset parotid lump
Ear pain
Facial twitching
-
What grading system is used for facial nerve dysfunction?
House Brackmann
Bristol Stool Chart
Wong-Baker FACES
Glasgow Coma Scale
-
What is the most common cause of facial nerve palsy?
Tumor
Idiopathic (Bell's Palsy)
Trauma
Infection
-
Which type of facial nerve palsy spares the forehead?
Complete paralysis
Upper motor neuron
Lower motor neuron
Partial paralysis
-
What is a possible aetiology for upper motor neuron palsy?
Herpes virus
Mastoiditis
Vascular e.g. aneurysm
Bell's Palsy
-
What does a progression beyond 3 weeks or lack of improvement beyond 6 months suggest?
malignant cause
bacterial infection
viral infection
benign condition
-
Which condition is associated with hearing loss in Ramsay Hunt syndrome?
otitis media
Bell's palsy
Meniere's disease
Acoustic neuroma
-
What comorbidity is noted to predispose to infection?
Chronic kidney disease
Diabetes
Asthma
Obesity
-
-
What is an important consideration for eye care in facial nerve palsy?
eye patching all day
use of artificial tears
avoidance of light
daily eye drops
-
What is the initial treatment recommended for facial nerve palsy?
antibiotics
physiotherapy
surgery
high dose steroid
-
Which grading system is used to track facial nerve palsy recovery?
House Brackmann system
Glasgow Coma Scale
Barthel Index
Fugl-Meyer Assessment
-
What should be done if no resolution occurs after 3 weeks?
perform surgery
start chemotherapy
consider referral to ENT
discontinue treatment
-
What is the most common form of otitis externa (OE)?
Otomycosis
Acute diffuse OE
Necrotizing OE
Chronic OE
-
Which type of otitis externa is associated with infection of a hair follicle?
Acute localized OE (furunculosis)
Eczematous OE
Chronic OE
Acute diffuse OE
-
What is a key characteristic of necrotizing (malignant) otitis externa?
Associated with atopic dermatitis
Infection extends into deeper tissues
Most common in swimmers
Caused by fungi
-
Which organism is commonly associated with otitis externa?
Streptococcus pneumoniae
Escherichia coli
Pseudomonas aeruginosa
Staphylococcus aureus
-
What symptom is commonly observed in otitis externa?
Hearing loss
Itching progressing to pain
Nausea
Severe headache
-
What type of otitis externa encompasses various dermatologic conditions?
Eczematous (eczematoid) OE
Necrotizing OE
Acute diffuse OE
Acute localized OE
-
What is a common diagnostic step for otitis externa?
X-ray of the skull
Blood test for allergies
CT scan of the brain
Swab for culture and sensitivity
-
Which condition is a fungal infection of the ear canal?
Eczematous OE
Otomycosis
Acute diffuse OE
Chronic OE
-
What is a common finding in the ear canal during examination of otitis externa?
Pus-filled cysts
Presence of wax
Diffuse erythema and edema
Clear fluid
-
What is the purpose of topical steroids in the treatment of otitis externa?
To dry the ear
To reduce oedema
To numb the pain
To treat fungal infections
-
Which medication is effective against Pseudomonas aeruginosa?
Neomycin
Clotrimazole
Gentamicin
Ciprofloxacin
-
What should patients avoid doing while treating otitis externa?
Wearing ear plugs
Keeping the ear dry
Applying topical antibiotics
Using cotton buds in the ear
-
Which drug is known to cause dose-related deafness if the tympanic membrane is perforated?
Ciprofloxacin
Hydrocortisone
Dexamethasone
Aminoglycosides
-
What is the role of ENT in severe cases of otitis externa?
Prescribing oral antibiotics
Providing topical treatments
Performing surgery
Micro suction and cleaning under the microscope
-
What is malignant otitis externa (MOE)?
A rare potentially fatal inflammatory disease of the external auditory canal
A type of skin cancer
A benign growth in the ear
A common ear infection
-
Which patients are most commonly affected by malignant otitis externa?
Immunocompromised or diabetic patients
Elderly patients only
Healthy individuals
Children under 5 years
-
What are the common symptoms of malignant otitis externa?
Mild earache, no fever
Nasal congestion
High fever, granulation tissue in EAC, severe pain
Sore throat
-
What is a major complication of malignant otitis externa?
Sinusitis
Otitis media
Meningitis
Tinnitus
-
How is malignant otitis externa diagnosed?
Otoscopy, elevated ESR, CT or MRI
Physical examination alone
Blood pressure measurement
X-ray only
-
What is the emergency treatment for malignant otitis externa?
Oral painkillers only
IV antibiotics +/- surgical debridement
Topical antibiotics only
No treatment needed
-
What is the aetiology of furunculosis in the external auditory meatus?
Viral infection
Bacterial infection from swimming
Fungal infection
Staphylococcus aureus infection of a hair follicle
-
What can nasal furunculosis lead to if not treated properly?
Nasal congestion
Facial cellulitis and cavernous sinus thrombosis
Allergic rhinitis
Earwax buildup
-
What are the symptoms of nasal furunculosis?
Itching and dryness
Pain, erythema, and oedema
Sore throat
Nasal bleeding
-
What is a common treatment for furunculosis?
Systemic anti-staphylococcus antibiotics – penicillin
Topical antifungals
Antihistamines
Corticosteroids
-
What is a common cause of traumatic tympanic membrane perforation?
Infection
Barotrauma
Allergy
Cold weather
-
Which of the following is a possible aetiology for tympanic membrane perforation?
Foreign bodies
Flu
Sinusitis
Earwax
-
What is a key diagnostic feature of traumatic tympanic membrane perforation?
Ragged edges
Smooth edges
Clear fluid
No bleeding
-
-
Which activity is associated with tympanic membrane perforation due to barotrauma?
Walking
Reading
Cooking
Water sports
-
What is a symptom of tympanic membrane perforation?
Coughing
Nasal congestion
Sore throat
Evidence of recent haemorrhage
-
What does figure 24 show?
A perforated tympanic membrane with blood
A foreign body in the ear
An ear infection
A healthy tympanic membrane
-
What may cause tympanic membrane perforation from a slap on the ear?
Cold air
Infection
Barotrauma
Dust
-
What is the first step in evaluating a patient with suspected ear perforation?
Examination of the ear
Performing a hearing test
Administering antibiotics
Scheduling surgery
-
What should be documented if the perforation is clearly seen during an ear examination?
Size and shape of the perforation
Presence of infection
Hearing level
Patient's age
-
What is a pathognomonic sign of a temporal bone fracture in a patient with a head injury?
Hearing loss
Ear discharge
Facial nerve palsy
CSF leakage
-
What is the recommended action if the tympanic membrane perforation is contaminated?
Perform immediate surgery
Ignore the contamination
Consider antibiotic treatment
Wait for spontaneous healing
-
What is the relationship between the size of a tympanic membrane perforation and healing?
All perforations heal equally
Smaller perforations have a greater chance of healing
Larger perforations heal faster
Size does not affect healing
-
What defines sudden onset sensorineural hearing loss?
Loss of 10 decibels over one week
Gradual loss of hearing over months
Complete hearing loss immediately
Loss of 30 decibels or more over three frequencies within three days
-
What is the incidence of sudden onset sensorineural hearing loss?
50 per 100,000
20 per 100,000
1 per 100,000
8 per 100,000
-
Which of the following is a potential infectious cause of sudden onset sensorineural hearing loss?
Acoustic neuroma
Multiple sclerosis
Diabetes
Herpes zoster
-
What type of hearing loss is defined as sudden onset sensorineural hearing loss?
Mixed hearing loss
Sensorineural hearing loss
Permanent hearing loss
Conductive hearing loss
-
What is a common treatment strategy for tympanic membrane perforation?
Perform self-cleaning of the ear
Apply heat to the ear
Use earplugs at all times
Keep water out of the ears
-
What should history focus on when evaluating hearing loss?
Only medications
Various aetiologies including medications, recent trauma, and infections
Only medical history
Only recent trauma
-
What is a key examination step for conductive hearing loss?
Neurological examination
Vision test
Physical examination of the throat
Otoscopy for conductive blockage
-
What type of investigation is performed on the day of presentation for hearing loss?
Audiogram
Blood glucose test
Hearing test with a tuning fork
MRI of the brain
-
Which tests are included in the haematological investigations?
FBC, ESR, Glucose, HbA1c
Only HbA1c
Only Glucose
Only FBC
-
What is the recommended steroid treatment for idiopathic sensory neural hearing loss?
1mg prednisolone/kg/day for 10 days
1mg prednisolone/kg/day for 5 days
5mg prednisolone/kg/day for 5 days
10mg prednisolone/kg/day for 10 days
-
What percentage of patients with sudden sensory neural hearing loss spontaneously recover?
50%
25%
10%
75%
-
What does improvement at 1-2 weeks indicate about hearing loss prognosis?
It does not affect prognosis
It guarantees full recovery
It indicates immediate surgery is needed
It may predict long-term prognosis
-
What is a caution when using high dose steroids in patients?
Only in elderly
Only in pregnant women
Elderly, diabetic, or those with a history of psychosis
Only in diabetics
-
What imaging is performed for suspected intracranial pathology?
MRI of brain and internal acoustic meatus
CT scan of the chest
Ultrasound of the head
X-ray of the skull
-
What is the significance of the audiogram in the treatment of hearing loss?
