Sign up to unlock more features
- Save this deck to your account
- Study flashcards with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from PDFs and documents
- Better text extraction from your PDFs and documents
- Better flashcards with our more advanced AI model
What two components make up the cardiovascular system?
Define 'perfusion' in the context of the cardiovascular system.
What are the main functions of the cardiovascular system?
What is the primary difference in direction between arteries and veins?
What is the main role of capillaries?
What does the right side and left side of the heart receive and pump?
Name the four chambers of the heart and their basic roles.
List the great vessels that transport blood to and from the heart and one function for each.
What are the two sets of heart valves and their general function?
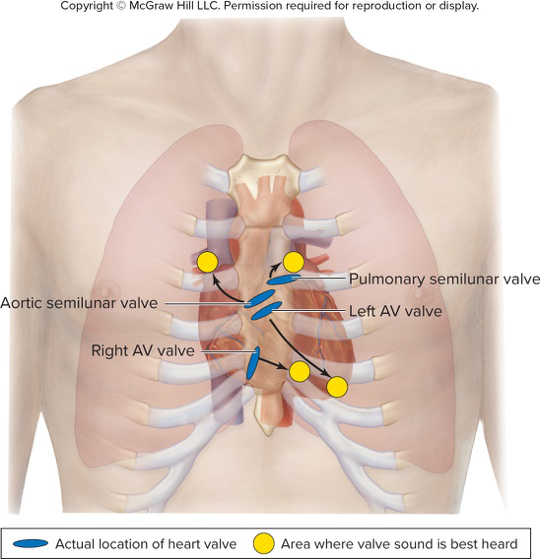
Where are the pulmonary and aortic semilunar valves located?
Refer to the circulatory diagram: which vessel type is shown exchanging gases in magnified capillaries? 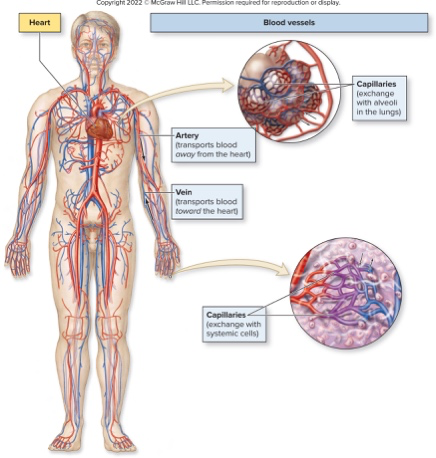
Refer to the heart anatomy diagram: name one chamber labeled in the diagram. 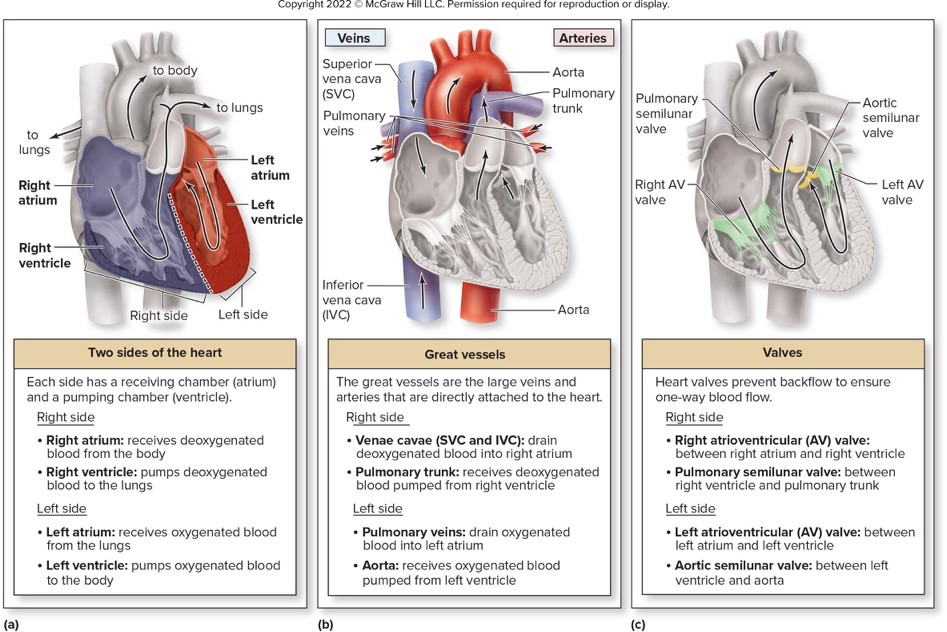
What is pulmonary circulation?