It shows improvement after steroid treatment
It indicates the need for surgery
It only shows initial hearing loss
It is irrelevant to treatment
-
What is an acoustic neuroma also known as?
Vestibular schwannoma
Acoustic sarcoma
Cochlear tumor
Neurofibroma
-
-
Which cranial nerve is affected by an acoustic neuroma?
5th cranial nerve
6th cranial nerve
7th cranial nerve
8th cranial nerve
-
What is a risk factor for developing an acoustic neuroma?
Diabetes
Hypertension
Asthma
Neurofibromatosis 2 (NF2)
-
What is a common symptom of acoustic neuroma?
Memory loss
Asymmetrical sensorineural hearing loss
Vision loss
Nausea
-
What examination method is used to test hearing in suspected cases of acoustic neuroma?
Endoscopy
CT scan
Blood test
Tuning fork
-
Which symptom involves hearing buzzing or repetitive sounds?
Tinnitus
Vertigo
Headache
Facial numbness
-
-
What is a red flag symptom for tinnitus that warrants referral to ENT?
Pulsatile tinnitus
Hearing loss
Chronic headache
Bilateral tinnitus
-
-
Which condition is associated with pulsatile tinnitus?
Meniere's
Acoustic trauma
Otosclerosis
Vascular pathology
-
What is a common non-troublesome cause of tinnitus?
Vestibular schwannoma
Otosclerosis
Conductive hearing loss
Idiopathic tinnitus
-
Which medication class is known to cause tinnitus?
Antibiotics
Antihistamines
Ototoxic drugs
Antidepressants
-
What should be examined in the tympanic membrane during a tinnitus assessment?
Identifiable cause of conductive hearing loss
Color of the membrane
Presence of wax
Shape of the ear
-
What is a psychosocial impact of tinnitus?
Hearing enhancement
Increased appetite
Sleep disturbance
Improved concentration
-
Which condition may be suggested by vertigo and sensory neural hearing loss with tinnitus?
Otosclerosis
Benign intracranial hypertension
Meniere's
Acoustic neuroma
-
What is the most common finding in audiograms related to hearing loss?
Acoustic neuroma
Ear infection
Age-related degeneration in hearing (high frequency)
Sudden hearing loss
-
-
Which of the following is a peripheral cause of vertigo?
Multiple sclerosis
Migraine
Benign Paroxysmal Positional vertigo (BPPV)
Cerebellar stroke
-
What does the mnemonic S.P.I.N.D.A.R help examine?
Vestibular system
Hearing ability
Cerebellar system
Visual acuity
-
Which condition is characterized by excess fluid in the inner ear?
Acoustic neuroma
Labyrinthitis
BPPV
Meniere's Disease
-
What type of nystagmus is associated with central causes of vertigo?
Rotatory nystagmus
Horizontal nystagmus
Vertical nystagmus
No nystagmus
-
What is a common cause of vertigo following a viral infection?
Sinusitis
Infection of the vestibular apparatus
Acoustic neuroma
Middle ear infection
-
What is a symptom of Benign Paroxysmal Position Vertigo (BPPV)?
Vertigo lasting for hours
Hearing loss
Severe headache
Vertigo lasting for seconds
-
What does the HINTS mnemonic help assess in a cerebellar examination?
Hearing loss
Vestibulo-ocular reflex
Balance disorders
Nystagmus
-
What are the symptoms of Meniere's disease?
Nystagmus, vertigo, tinnitus
Hearing loss only
Vertigo, tinnitus, hearing loss, aural fullness
Dizziness, nausea, headaches, fatigue
-
What is the main treatment for acute attacks of Meniere's disease?
Surgery
Hearing aids
Epley manoeuvre
Vestibular sedatives
-
What is the cause of BPPV?
Inner ear infection
Migraine
Vestibular neuritis
Dislodging of otoconia into semicircular canals
-
What maneuver is diagnostic for BPPV?
Epley manoeuvre
Cover/uncover test
Dix Hallpike manoeuvre
HINTS test
-
What is the primary treatment for BPPV?
Betahistadine
Epley manoeuvre
Vestibular sedatives
Steroid injections
-
What lifestyle changes are recommended for managing Meniere's disease?
Reduce salt, caffeine, alcohol, and stop smoking
Increase salt intake
Avoid exercise
Consume more caffeine
-
What does a vertical movement of the eye during the cover/uncover test suggest?
Hearing loss
Normal vestibular function
Peripheral cause of vertigo
Central cause of vertigo
-
What is the most common cause of vestibular neuritis?
Fungal infection
Allergic reaction
Bacterial infection
Herpes simplex virus
-
What are common symptoms of vestibular neuritis?
Chest pain, cough, fatigue
Acute-onset vertigo, nausea, vomiting
Headache, fever, rash
Loss of smell, sore throat, ear pain
-
What is the primary treatment for vestibular neuritis?
Antibiotics
Supportive care and vestibular inhibitors
Corticosteroids
Surgery
-
What prevents nasal regurgitation of food during swallowing?
Opening of the epiglottis
Elevation of the soft palate
Contraction of the diaphragm
Closure of the vocal cords
-
How does the nasal cavity help in breathing?
Filters out carbon dioxide
Reduces air temperature
Cleans and humidifies air
Increases air pressure
-
What lines the respiratory surfaces in the nose and paranasal sinuses?
Respiratory mucous membrane
Simple squamous epithelium
Skin epithelium
Cuboidal epithelium
-
What is the role of the ciliated columnar epithelium in the nasal cavity?
To help move mucus and debris out of the airways
To absorb nutrients
To facilitate gas exchange
To produce mucus
-
What is the relationship between rhinitis and asthma?
Rhinitis is a symptom of asthma
They are completely unrelated
They should be treated as a unified functional unit
Asthma only occurs in children
-
What is Sinusitis?
A type of headache
A skin condition
An infection of the throat
Inflammation of the paranasal sinuses
-
What is the duration that defines acute Rhinosinusitis?
<blockquote>
12 weeks
</blockquote>
1 week
6 months
<12 weeks
-
Which of the following is NOT a type of Rhinosinusitis?
Nasal polyposis
Allergic
Vasomotor
Acute Infective
-
What is a common consequence of a viral common cold?
Sinus cancer
Nasal polyps
Acute rhinosinusitis
Chronic rhinosinusitis
-
Which condition can lead to primary ciliary abnormality?
Cystic fibrosis
Kartageners syndrome
Allergic rhinitis
Asthma
-
Which of the following is a clinical feature of Acute Rhinosinusitis?
Weight loss
Nasal congestion
Fever
Skin rash
-
What is a serious risk associated with Acute Rhinosinusitis?
Common cold
Life-threatening complications
Seasonal allergies
Nasal dryness
-
-
What is the main reason for prescribing antibiotics in rhinosinusitis?
To alleviate allergies
To manage bacterial infections
To reduce inflammation
To treat viral infections
-
What are the paranasal sinuses illustrated in the provided diagram?
Temporal and occipital sinuses
Nasal and oral sinuses
Frontal, ethmoid, sphenoid, and maxillary sinuses
Cranial and thoracic sinuses
-
-
-
Which sinusitis may radiate pain to the teeth?
Maxillary sinusitis
Sphenoid sinusitis
Frontal sinusitis
Ethmoidal sinusitis
-
What does frontal sinus pain typically present as?
Directly over the affected sinus
At the vertex
Radiating to the teeth
Near the eyes
-
How many symptoms are needed to diagnose rhinosinusitis?
At least two symptoms
One symptom
Four symptoms
Three symptoms
-
Which symptom is NOT part of the rhinosinusitis diagnosis criteria?
Cough
Blockage/congestion
Reduced sense of smell
Facial pain/pressure
-
What is a necessary sign for diagnosing rhinosinusitis?
Endoscopic signs
Fever
Nasal bleeding
Ear pain
-
-
Where is pus or obstruction primarily found in rhinosinusitis?
Middle meatus
Nasal passages
Sphenoid sinuses
Frontal sinuses
-
What are mucosal changes in relation to in rhinosinusitis diagnosis?
Ears
Nasal cavity
Throat
Osteomeatal complex and/or sinuses
-
What does the diagram in Figure 27 illustrate?
Symptoms of rhinosinusitis
Anatomy of the sinuses
Referred pain patterns from different sinuses
Types of sinusitis
-
What symptom is associated with allergic rhinosinusitis but not infectious rhinosinusitis?
Congestion
Sneezing
Discharge
Hyposmia
-
Which type of rhinosinusitis may have colored discharge?
Neither type
Both types
Infectious rhinosinusitis
Allergic rhinosinusitis
-
What is a common treatment for bacterial rhinosinusitis?
Nasal decongestants
Topical steroids
Antihistamines
Amoxicillin
-
What type of hypersensitivity reaction is involved in allergic rhinitis?
Type 4
Type 2
Type 3
Type 1
-
Which of the following is NOT a common allergen for allergic rhinitis?
Pollen
House dust mites
Pollutants
Animal dander
-
What does the EPOS 2020 guidelines focus on regarding acute rhinosinusitis?
Management pathways for acute rhinosinusitis
Long-term medication for sinusitis
Surgical treatments for sinusitis
Home remedies for sinusitis
-
What is a recommended non-medical treatment for allergic rhinitis?
Use decongestants
Take antihistamines
Remove bedroom carpeting
Use nasal sprays
-
Which testing method is used to identify specific allergens in allergic rhinitis?
Skin prick testing
Blood pressure testing
X-ray imaging
MRI scanning
-
What should be done to bed clothes to manage dust mite allergies?
Use fabric softener
Wash at greater than 60 degrees
Dry clean only
Wash in cold water
-
What is one of the alarm symptoms for acute bacterial rhinosinusitis (ABRS)?
Mild congestion
Itchy eyes
Severe headache
Sneezing
-
-
Which of the following is a surgical treatment indication for allergic rhinitis?
Mild symptoms
Nasal congestion
Seasonal allergies
Unresponsive to medical treatment
-
What type of abscess can occur as a complication of acute rhinosinusitis?
Brain abscess
Lung abscess
Kidney abscess
Liver abscess
-
According to ARIA guidelines, what should be considered in the management of allergic rhinitis?
Gender of patient
Severity of symptoms
Geographic location
Age of patient
-
Which complication of acute rhinosinusitis affects the eyes?
Retinal detachment
Glaucoma
Cataract
Periorbital cellulitis
-
What is a possible bone complication of acute rhinosinusitis?
Bone fracture
Rheumatoid arthritis
Osteomyelitis
Osteoporosis
-
What is represented in the flowchart related to allergic rhinitis management?
Guidelines for sinus surgery
Treatment options for asthma
Diagnosis and management based on symptoms
Management of nasal polyps
-
What is a nasal complication of acute rhinosinusitis?
Nasal polyp
Deviated septum
Septal perforation
Mucocele
-
What is periorbital cellulitis commonly caused by?
Acute sinusitis
Trauma
Dacryocystitis
Insect bites
-
What is a major risk associated with untreated post septal cellulitis?
Hearing loss
Skin necrosis
Blindness
Facial paralysis
-
-
What are the most common pathogens in periorbital cellulitis?
E. coli and Klebsiella
Staphylococci and Streptococci
Candida and Aspergillus
Pseudomonas and Bacillus
-
What symptoms suggest post septal cellulitis?
Nasal congestion
Sore throat
Reduced visual acuity
Cough
-
What is a common treatment for periorbital cellulitis?
IV antibiotics
Topical steroids
Cold compresses
Oral antihistamines
-
What is the significance of the lamina papyracea in periorbital cellulitis?
It allows direct spread of infection
It is a surgical procedure
It prevents infection
It is a type of antibiotic
-
Which symptom indicates possible optic neuritis?
Ear pain
Nasal bleeding
Fever
Reduced colour vision
-
What is a possible complication of untreated orbital cellulitis?
Cavernous sinus thrombosis
Hypertension
Asthma
Diabetes
-
-
What is cavernous sinus thrombosis (CST)?
An infection of the lungs
A type of brain tumor
A stroke
Formation of a blood clot within the cavernous sinus
-
What are common presentations of cavernous sinus thrombosis?
Headaches
Nausea
High fever
Sepsis
Loss of vision
Dizziness
-
What is the mortality rate without antibiotics for cavernous sinus thrombosis?
50-70%
10-15%
20-30%
80-100%
-
What is a common treatment for cavernous sinus thrombosis?
Physical therapy
Radiation therapy
Antibiotics
Surgery
-
What anticoagulation therapy options are available for CST?
Unfractionated IV heparin and fractionated low-molecular-weight SC heparins
Warfarin and aspirin
Clopidogrel and rivaroxaban
Enoxaparin and dabigatran
-
What are the symptoms required for a diagnosis of chronic rhinosinusitis?
Nasal obstruction only
Only reduction in smell
Only facial pain
Two or more symptoms including nasal blockage or discharge
-
How long must symptoms be present to diagnose chronic rhinosinusitis?
6 weeks
8 weeks
Greater than 12 weeks
Less than 4 weeks
-
What percentage of the general population is affected by chronic rhinosinusitis?
10-15%
5-12%
1-3%
15-20%
-
-
What imaging technique is commonly used in the examination of chronic rhinosinusitis?
CT Scan
X-ray
PET Scan
MRI Scan
-
Which test may be performed if allergies are suspected in chronic rhinosinusitis?
Ultrasound
X-ray
Blood pressure test
Skin prick test
-
What does Functional Endoscopic Sinus Surgery (FESS) aim to achieve in chronic rhinosinusitis management?
Permanent cure of all sinus issues
Complete removal of sinuses
Restitution of physiology
Only cosmetic improvement
-
Which of the following is NOT a criterion for Functional Endoscopic Sinus Surgery (FESS)?
Facilitates mucociliary clearance
Creates a sinus cavity that incorporates the natural ostium
Facilitates instillation of topical therapies
Allows adequate sinus ventilation
-
What is one of the management steps for chronic rhinosinusitis outlined in the EPOS 2020 care pathways?
Only medication
Avoiding all therapies
Immediate surgery
Self-care
-
What does FESS facilitate for ongoing care in chronic rhinosinusitis?
Use of antibiotics only
Instillation of topical therapies
Surgical intervention
Long-term hospitalization
-
What is depicted in the flowchart for chronic rhinosinusitis management?
Care pathways for CRS
Dietary recommendations
Surgical techniques
Historical treatment methods
-
What is one of the rare inflammatory sinonasal diseases associated with systemic illness?
Rhinorrhea
Granulomatosis with polyangiitis (Wegner's)
Epistaxis
Saddle deformity
-
Which of the following is NOT a symptom of granulomatous sinonasal disease?
Saddle deformity
Crusting
Rhinorrhea
Congestion
-
What type of diagnostic test is used for suspected granulomatous sinonasal disease?
Ultrasound
MRI
Full blood count
Liver function tests
-
Which imaging technique is used in the workup for granulomatous sinonasal disease?
CT scan of the abdomen
MRI
Ultrasound
Chest X-Ray
-
-
What type of biopsy is performed if the initial investigations are inconclusive?
Skin biopsy
Bone marrow biopsy
Liver biopsy
Histological biopsy
-
-
What is one of the systemic investigations for granulomatous sinonasal disease?
Blood glucose
ANCA
Thyroid function tests
Vitamin D levels
-
What is a common nasal sign of granulomatous disease?
Septal perforation
Nasal polyps
Sinusitis
Allergic rhinitis
-
What does the diagnostic workup for granulomatous sinonasal disease include?
Lipid profile
Endoscopy
Chest ultrasound
Urinalysis
-
What is Granulomatous with Polyangiitis also known as?
Eosinophilic Granulomatosis
Churg Strauss Syndrome
Granulomatosis with Polyangiitis
Wegener's
-
What is a characteristic feature of Granulomatous with Polyangiitis?
Pulmonary infiltrates
Asthma
Necrotising granulomas of the respiratory tract
Eosinophilia
-
What is the mean age of incidence for Granulomatous with Polyangiitis?
30 years
60 years
50 years
40 years
-
What type of antibodies are associated with Granulomatous with Polyangiitis?
Anti Nuclear Antibody (ANA)
Anti-DNA Antibodies
Anti Neutrophil Cytoplasmic Antibody (ANCA)
Rheumatoid Factor
-
What percentage of patients with Granulomatous with Polyangiitis experience complete remission with treatment?
50%
65%
90%
75%
-
-
What is one of the main treatments for Granulomatous with Polyangiitis?
Antibiotics alone
Surgery
Combination of Steroids + Cyclophosphamides
Radiation therapy
-
What is the triad of symptoms associated with Churg Strauss Syndrome?
Asthma, systemic vasculitis, eosinophilia
Fever, cough, fatigue
Chest pain, dyspnea, wheezing
Nasal congestion, sneezing, anosmia
-
What is the incidence rate of Churg Strauss Syndrome?
1-2/100,000
2-3/100,000
3-4/100,000
5-10/100,000
-
-
What is the definition of sarcoidosis?
A type of cancer
A bacterial infection
An autoimmune disorder
A multisystem inflammatory disease with noncaseating granulomas
-
What is the incidence rate of sarcoidosis?
20-25 per 100,000
30-35 per 100,000
10-15 per 100,000
5-10 per 100,000
-
Which demographic has a higher incidence of sarcoidosis?
Caucasians
Afro-Caribbeans and Scandinavians
Asians
Native Americans
-
What is a common presentation of sarcoidosis?
Skin rashes only
Headaches
Nausea and vomiting
Pulmonary complaints like cough and dyspnoea
-
-
What treatment is commonly used for sarcoidosis?
Radiation therapy
Systemic steroids and immune suppression
Surgery
Antibiotics
-
What is a significant histological finding in sarcoidosis?
Eosinophilia
Caseating granulomas
Necrotising granulomas
Vasculitis
-
Which condition is associated with systemic lupus erythematosus?
Nasal polyps
Non-granulomatous sinonasal conditions
Asthma
Chronic rhinosinusitis
-
-
-
What is a potential immune dysregulation finding in sarcoidosis?
Raised B-cells
Decreased antibodies
Low T-cells
High neutrophils
-
Which age groups are most affected by sarcoidosis?
20-30 and 40-50
25-35 and 45-65
30-40 and 50-60
15-25 and 35-45
-
What type of granulomas are predominantly found in sarcoidosis?
Noncaseating granulomas
Necrotising granulomas
Eosinophilic granulomas
Caseating granulomas
-
What systemic complaint is experienced by 45% of sarcoidosis cases?