What is systemic circulation?
What is the basic overall pattern of blood flow through the heart and body?
What is congestive heart failure (CHF)?
What can cause systemic edema in heart failure?
What causes pulmonary edema in heart failure and what is its effect?
Where is the heart located and how is it oriented in the thoracic cavity?
Show an illustration of the heart's position in the thoracic cavity.
What is pericarditis?
What pathogens can cause pericarditis?
How does pericarditis lead to fluid accumulation?
What is the danger when the pericardial cavity fills with fluid?
What is a friction rub in pericarditis?
Which chambers appear most prominent on an anterior view of the heart?
Which chambers are prominent on a posterior view of the heart?
What do the coronary sulcus and interventricular sulci separate?
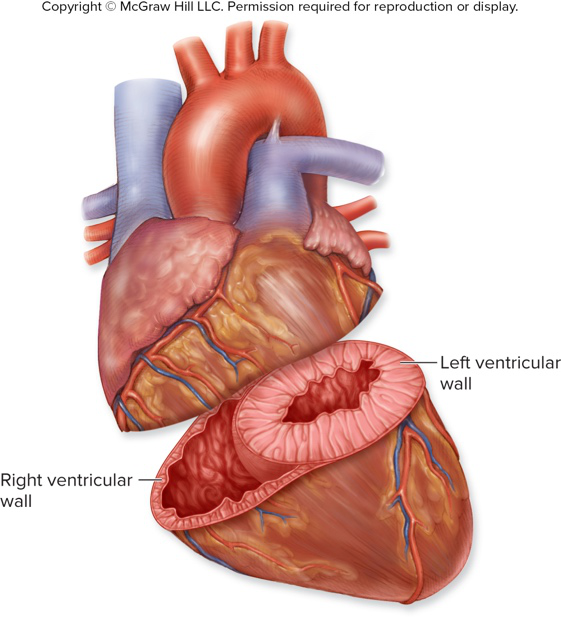
How do ventricular wall thicknesses compare and why is the left ventricle thicker?
Which structures do the grooves on the heart surface contain?
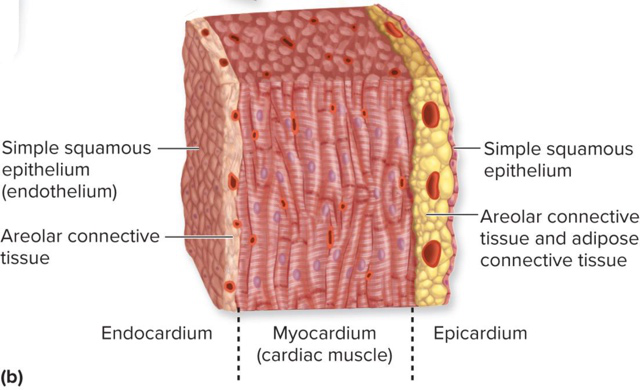
What are the three layers of the heart wall?
What tissue types compose the epicardium (visceral pericardium)?
Which heart wall layer is the thickest and what is it made of?
What tissues form the endocardium and what is its continuity?
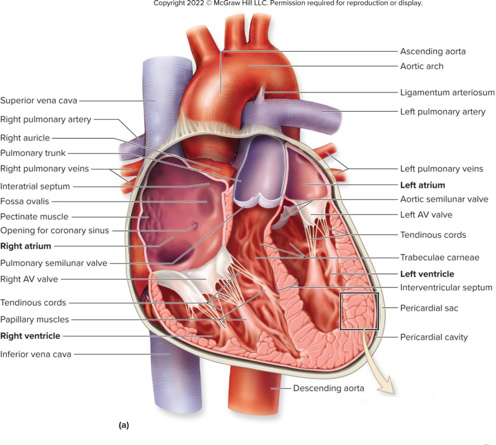
Which septum separates the left and right atria?
Which septum separates the left and right ventricles?
What are pectinate muscles and where are they found in the heart?
What is the fossa ovalis and what fetal structure did it occupy?
Name three structures that enter the right atrium.
What are trabeculae carneae and where are they located?
What are papillary muscles and their function in ventricles?
What are chordae tendineae composed of and what do they attach to?