Fever and anorexia
Joint pain
Skin rashes
Headaches
-
What is a specific mucosal change associated with sarcoidosis?
Swelling of the tongue
Granulations and yellow submucosal nodules in the nose
Nasal congestion
Bleeding gums
-
Which of the following is a non-granulomatous sinonasal condition?
Behcet's disease
Chronic rhinosinusitis
Lupus pernio
Sarcoidosis
-
What is a characteristic feature of eosinophilia?
Decreased white blood cells
Decreased red blood cells
Increased eosinophil count in blood
Increased neutrophils
-
-
Which systemic condition is NOT associated with sinonasal symptoms?
Relapsing polychondritis
NK-cell lymphoma
Behcet's disease
Lupus pernio
-
What is the main cause of immune dysregulation in sarcoidosis?
Genetic mutation
Bacterial infection
Unknown aetiology
Viral infection
-
What does the table in the document list?
Treatment options for sarcoidosis
Types of sarcoidosis
Non-granulomatous sinonasal conditions associated with systemic disease
Symptoms of sarcoidosis
-
What are the two types of epistaxis based on the location of the bleed?
Internal and External
Anterior and Posterior
Left and Right
Acute and Chronic
-
Which plexus is associated with anterior epistaxis?
Woodruff's plexus
Sphenopalatine plexus
Kiesselbach's plexus
Ophthalmic plexus
-
What is the common age distribution for epistaxis?
30 to 40 and 60 to 70 years
0 to 5 and 50 to 60 years
Younger than 10 and 70 to 79 years
20 to 30 and 40 to 50 years
-
What is the primary blood supply for Kiesselbach's plexus?
Branches from Brachiocephalic artery
Branches from External Carotid artery
Branches from Subclavian artery
Branches from Internal Carotid artery
-
Which condition is a traumatic cause of epistaxis?
Leukemia
Vitamin K deficiencies
Hemophilia
Facial trauma
-
What is a common infectious cause of epistaxis?
Polycythemia vera
Thrombocytopenia
Sinusitis
Aplastic anemia
-
Which of the following is a disorder of hemostasis that can cause epistaxis?
Digital trauma
Environmental irritants
Upper respiratory infection
Hemophilia
-
What is the most frequent treatment for anterior epistaxis?
General anaesthesia
Nasal packing
Cautery under local anaesthesia
Observation only
-
Which plexus is associated with posterior epistaxis?
Kiesselbach's plexus
Ophthalmic plexus
Woodruff's plexus
Sphenopalatine plexus
-
What is one of the major arteries supplying the nasal septum?
Sphenopalatine artery
Facial artery
Subclavian artery
Brachiocephalic artery
-
What is a common benign tumor that can cause epistaxis?
Metastatic lesions
Benign nasal polyps
Juvenile angiofibroma
Nasopharyngeal neoplasms
-
What is one of the treatments for posterior epistaxis?
Nasal packing
Topical medications
Observation only
Cautery under local anaesthesia
-
What is a contributing factor to epistaxis related to environmental exposure?
Aplastic anemia
Environmental irritants
Thrombocytopenia
Leukemia
-
What is a common age range for epistaxis to occur?
Younger than 10 and 70 to 79 years
50 to 60 years
30 to 40 years
20 to 30 years
-
What is the role of the greater palatine artery in epistaxis?
It is a cause of epistaxis
It is used for cauterization
It is involved in nasal packing
It supplies blood to the nasal septum
-
Which of the following is an infectious cause of epistaxis?
Trauma
Leukemia
Tuberculosis
Environmental irritants
-
What is the primary anatomical challenge in posterior epistaxis?
Age of the patient
Type of bleeding
Duration of bleeding
Anatomical location
-
What is the most common treatment for posterior epistaxis?
Cautery under local anaesthesia
Observation only
Topical medications
Management under general anaesthesia
-
What is the relationship between the External Carotid artery and epistaxis?
It is a cause of epistaxis
It only supplies posterior epistaxis
It supplies both plexuses involved in epistaxis
It is irrelevant to epistaxis
-
What is a key contributing factor to epistaxis in children?
Leukemia
Digital trauma
Hemophilia
Vitamin K deficiencies
-
-
What is the purpose of cautery in treating epistaxis?
To diagnose the cause
To promote healing
To prevent infection
To stop the bleeding
-
What is depicted in the image related to epistaxis?
A treatment guide for epistaxis
A list of causes of epistaxis, including trauma, tumors, infections, and disorders of hemostasis.
Statistics on epistaxis incidence
Anatomical diagrams of the nasal cavity
-
What is a common aetiology for epistaxis related to medications?
Antidepressants
Antibiotics
Anticoagulants medications
Antihistamines
-
Which congenital condition is an uncommon aetiology for epistaxis?
Haemophilia
Hypertension
Diabetes
Asthma
-
What initial assessment is imperative in managing epistaxis?
MRI
ABC Assessment
Blood pressure measurement
CT scan
-
Which of the following is a sign to check for during assessment of epistaxis?
Signs of haemorrhagic shock
Signs of dehydration
Signs of infection
Signs of allergy
-
What should be done to control bleeding in epistaxis?
Use nasal spray
Apply manual compression on nostrils
Tilt head back
Apply ice pack on forehead
-
What is a method for treating anterior bleeding in epistaxis?
Oral antihistamines
Antibiotic treatment
Nasal packing with gauze
Nasal cautery with silver nitrate
-
What history taking aspect is vital to rule out contributing factors for epistaxis?
Travel history
Medication history
Family history
Diet history
-
What should be assessed if trauma is suspected in epistaxis?
Abdominal injury assessment
Neck injury assessment
Chest injury assessment
Head injury assessment
-
What is the purpose of a nasal tampon in epistaxis management?
To expand in the nasal cavity and apply pressure
To clean the nasal cavity
To numb the nasal area
To prevent infection
-
Which agent can be prescribed to prevent toxic shock syndrome when nasal packing is used for 24+ hours?
Acetaminophen
Ibuprofen
Amoxicillin
Ciprofloxacin
-
What is BIPP used for in nasal packing?
To promote healing
Advanced nasal packing
To anesthetize the area
To clean the nasal cavity
-
What is Floseal used for in epistaxis management?
Cleaning the nasal cavity
Numbing the area
Preventing infection
Controlling epistaxis
-
What procedure may be required if epistaxis is persistent?
Antibiotic administration
Examination Under General Anaesthesia
Nasal tampon insertion
Use of nasal spray
-
What is one of the options for controlling epistaxis in centers with Interventional Radiology?
Use of nasal sprays
Embolization of artery
Electrocauterization
Nasal packing
-
What is the function of the Rapid Rhino device in nasal packing?
To administer medication
To apply pressure to the nasal cavity
To provide anesthesia
To clean the nasal cavity
-
What is the recommended position for inserting a nasal tampon?
Along the septum
Vertically
At an angle
Against the palate
-
What is Reinke's oedema primarily caused by?
Emotional stress
Hypothyroidism
Cigarette smoking
Viral infection
-
What is a common treatment for early stages of Reinke's oedema?
Voice therapy
Antibiotics
Stopping smoking and voice rest
Surgical intervention
-
What condition can cause hoarseness due to vocal cord oedema?
Hypothyroidism
Muscle tension dysphonia
Vocal cord paralysis
Reinke's oedema
-
Which nerve is more often affected in unilateral vocal cord paralysis?
Left recurrent laryngeal nerve
Vagus nerve
Right recurrent laryngeal nerve
Phrenic nerve
-
What is a potential complication of bilateral vocal cord palsy?
Airway compromise
Vocal fatigue
Hoarseness
Dysphagia
-
What examination can confirm unilateral vocal cord palsy?
CT scan
MRI brain
Nasendoscopy
Cranial nerve examination
-
-
What is a common idiopathic cause of vocal cord paralysis?
Nuclear palsy
Vascular injury
Thyroid malignancy
Idiopathic
-
What is the most commonly used material for Injection Medialisation Techniques in vocal cord palsy treatment?
Hydroxyapatite
Collagen
Glycerin
Silicone
-
What is the normal salivary production per day?
1 - 2 litres
0.5 - 1.5 litres
0.2 - 0.5 litres
1.5 - 2.5 litres
-
What is Sialadenitis?
Obstruction of the airway
Inflammation of salivary glands
Infection of the throat
Tumor in the salivary glands
-
Which condition can cause bilateral vocal cord palsy?
Chronic bronchitis
Asthma
Iatrogenic trauma
Pneumonia
-
What are common symptoms of Sialadenitis?
Erythema over the area
Hoarseness
Dry mouth
Difficulty swallowing
-
What can be a treatment option for airway obstruction in bilateral cord palsy?
Antibiotics
Inhalers
Tracheostomy
Surgery
-
What is a common cause of Sialadenitis?
Bacterial infection
Viral infection
Allergic reaction
Autoimmune disease
-
What is the function of salivary glands?
Lubrication of food
Production of urine
Absorption of nutrients
Secretion of hormones
-
What can be a cause of bilateral vocal cord palsy related to congenital conditions?
Hydrocephalus
Asthma
Chronic cough
Tonsillitis
-
-
What is the medical management for acute sialadenitis?
Surgery, gland excision, radiation therapy
Hydration, antibiotics, warm compresses, massage, sialagogues
Only warm compresses and massage
Only hydration and antibiotics
-
Which gland is preferentially affected in Sjögren syndrome?
Submandibular gland
Parotid gland
Minor salivary glands
Sublingual gland
-
What is a common ENT presentation of Sjögren syndrome?
Hearing loss
Nasal congestion
Throat pain
Xerostomia
-
What is sialadenosis?
Cancer of the salivary glands
Infection of the salivary glands
Non-neoplastic noninflammatory swelling with gland hypertrophy
Formation of salivary stones
-
Which laboratory test is used to confirm Sjögren syndrome?
Autoantibodies SS-A and SS-B
Liver function test
Complete blood count
Thyroid function test
-
What is a potential complication of Sjögren syndrome affecting the CNS?
Vasculitis or demyelinating lesions
Alzheimer's disease
Parkinson's disease
Stroke
-
What are the major categories of aetiologies for sialadenosis?
Only nutritional and endocrine
Viral, bacterial, fungal, autoimmune, drug induced
Nutritional, endocrine, metabolic, inflammatory/autoimmune, drug induced
Infectious, traumatic, genetic, environmental, metabolic
-
What is the primary staging system used for head and neck tumours?
AJCC (American Joint Committee on Cancer)
UICC (Union for International Cancer Control)
FIGO (International Federation of Gynecology and Obstetrics)
TNM (Tumour, Nodes, Metastasis)
-
Which professionals are part of the Head and Neck Oncology Multidisciplinary Team?
Dermatologists, Psychologists, Nutritionists
ENT, Radiation Oncology, Medical Oncology, Radiology, Pathology, Specialist Nurses, Dieticians, Speech and Language therapists
Surgeons, General Practitioners, Physiotherapists
Oncologists, Pharmacists, Social Workers
-
Which type of tumours is NOT included in head and neck cancers?
Neurogenic
Salivary gland
Thyroid
Mucosal
-
What is the purpose of the TNM staging system?
Guides management and gives prognostic information
Only for research purposes
To determine treatment costs
To classify tumours by size
-
What types of tumours are discussed in Head and Neck Oncology MDTs?
Lung, breast, colon, prostate
Skin, muscle, bone, nerve
Brain, liver, kidney, bladder
Mucosal, thyroid, parathyroid, skin, salivary gland, vascular, neurogenic
-
What does the diagram in Figure 35 illustrate?
Treatment methods for head and neck cancers
Subtypes of head and neck cancers categorized by anatomical location
Symptoms of head and neck cancers
Statistics on cancer survival rates
-
Which of the following is a common tumour type in the head and neck region?
Liver tumours
Salivary gland tumours
Bone tumours
Breast tumours
-
What symptom indicates difficulty swallowing in patients with mucosal tumours?
Dysarthria
Odynophagia
Dysphagia
Dysphonia
-
-
What is referred otalgia related to?
Shared sensory innervation with the upper aerodigestive tract
Inflammation
Nerve damage
Infection
-
-
What sensation is referred to as globus?
Difficulty swallowing
Hoarse voice
Sensation of mass in throat
Pain swallowing
-
What should alert clinicians to potential head and neck malignancy?
Symptoms in conjunction with risk factors
Only age
Only smoking
Only weight loss
-
Which risk factors are mentioned for mucosal tumours?
Genetics
Diet and exercise
Smoking and systemic signs
Age
-
What is the main focus of the provided text?
Prevention strategies
Treatment options
Diagnosis methods
Red flag presentations of mucosal tumours
-
What does the diagram illustrate regarding referred otalgia?
Connections between various head and neck structures and the ear
Only the throat anatomy
Only the nasal anatomy
Only the ear anatomy
-
What is the most common tumor type in head and neck mucosa?
Basal Cell Carcinoma
Melanoma
Squamous Cell Cancer (SCC)
Adenocarcinoma
-
What are the premalignant lesions associated with SCC?
leukoplakia and erythroplakia
basal cell carcinoma
actinic keratosis
melanoma
-
What are the boundaries of the oral cavity?
Lips to uvula
Lips to junction of hard and soft palate
Teeth to gums
Tongue to pharynx
-
What are common causative agents for oral cavity tumors?
alcohol and diet
tobacco and HPV
viral infections
radiation and sunlight
-
What is a common presentation of oral cavity tumors?
Odynophagia and dysphagia
Fever
Nausea and vomiting
Weight loss
-
What is the mainstay of treatment for oral cavity tumors?
Surgery +/- radiotherapy
Immunotherapy
Radiotherapy only
Chemotherapy only
-
What procedure is typically required for the majority of oral cavity tumors?
Tracheostomy
Biopsy
Neck dissection
Lymph node sampling
-
What is the primary causative agent of oropharyngeal cancer?
Tobacco smoking
Alcohol consumption
Genetic mutations
Human papilloma virus (HPV)
-
What is a common presentation of oropharyngeal cancer?
Painless neck mass
Severe headache
Sore throat
Nasal congestion
-
How does HPV mediated oropharyngeal cancer compare to smoking induced cancers in terms of death risk?
60% reduction in death risk
30% reduction in death risk
Higher death risk
No difference in risk
-
What is a common treatment for oropharyngeal tumours?
Surgery +/- adjuvant radiotherapy
Only chemotherapy
Observation
Only radiotherapy
-
What is the significance of transoral robotic surgery in treating oropharyngeal tumours?
Increases the efficacy of surgery
Is less effective than traditional surgery
Decreases recovery time
Eliminates the need for chemotherapy
-
What anatomical boundaries define the oropharynx?
Junction of soft palate and hard palate to the level of the hyoid bone
Nasal cavity to the soft palate
Base of skull to the hyoid bone
Pharyngeal walls only
-
What are the two types of nasopharyngeal cancers?
Benign and malignant tumours
Melanoma and lymphoma
Squamous cell carcinoma and adenocarcinoma
Non-keratinising (NKSCC) and keratinising (KSCC) tumours
-
What is a common risk factor for Non-keratinising nasopharyngeal cancer?
Alcohol exposure
Epstein Barr Virus (EBV)
Genetic (HLA I)
Smoking
-
What is the main treatment for hypopharyngeal tumours?
Radiotherapy
Surgery
Chemotherapy
Immunotherapy
-
What is a common presentation of hypopharyngeal tumours?
Nasal obstruction
Dysphagia
Epistaxis
Painless neck mass
-
What is the primary risk factor for hypopharyngeal cancer?
Nitrosamines
Genetic factors
Epstein Barr Virus
Smoking
-
-
What is a co-factor associated with hypopharyngeal cancer?
Nitrosamines
Genetic predisposition
Alcohol
EBV
-
What is the typical presentation of nasopharyngeal cancer?
Sore throat
Cough
Painless neck mass
Hoarseness
-
What surgical procedure may be required for very advanced hypopharyngeal tumours?
Tracheostomy
Tonsillectomy
Pharyngo-laryngo-oesophagectomy (PLO)
Laryngectomy
-
What are the primary roles of the larynx?
Hearing, taste, smell
Breathing, digestion, circulation
Speech, swallowing, airway protection
Movement, balance, coordination
-
What is the term for premalignant tumours in the larynx?
Papilloma
Carcinoma in situ
Leukoplakia
Dysplasia
-
-
How are early stage tumours (T1) managed?
Surgery or radiotherapy
Total laryngectomy
Observation
Chemotherapy only
-
What is the recommended treatment for advanced tumours (T4)?
Radiotherapy only
Surgery only
Total laryngectomy and radiotherapy
Chemotherapy only
-
What are the subdivisions of the larynx based on the vocal cords?
Anterior, posterior, lateral
Supraglottic, glottic, subglottic
Superior, inferior, medial
Cervical, thoracic, abdominal
-
What symptoms may present in advanced laryngeal tumours?
Fatigue, muscle pain, joint pain
Dysphonia, dysphagia, weight loss
Nausea, vomiting, diarrhea
Fever, cough, headache
-
-
What type of image shows laryngeal cancer?
CT scan of the abdomen
Photograph showing white growths on vocal cords
X-ray of the chest
MRI of the brain
-
What is a significant benefit of adding chemotherapeutic agents to radiotherapy?
Reduced treatment time
Increased pain
Improved local control and overall survival
Less need for surgery
-
What is the larynx primarily composed of?
Cartilaginous framework
Bone structure
Connective tissue
Muscular tissue
-
What is a laryngectomy?
Removal of the larynx and separation of the airway from the mouth, nose, and esophagus
Insertion of a tracheostomy tube
Surgery to repair vocal cords
Removal of the trachea
-
What is a major consequence of laryngectomy regarding breathing?
The patient can breathe normally through the mouth
The patient becomes an obligate neck breather
The patient requires a ventilator
The patient can still phonate normally
-
Which of the following is NOT a complication of laryngectomy?
Fistulae
Haematoma
Nerve injury
Chyle leak
-
-
What is the purpose of a tracheo-oesophageal puncture?
To create a passage between the trachea and the esophagus
To improve breathing
To prevent food aspiration
To enhance vocal cord function
-
What device can be used for alaryngeal speech after laryngectomy?
Electrolarynx
Respirator
Hearing aid
Pacemaker
-
What happens to the vocal cords after a laryngectomy?
They are enhanced
They are lost
They function normally
They are repaired
-
What is a stoma in the context of laryngectomy?