Through which valve does blood exit the right ventricle to the pulmonary trunk?
Through which valve does blood exit the left ventricle to the aorta?
How many papillary muscles typically anchor chordae tendineae in the right ventricle and in the left ventricle?
Which atrium receives pulmonary veins and exits to the left ventricle through which valve?
Show a labeled diagram of the heart wall layers for visual reference.
Show a cross-section diagram of the heart illustrating chambers, valves, and major vessels.
What are the two main types of heart valves?
What tissue composes heart valve cusps?
Name the right atrioventricular valve and its distinguishing feature.
Name the left atrioventricular valve and its distinguishing feature.
What prevents atrioventricular valves from inverting into the atria during ventricular contraction?
How do semilunar valves close when ventricles relax?
Where is the pulmonary semilunar valve located?
Where is the aortic semilunar valve located?
Which heart sounds correspond to closing of AV and semilunar valves?
What is a heart murmur and its two main types?
What causes valvular insufficiency and its consequence?
What is valvular stenosis and its effect on cardiac output?
What is cardiomegaly and a common cause?
How does cardiac muscle enlargement affect contraction force in cardiomegaly?
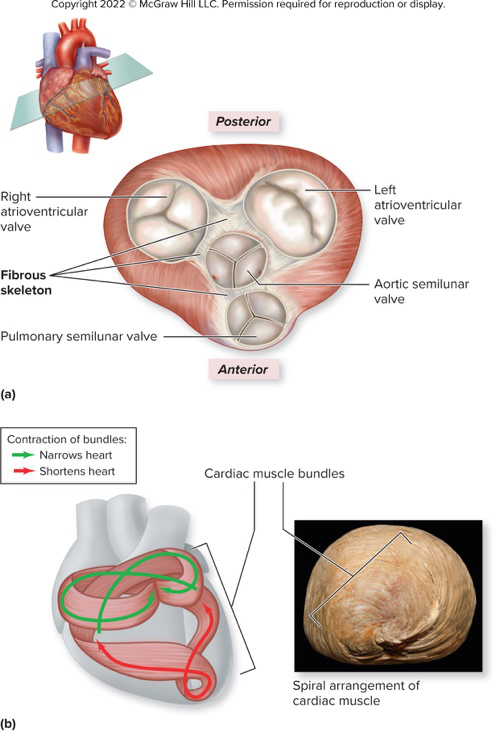
What is the fibrous skeleton of the heart made of and one primary structural role?
How does the fibrous skeleton contribute to valve function?
What electrical role does the fibrous skeleton perform?
Describe the arrangement of cardiac muscle fibers and one consequence for contraction.
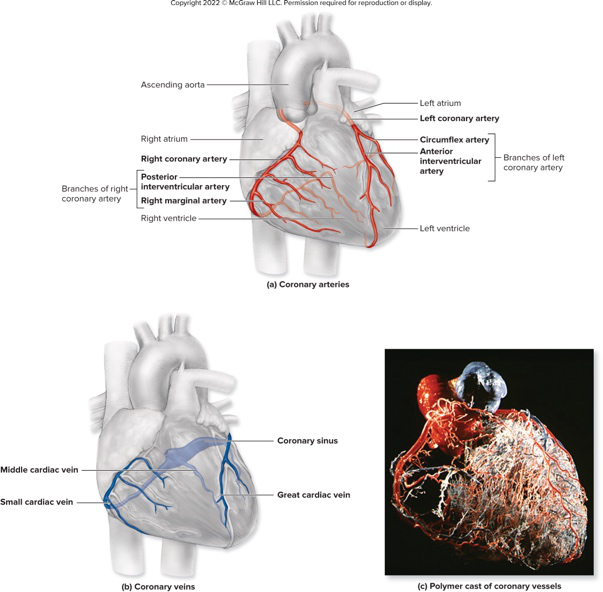
What is the main function of coronary arteries?
Where do coronary veins drain blood and toward which chamber?
Name two branches of the right coronary artery and one area each supplies.
Name two branches of the left coronary artery and what they supply.
What does it mean that coronary arteries are 'functional end arteries'?
How does cardiac contraction affect coronary blood flow during the cardiac cycle?
Which cardiac veins and structure collect venous blood from the heart muscle?
What structures are anchored by the fibrous rings shown in the heart valve diagram?
What is coronary heart disease?