A type of vocal cord
An opening created for breathing
A breathing mask
A surgical tool
-
What type of speech will patients have after a laryngectomy?
Alaryngeal speech
Whispered speech
Normal speech
Enhanced speech
-
What is shown in the diagram comparing normal anatomy with post-laryngectomy anatomy?
The heart and lungs
The pharynx, larynx, trachea, and esophagus
The stomach and intestines
The brain and spinal cord
-
What device is used to produce speech after a laryngectomy by allowing air from the lungs to pass through it?
Laryngeal mask
Tracheostomy tube
Electrolarynx
Voice prosthesis
-
What is the purpose of a tracheoesophageal puncture (TEP) in speech production?
To enhance sound production
To replace vocal cords
To block airflow to the lungs
To allow airflow from the trachea to the esophagus
-
Which part of the body is involved in airflow during the use of an electrolarynx?
Lungs
Heart
Kidneys
Stomach
-
In airflow with a tracheoesophageal puncture, what does air pass through before entering the esophagus?
A valve
The trachea
The pharynx
The vocal cords
-
What should all medical personnel be familiar with regarding laryngectomy patients?
Surgical procedures
Emergency management
Long-term rehabilitation
Speech therapy
-
How should laryngectomy patients be oxygenated or intubated?
They cannot be intubated or oxygenated from the nose/mouth.
They can be oxygenated via the nose.
They can be intubated via the mouth.
They can use a standard mask.
-
What type of signage should be found at the bedside of laryngectomy patients?
Dietary restrictions
Patient history forms
Overbed signs and algorithms
Medication charts
-
What information is included on the laryngectomy signage?
Patient's name, age, allergies
Date, tube size, hospital number, notes, emergency contact
Insurance information, family contacts
Doctor's name, treatment plan, follow-up
-
What is the primary focus of training for laryngectomy patients before discharge?
Psychological counseling
Management of their condition
Dietary changes
Physical therapy
-
What is the first step in managing a laryngectomy emergency?
Call for airway expert help
Apply high flow oxygen to face
Assess laryngectomy stoma patency
Perform tracheal suction
-
What should be used to assess the airway if available?
Manual resuscitation bag
Suction catheter
Oxygen mask
Waveform capnography
-
If the patient is not breathing, what should be done next?
Perform CPR immediately
Call for help
Ventilate via stoma
Administer medication
-
What should you do if the laryngectomy stoma is patent?
Deflate the cuff
Perform tracheal suction
Remove the tube from the stoma
Apply oxygen to the face
-
What is a primary emergency oxygenation method for a laryngectomy patient?
Bag-mask ventilation
Nasal cannula
Paediatric face mask applied to stoma
Oxygen via mouth
-
What should you consider using for intubation of a laryngectomy stoma?
Laryngeal mask airway
Endotracheal tube without cuff
Oral airway
Small tracheostomy tube / 6.0 cuffed ETT
-
What is a tracheostomy?
A method of intubation
A type of lung surgery
A procedure to remove the larynx
The surgical formation of an opening into the trachea through the anterior neck
-
What is one indication for performing a tracheostomy?
Chest tube insertion
Long term ventilation
Short term sedation
Laryngeal surgery
-
Which anesthesia can be used for a surgical tracheostomy?
Only local anesthesia
Sedation only
Local anesthesia (LA) or general anesthesia (GA)
Only general anesthesia
-
What type of incision can be made for a tracheostomy?
Diagonal
Horizontal or vertical
Lateral
Circular
-
What is the first step in performing a surgical tracheostomy?
Inserting the tracheostomy tube
Making a skin incision in the anterior neck
Disconnecting the ventilator
Placing a stay suture
-
What is included in the parts of a tracheostomy tube?
Laryngeal mask, connector, shaft
Endotracheal tube, cuff, balloon
Ventilator, tube, cuff
15 mm connector, cuff, flange, shaft, distal tip
-
What is a potential complication of a tracheostomy?
High bleeding risk
Pneumonia
Low oxygen levels
Infection at the incision site
-
What is a potential immediate complication of a tracheostomy?
Granulation tissue formation
Paratracheal insertion (false passage)
Tracheomalacia
Vocal cord paralysis
-
What are early complications of tracheostomy?
Loss of airway
Infection
Accidental decannulation
Bleeding
Tracheal stenosis
Tracheo-oesophageal fistula
Delayed stoma closure
-
What is a late complication of tracheostomy?
Tracheomalacia
Aspiration
Accidental decannulation
Subcutaneous emphysema
-
What is the purpose of the cuff in a tracheostomy tube?
To allow ventilation (closed circuit created)
To enable speech
To prevent infection
To prevent aspiration
-
What is a disadvantage of using a cuffed tracheostomy tube?
Facilitates swallowing
Allows for better ventilation
Prevents air reaching vocal cords, hence patients cannot speak
Reduces risk of infection
-
When should a cuffless tube be used after tracheostomy?
Immediately after surgery
As soon as ventilation is no longer required and there is no risk of aspiration
Only if the patient requests it
When the patient is fully awake
-
How is the cuff of a tracheostomy tube deflated?
By using a needle
Automatically after a set time
By cutting the tube
Using a syringe
-
What is a risk of failure of decannulation?
Complete recovery
Improved airway function
Permanent tracheostomy
Reduced risk of infection
-
What is the purpose of fenestrations in a tracheostomy tube?
Increases airway resistance
Promotes airflow through upper airway allowing phonation
Prevents aspiration
Facilitates mucus retention
-
What is a crucial function of the inner cannula in a tracheostomy tube?
Blocks mucus plugs
Facilitates cleaning while maintaining the airway
Prevents phonation
Increases airflow resistance
-
What can occur if fenestrations are not properly positioned in the airway?
Easier phonation
Increased airflow
Decreased risk of blockage
Aspiration and granulation tissue
-
What happens if the tracheostomy becomes blocked with a mucus plug?
Airway resistance decreases
Phonation is enhanced
The inner cannula can be removed
The outer cannula must be replaced
-
What should be placed above the bed of every patient with a tracheostomy?
A patient history report
A list of medications
A sign with details of their procedure, indication, and tube
A daily schedule
-
What is included in the 'Trachy Box' by the bedside?
Patient's medical records
Suctioning equipment only
Emergency contact numbers
Necessary supplies for accidental decannulation
-
What training do patients receive upon getting a tracheostomy?
Training on suctioning and managing their own tubes
Training on dietary needs
Training on physical therapy
Training on medication management
-
Why is it important for healthcare professionals to know about tracheostomy management?
To handle emergencies effectively
To perform surgeries
To prescribe medications
To conduct physical exams
-
What do algorithms developed for tracheostomy management help with?
Conducting routine check-ups
Determining medication dosages
Guiding management in emergency situations
Scheduling patient appointments
-
What should be done first if a patient with a tracheostomy is breathing?
Perform tracheal suction
Remove inner tube
Apply high flow oxygen
Call Resuscitation Team
-
What indicates a patent or partially patent airway during assessment?
Waveform capnography
Chest X-ray
Blood pressure monitoring
Pulse oximetry
-
What should be used to cover the stoma during emergency oxygenation?
Swabs or hand
Oral airway
Oxygen mask
Bag-valve-mask
-
What is the next step if you cannot pass a suction catheter through the tracheostomy?
Call Resuscitation Team
Remove inner tube
Deflate the cuff
Perform tracheal suction
-
If the tracheostomy tube is partially obstructed, what should be done?
Apply high flow oxygen
Attempt oral intubation
Remove the tracheostomy tube
Continue ABCDE assessment
-
What should be done if the patient is not breathing and the tracheostomy tube is patent?
Ventilate via tracheostomy
Remove the tracheostomy tube
Perform CPR
Deflate the cuff
-
When should the tracheostomy tube be removed?
If the patient is stable
If the patient is not stable or improving
If the tube is patent
If the patient is breathing
-
Which device can be used for secondary emergency oxygenation?
Oral airway adjuncts
Bag-valve-mask
Supraglottic airway device (e.g. LMA)
Paediatric face mask
-
What is a potential tool for intubation of the stoma?
Aintree catheter
Suction catheter
Endotracheal tube
Bag-valve-mask
-
What should be assessed at the mouth and tracheostomy?
Call for help
Perform CPR
Look, listen & feel
Apply high flow oxygen
-
What is the purpose of using waveform capnography in tracheostomy management?
To assess oxygen saturation
To monitor heart rate
To measure blood pressure
To indicate airway patency
-
What is the most common location for Acinic cell carcinoma?
Submandibular gland
Sublingual gland
Parotid
Buccal mucosa
-
What percentage of salivary gland malignancies does Acinic cell carcinoma represent?
15-20%
8-14%
20-30%
1-5%
-
Which imaging modality is 96% sensitive in diagnosing Adenoid Cystic carcinoma?
CT
Ultrasound
PET
MRI
-
What is a common presentation symptom of salivary gland malignancies?
Painless mass
Severe headache
Vision changes
Nausea
-
Which salivary gland malignancy is characterized by slow growth and excellent prognosis?
Acinic cell carcinoma
Mucoepidermoid
Lymphoma
Adenoid Cystic
-
What is the demographic trend for Adenoid Cystic carcinoma?
More common in children
Men more than women in 30-40s
Women more than men in 40-60s
Equal in both genders
-
Which imaging technique helps assess infiltration and lymph nodes in salivary gland malignancies?