What is a coronary spasm?
What conditions can coronary atherosclerosis or coronary spasm lead to?
How is angina pectoris typically experienced?
What defines a myocardial infarction?
List common symptoms of a myocardial infarction.
Describe the basic microscopic structure of cardiac muscle cells.
What specialized membrane and invaginations are present in cardiac muscle cells?
How are cardiac cells connected and how does this affect heart function?
What are key metabolic features of cardiac muscle?
Why is cardiac muscle especially susceptible to ischemia?
Which image shows cross and longitudinal views of cardiac muscle cells and intercellular junctions? (illustration on answer side)
What is the heart's conduction system?
What is special about the cardiac muscle cells in the conduction system?
Which structure initiates the heartbeat and where is it located?
Where is the atrioventricular (AV) node located?
Describe the path and division of the atrioventricular (AV) bundle.
Where do Purkinje fibers extend and what do they do?
What are the components and primary inputs of the cardiac center in the medulla oblongata?
How does the autonomic nervous system influence cardiac activity?
What are the specific effects and pathways of parasympathetic innervation of the heart?
What are the specific effects and pathways of sympathetic innervation of the heart?
What two events are involved in heart contraction?
In what order do the conduction and contraction events occur in the heart?
Illustration: where are major conduction components located? (See diagram on answer side)
What role do SA nodal cells play in heart function?
What is the resting membrane potential (RMP) of SA nodal cells and is it stable?
What is the pacemaker potential of SA nodal cells?
Name the common membrane proteins present in SA nodal cells.
Which specific voltage-gated channels are found in SA nodal cells?
During the 'reaching threshold' phase in SA node AP, which channels open and how does membrane potential change?
What occurs during the depolarization phase of an SA nodal cell action potential?
What ionic events cause repolarization in SA nodal cells?
How often does an SA node action potential start at rest according to the text, and what heart rate does this translate to?
What factors modify the intrinsic firing rate of the SA node?
Refer to an illustration of SA nodal cell channels (image on answer). Which image shows the SA nodal cell at rest?
Refer to an illustration of nodal action potential phases (image on answer). What phases are illustrated?
What is the first step in spread of the cardiac action potential after initiation at the SA node?
Why is the action potential delayed at the AV node?
Give the sequence of structures the AP travels through from AV node to ventricular myocardium.
What specialized features of Purkinje fibers speed ventricular excitation?
Where does ventricular stimulation begin and why is this important for ejection?
What role do papillary muscles play during ventricular contraction?
What is an ectopic pacemaker and which structure commonly becomes the default pacemaker if the SA node fails?
What are the inherent spontaneous rates of the AV node and of cardiac muscle if they act as pacemakers?
What is the resting membrane potential of cardiac muscle cells and which major membrane channels do they contain?
Show a diagram illustrating the cardiac conduction pathway (SA node to ventricles).
Show an image of cardiac muscle cells at rest with their membrane channels.
What ion movement causes the rapid depolarization phase of a cardiac muscle action potential?
Which channels open during the plateau phase of a cardiac muscle action potential and what ions move?
How does the plateau phase affect the membrane potential of cardiac muscle cells?
What initiates contraction in cardiac muscle cells after Ca2+ entry?
List the main steps of crossbridge cycling in cardiac muscle.
How is relaxation achieved in cardiac muscle cells after contraction?
Why can cardiac muscle not exhibit tetany?
What is the approximate duration of the refractory period produced by the cardiac plateau phase?
How do voltage-gated Ca2+ channels and K+ channels behave during repolarization of cardiac muscle?
Illustrate the phases of a cardiac action potential and muscle tension relationship (useful diagram).
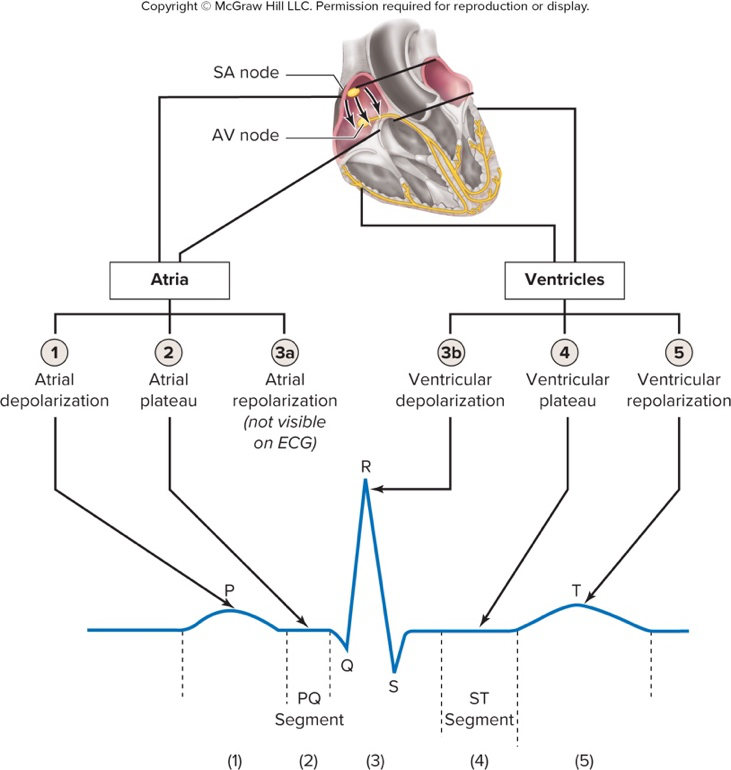
What is an electrocardiogram (ECG/EKG)?
What does the P wave on an ECG represent?
What cardiac event does the QRS complex reflect?
What does the T wave on an ECG represent?
Why is atrial repolarization not visible on a typical ECG?
What does the P-Q (PQ) segment correspond to in atrial activity?
What does the S-T (ST) segment correspond to in ventricular activity?
Define the P-R (P-R) interval on an ECG.
Define the Q-T (Q-T) interval on an ECG.
Which ECG intervals or segments are associated with plateaus of cardiac action potentials?
How do major electrical events of the heart map to ECG waves and segments?
What clinical risk can be associated with changes in the Q-T interval?
What is a cardiac arrhythmia?
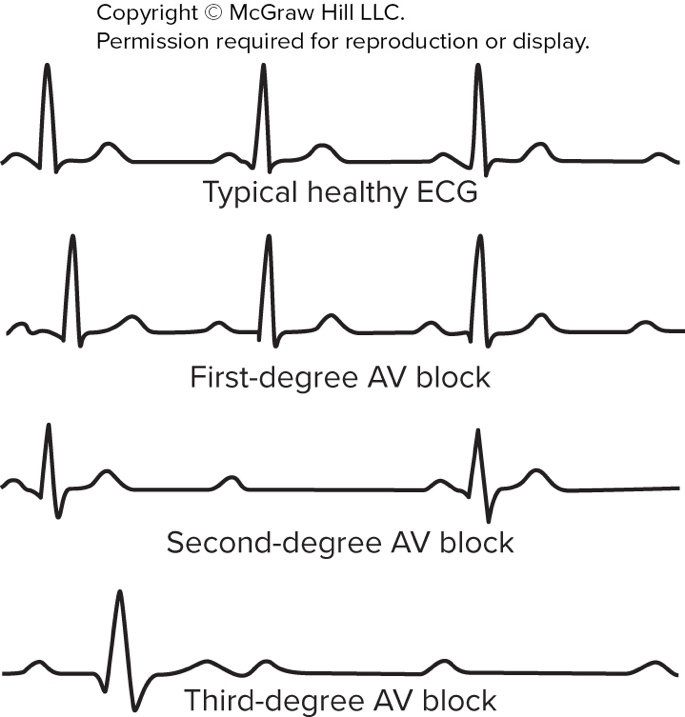
What is a heart block?
What defines a first-degree AV block?
What occurs in a second-degree AV block?
What occurs in a third-degree (complete) AV block?
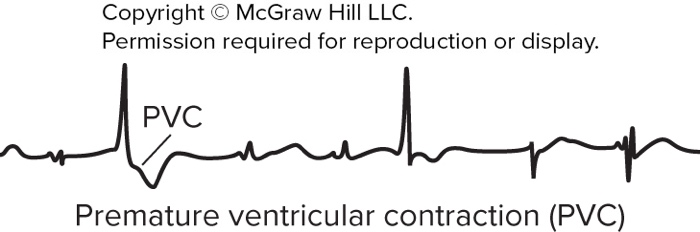
What are premature ventricular contractions (PVCs) and common triggers?