PET
X-ray
MRI
CT
-
What is a common association with salivary gland malignancies?
Metastatic nodes from Skin Ca
Asthma
Hypertension
Diabetes
-
What percentage of salivary tumors does Adenoid Cystic carcinoma represent?
5-10%
10-22%
15-25%
20-30%
-
What are common symptoms associated with salivary gland malignancies?
Chest pain
Severe dizziness
Persistent cough
CN VII palsy or paralysis
-
-
Which two locations are most commonly affected by metastasis?
Lung and Bone
Skin and Muscle
Kidney and Pancreas
Liver and Brain
-
What is the most common type of salivary gland malignancy?
Adenoid cystic carcinoma
Pleomorphic adenoma
Acinic cell carcinoma
Mucoepidermoid carcinoma
-
What is the survival rate for low/intermediate grade mucoepidermoid carcinoma after surgery?
80-90%
60-70%
30-40%
40-50%
-
What is the most common benign salivary gland tumor?
Pleomorphic adenoma
Mucoepidermoid carcinoma
Adenoid cystic carcinoma
Warthin's tumor
-
-
What is the typical presentation of pleomorphic adenomas?
Firm and fixed lump
Soft and mobile mass
Slow growing painless lump
Rapidly growing painful mass
-
What is the facial nerve's involvement in pleomorphic adenomas?
Affected in all cases
Frequently involved
Very rarely affected
Always affected
-
What are the three histological grades of mucoepidermoid carcinoma?
Benign, Malignant, Transitional
Low, Intermediate, High
Simple, Complex, Mixed
Mild, Moderate, Severe
-
What type of treatment is typically given for high-grade mucoepidermoid carcinoma?
Radiotherapy only
Surgery +/- Selective Nodal Dissection +/- radiotherapy
Chemotherapy only
Surgery alone
-
What is the risk of pleomorphic adenomas transforming into malignant tumors over 15 years?
5%
20%
15%
10%
-
What is the prognosis for carcinoma ex-pleomorphic after transformation?
30% 5-year survival
50% 5-year survival
40% 5-year survival
60% 5-year survival
-
What is the most common treatment for pleomorphic adenomas?
Observation
Radiation therapy
Chemotherapy
Parotidectomy
-
-
What is the survival rate for differentiated thyroid cancer (DTC) over 10 years?
80-85%
92-98%
60-65%
70-75%
-
-
What clinical feature indicates a higher risk of thyroid cancer?
Painless mass
Small size
Soft nodule
Firm nodule
-
What should be checked in haematology for medullary thyroid cancer?
Free T4
Thyroglobulin
TSH
Calcitonin/CEA
-
What classification is used for ultrasound assessment of thyroid nodules?
B Classification
C Classification
A Classification
U Classification
-
Which of the following is a characteristic of benign thyroid nodules?
Solid hypo-echoic
Lobulated outline
Intra-nodular vascularity
Peripheral vascularity
-
What is a feature of suspicious thyroid nodules?
Micro-cystic
Peripheral vascularity
Solid, hypo-echoic
Cystic change
-
-
What is a feature of malignant thyroid nodules?
Iso-echoic
Peripheral egg shell calcification
Cystic change
Solid, hypo-echoic, lobulated outline
-
What does 'de-differentiation' refer to in thyroid tumors?
The size of the tumor
The type of cancer
The degree of carcinoma deviation from normal cells
The location of metastasis
-
What is a characteristic associated with papillary thyroid cancer?
High aggressiveness
No metastasis
Good prognosis
Poor prognosis
-
What is the first step in the investigation of thyroid nodules if suspicious?
Clinical exam
TFTS
Document cytology score
US guided FNA if nodule >10mm
-
-
What is the most common treatment for thyroid cancer?
Radioactive iodine
Total thyroidectomy
US guided FNA
Diagnostic hemi-thyroidectomy
-
Which of the following is NOT a criterion for a completion thyroidectomy?
Clinically negative lymphadenopathy in neck
Multifocal
Low risk
Tumours > 4cm
-
What is the purpose of radioactive iodine in adjuvant treatment?
Increase hormone levels
Destroy metastasis and residual tissue
Prevent recurrence
Reduce tumor size
-
What is the effective method for monitoring local recurrence in thyroid cancers?
MRI
X-ray
US neck
CT scan
-
What biological marker is used for monitoring papillary and follicular thyroid cancers?
TSH
Calcitonin
T3
Thyroglobulin
-
-
Follicular thyroid cancer arises from which type of cells?
Thyroid parafollicular cells
Thyroid medullary cells
Thyroid C cells
Thyroid follicular cells
-
What is the initial surgery for patients with follicular neoplasms?
Hurtle cell removal
Total thyroidectomy
Thyroid lobectomy
External beam radiotherapy
-
Which type of thyroid cancer is more likely to develop lung and bone metastases?
Hurtle cell cancer
Medullary thyroid cancer
Papillary thyroid cancer
Follicular thyroid cancer
-
What percentage of patients with FTC have metastases beyond cervical or mediastinal areas on initial presentation?
11%
20%
25%
5%
-
What treatment is indicated for aggressive or advanced follicular thyroid cancer?
Adjuvant Radioactive iodine
Chemotherapy
Hormone therapy
Observation
-
What is the significance of a RET mutation in medullary thyroid cancer?
More RET mutation = more aggressive tumor
RET mutation indicates benign tumor
Less RET mutation = more aggressive tumor
RET mutation has no significance
-
Which symptoms are associated with medullary thyroid cancer?
Nausea and vomiting
Hair loss and skin rash
Flushing and diarrhea
Weight gain and fatigue
-
What is the recommended treatment if invasive FTC is found on the final histologic section?
Only observation
Completion of thyroidectomy
No further treatment
Adjuvant chemotherapy
-
What is the monitoring approach for follicular thyroid cancer?
Same as papillary thyroid cancer
No monitoring needed
Only blood tests
More frequent imaging
-
What is the classification of medullary thyroid cancer in terms of prevalence?
10-15% of thyroid malignancies
0.5-1% of thyroid malignancies
1-3% of thyroid malignancies
5-10% of thyroid malignancies
-
When is external beam radiotherapy (EBRT) indicated?
When the patient refuses surgery
For all thyroid cancers
If all gross disease cannot be resected
Only for benign conditions
-
What is measured to investigate Medullary thyroid cancer?
Calcitonin & CEA
RET proto-oncogene
24 urinary Catecholamines
Serum Calcium & PTH
-
What is the primary management for Medullary thyroid cancer?
Observation
Chemotherapy only
Total Thyroidectomy & level VI neck dissection
Palliative care
-
What is the prognosis for Anaplastic thyroid cancer?
Average prognosis is six months
Average prognosis is nine months
Average prognosis is one year
Average prognosis is two years
-
Which imaging techniques are used for monitoring Medullary thyroid cancer?
PET scan
US, MRI, CT scanning
X-ray
Endoscopy
-
What is required if local metastatic lymph nodes are present in Medullary thyroid cancer?
Observation only
Chemotherapy
Radiation therapy
Neck dissections of these and adjacent lymphatic nodal beds
-
What should be monitored hematologically in Medullary thyroid cancer?
Calcitonin levels
Thyroid hormones
Calcium levels
Blood glucose
-
What is the primary function of parathyroid hormone (PTH)?
Blood pressure regulation
Protein synthesis
Calcium homeostasis
Insulin secretion
-
Which of the following is NOT a physiological function of calcium?
Coagulation
Cardiac automaticity
Neuromuscular transmission
Protein synthesis
-
What does parathyroid hormone do to renal calcium reabsorption?
Increases renal calcium reabsorption
Increases renal phosphate excretion
Has no effect on renal calcium reabsorption
Decreases renal calcium reabsorption
-
How does parathyroid hormone affect vitamin D3 production?
Decreases renal production of Vitamin D3
Increases intestinal absorption of Vitamin D3
Increases renal production of Vitamin D3
Has no effect on Vitamin D3
-
Which of the following processes is regulated by calcium?
Smooth muscle contraction
Digestion
Hormone secretion
Blood filtration
-
What is the effect of parathyroid hormone on phosphate levels?
Has no effect on phosphate levels
Increases phosphaturia
Increases phosphate absorption
Decreases phosphaturia
-
What role does calcium play in nerve function?
Regulates blood pressure
Facilitates nerve transmission
Has no role in nerve function
Inhibits nerve transmission
-
What is the source of calcium released into the bloodstream by parathyroid hormone?
Bone
Liver
Kidneys
Muscles
-
What is one of the roles of calcium in cell division?
Has no effect on cell division
Inhibits cell division
Promotes protein synthesis
Regulates cell movement
-
What does the diagram illustrate regarding calcium homeostasis?
Kidney filtration
Regulation by parathyroid hormone and organs
Bone structure
Calcium absorption only
-
What are common neuro-psychiatric symptoms of hypercalcaemia?
Constipation
Depression
Bone pain
Hypertension
-
What is the most common cause of secondary hyperparathyroidism?
Parathyroid carcinoma
Vitamin D deficiency
Chronic hypocalcaemia
Parathyroid adenoma
-
-
What is a common gastrointestinal symptom of hypercalcaemia?
Fatigue
Arrhythmias
Abdominal pain
Muscle weakness
-
-
What is the incidence rate of primary hyperparathyroidism?
21/100,000
50/100,000
100/100,000
10/100,000
-
What musculo-skeletal symptom is associated with hypercalcaemia?
Osteoporosis
Kidney stones
Hypertension
Anorexia
-
-
What is tertiary hyperparathyroidism caused by?
Vitamin D deficiency
Parathyroid adenoma
Chronic overstimulation of hyperplastic glands
Renal stones
-
-
What conditions should be ruled out in diagnostic considerations for hyperparathyroidism?
Cushing's Syndrome
Hyperthyroidism
Diabetes Mellitus
MEN1, MEN2a
-
What does elevated calcium in the absence of normal PTH suggest?
Hyperparathyroidism
Malignancy
Kidney stones
Vitamin D deficiency
-
What is one cause of lithium-induced hypercalcemia?
Lithium medication
Thyroid medication
Corticosteroids
High calcium diet
-
Which blood tests are essential for diagnosing hyperparathyroidism?
PTH, Calcium, Vitamin D levels
Creatinine, Uric Acid, Electrolytes
Glucose, Insulin, Hemoglobin
Lipid profile, Liver enzymes, Thyroid hormones
-
What imaging techniques are used in the investigation of hyperparathyroidism?
CT scan, Ultrasound, Bone scan
U/S, Sestamibi, 4D-CT
X-ray, MRI, PET scan
Echocardiogram, Angiogram, Fluoroscopy
-
What is the treatment of choice for primary hyperparathyroidism?
Surgical resection of the adenoma
Vitamin D analogues
Phosphate binders
Dietary phosphate restriction
-
What causes secondary hyperparathyroidism?
Vitamin D overdose
Surgical resection
Genetic mutation
Chronic abnormal stimulus
-
Which laboratory finding is expected in secondary hyperparathyroidism due to renal insufficiency?
Normal serum phosphate
High serum phosphate
Low serum calcium
High serum calcium
-
What is a common treatment for secondary hyperparathyroidism?
High-dose Vitamin D
Calcium restriction
Dietary phosphate restriction
Surgical resection
-
What characterizes tertiary hyperparathyroidism?
Absence of parathyroid hypertrophy
Continued excessive secretion of PTH despite normal or high serum calcium
Normal secretion of PTH
Low serum calcium
-
What is the effect of bisphosphonates in tertiary hyperparathyroidism?
Increased urinary calcium
Increased serum calcium
Increased BMD in spine and hip
Decreased PTH levels
-
What is the most common cause of hypercalcaemia in hospitalised patients?
Granulomatous disease
Overproduction of Vitamin D
Local osteolytic metastatic lesions
Parathyroid hormone-related peptide
-
What is the primary diagnosis indicator for hypercalcaemia of malignancy?
Normal PTH
HIGH PTH
Elevated Vitamin D
LOW PTH
-
Which type of cancer is most commonly associated with hypercalcaemia of malignancy?
Multiple myeloma
Ovarian cancer
Squamous cell lung cancer
Breast cancer
-
What percentage of hypercalcaemia cases in malignancy are due to solid tumors without metastasis?
80%
20%
100%
50%
-
Which skin cancer is described as slow-growing and locally invasive?
Squamous Cell Carcinoma
Basal Cell Carcinoma
Merkel Cell Carcinoma
Melanoma
-
What disciplines are involved in the management of sun-induced skin cancers?
Dermatology, Plastic surgery, ENT
Pediatrics, Neurology, Psychiatry
Internal Medicine, Cardiology, Dermatology
Oncology, Radiology, Pathology
-
What age group is most affected by Basal Cell Carcinoma?
7th Decade
2nd Decade
9th Decade
4th Decade
-
What is a common cause of increased serum calcium levels besides malignancy?
Granulomatous disease
Obesity
Hypertension
Diabetes
-
What is one of the humoral factors produced by tumors that can lead to hypercalcaemia?
Insulin
PTH-rP
Cortisol
Adrenaline
-
-
What is a predisposing factor for basal cell carcinoma (BCC)?
Obesity
High blood pressure
Exposure to UV radiation
Diabetes
-
Which subtype of basal cell carcinoma is considered aggressive?
Nodular
Superficial
Morphoeic
Cystic
-
What is the gold standard treatment for basal cell carcinoma?
Surgery
Chemotherapy
Immunotherapy
Radiotherapy
-
What is the recommended surgical margin for a 0-2 cm basal cell carcinoma?
10-12mm
4-5mm
1-2mm
8-10mm
-
-
Which feature is NOT a high-risk feature for basal cell carcinoma?
Poorly defined margins
Tumour size
Immunosuppression
Tumour site
-
Which subtype of basal cell carcinoma is characterized by infiltrative growth?
Infiltrative
Pigmented
Keratotic
Nodular
-
Which condition is contraindicated for radiotherapy?
Melanoma
Basal cell carcinoma
Squamous cell carcinoma
Gorlin's Syndrome
-
What is the definition of squamous cell carcinoma (SCC)?
A tumor that only occurs in the lungs
Locally invasive malignant tumor from keratinizing cells of the epidermis
A type of melanoma
A benign tumor of the skin
-
What is the second most common skin cancer?
Melanoma
Squamous cell carcinoma (SCC)
Dermatofibroma
Basal cell carcinoma
-
Which of the following is a predisposing factor for SCC?
Diabetes
High cholesterol
Chronic UV light exposure
Hypertension
-
What size of SCC tumors is three times more likely to metastasize?
Tumors < 1cm
Tumors > 2cm
Tumors = 1cm
Tumors > 5cm
-
Which histological differentiation subtype of SCC has a worse prognosis?
Well differentiated
Mildly differentiated
Poorly differentiated
Atypical
-
Which area has the greatest risk for SCC metastasis?
Back
Non-sun exposed sites
Inner thigh
Sun exposed area
-
What is a common environmental factor that can predispose someone to SCC?
Low protein diet
Vitamin D deficiency
High sugar diet
Arsenic exposure
-
Which condition is associated with a higher risk of SCC due to immunosuppression?
Asthma
High blood pressure
Diabetes
Recurrent disease
-
What is the histological subtype of SCC that is characterized by spindle cells?
Well differentiated subtype
Desmoplastic subtype
Acantholytic subtype
Spindle subtype
-
-
What is the recommended surgical margin for well-defined, low-risk tumors less than 2 cm in size?
6 mm
2 mm
4 mm
8 mm
-
For tumors larger than 2 cm, what is the required surgical margin?
2 mm
4 mm
<blockquote>
6 mm
</blockquote>
8 mm
-
What is a reason to use radiotherapy instead of surgery?
Patient prefers surgery
Small tumor size
Low risk of metastasis
Patient unfit for surgery
-
-
What is the incidence of melanoma in the USA?
21 per 100,000
15 per 100,000
7.9 per 100,000
30 per 100,000
-
Which melanoma subtype is associated with higher rates of local recurrence?
Acral lentiginous
Melanomas of the face and scalp
Desmoplastic melanoma
Nodular melanomas
-
-
What is the primary cell type involved in melanoma?
Lymphocyte
Fibroblast
Keratinocyte
Cutaneous melanocyte
-
What is an indication for radiotherapy in melanoma treatment?
Only for small tumors
Only for patients over 60
All melanoma cases
Adjuvant treatment of nodal metastasis
-
What subtype of melanoma accounts for less than 1%?
Superficial spreading
Nodular melanomas
Lentigo maligna
Acral lentiginous
-
What is a risk factor for melanoma related to the number of moles?
Exactly 100 normal moles
Only 1 normal mole
More than 100 normal moles
Less than 50 normal moles
-
Which type of melanoma is characterized by dark skin lesions on the sole of the foot?
Lentigo maligna
Superficial spreading melanoma
Acral lentiginous melanoma
Nodular melanoma
-
What hair or skin type is considered a risk factor for melanoma?
Brown hair and olive skin
Red hair or skin that burns in the sun
Black hair and dark skin
Blonde hair and tanned skin
-
What family history is a risk factor for melanoma?
Two or more cases of melanoma in first-degree relatives
One case of melanoma in second-degree relatives
Three or more cases of melanoma in distant relatives
No cases of melanoma in the family
-
What type of melanoma is depicted in the image with a close-up of a dark skin lesion?
Acral lentiginous melanoma
Nodular melanoma
Superficial spreading melanoma
Lentigo maligna
-
What is the recommended surgical margin for melanoma in situ?
5mm margin
1cm margin
2cm margin
No margin required
-
What thickness of melanoma requires a 1cm surgical margin?
Thickness ≥ 1mm
Thickness ≥ 2mm
Thickness < 1mm
Thickness ≤ 1mm
-
What thickness of melanoma requires a 2cm surgical margin?
Thickness ≤ 1mm
Thickness = 1mm
Thickness < 1mm
Thickness ≥ 1mm
-
What is the purpose of a Sentinel Lymph Node Biopsy (SLN Bx)?
Diagnosis of melanoma
Treatment of melanoma
Accurate staging of melanoma
Prevention of melanoma
-
Which patients are indicated for imaging?
Stage IIC patients without SLN bx
Stage IA patients
Stage I patients
Stage IB patients
-
What is Vemurafenib used for?
Targeted treatment for BRAF v600 positive cancers
Radiation therapy for melanoma
Chemotherapy for all cancers
Immunotherapy for all cancers