When are premature ventricular contractions considered detrimental?
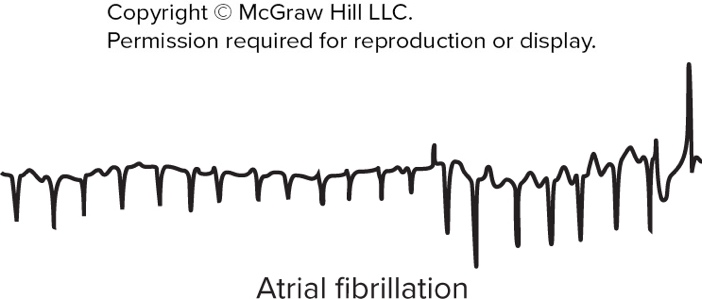
What characterizes atrial fibrillation?
What characterizes ventricular fibrillation and its consequence?
How is ventricular fibrillation treated acutely?
What is the cardiac cycle?
During the cardiac cycle, what drives blood movement?
What is the role of valves during the cardiac cycle?
List the valve changes during ventricular contraction.
What happens to valves during ventricular relaxation?
What are the events at the start of the cardiac cycle regarding chamber states and valve positions?
Provide an image illustrating ECG examples of AV blocks and arrhythmias (as supplementary material).
Provide an image illustrating a premature ventricular contraction (PVC) ECG (as supplementary material).
Provide an image illustrating atrial fibrillation ECG (as supplementary material).
Provide an image illustrating ventricular fibrillation ECG (as supplementary material).
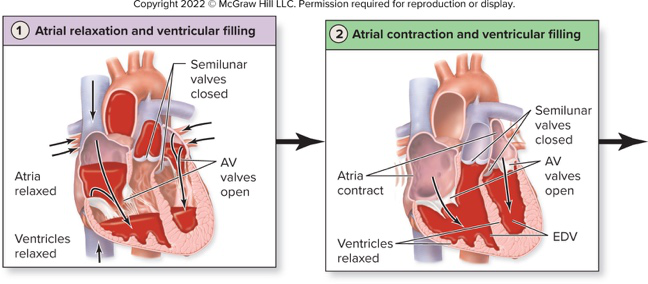
Provide an image illustrating atrial relaxation and ventricular filling stages (as supplementary material).
What initiates atrial excitation in the cardiac conduction sequence?
What happens during atrial contraction regarding ventricular filling?
What initiates ventricular excitation before isovolumic contraction?
What occurs to the AV valves and semilunar (SL) valves during isovolumic contraction?
What triggers semilunar valves to open during ventricular ejection?
Define stroke volume (SV) in the context of the cardiac cycle.
Provide the relationship between end systolic volume (ESV), end diastolic volume (EDV), and stroke volume (SV).
Give the numerical example of ESV, EDV, and SV provided in the text.
What describes isovolumic relaxation after ventricular ejection?
What happens during atrial relaxation and ventricular filling at the start of the cycle?
What is meant by ventricular balance between left and right sides of the heart?
Refer to a diagram illustrating cardiac cycle phases and ECG/pressure/volume graphs. What phases are labeled in that diagram?
What is cardiac output (CO)?
Which two variables determine cardiac output?
Why do individuals with smaller hearts typically have higher resting heart rates?
How does the heart of an endurance athlete differ in stroke volume and resting heart rate?
What is cardiac reserve and how is it calculated?
Typical increases in CO during exercise for nonathletes and athletes?
What are chronotropic agents and what cells do they alter?
Name mechanisms by which sympathetic stimulation raises heart rate.
What intracellular signaling cascade is activated by ẞ1-adrenergic receptors on nodal cells?
How does thyroid hormone affect heart rate via nodal cells?
How do caffeine, nicotine, and cocaine each increase heart rate?
Refer to the diagram of an SA nodal cell and modulatory agents. Which URL shows this diagram?
What effect do negative chronotropic agents have on heart rate?
How does parasympathetic activity slow the heart via nodal cells?
What is the mechanism of action of beta-blocker drugs mentioned in the text?
For what clinical purpose are beta-blocker drugs used in the text?
Which receptors send signals to the cardiac center to influence autonomic output?
What does the atrial (Bainbridge) reflex protect the heart from?
Describe the sequence triggered by increased venous return in the atrial reflex.
What three main factors influence stroke volume (SV) as listed in the text?
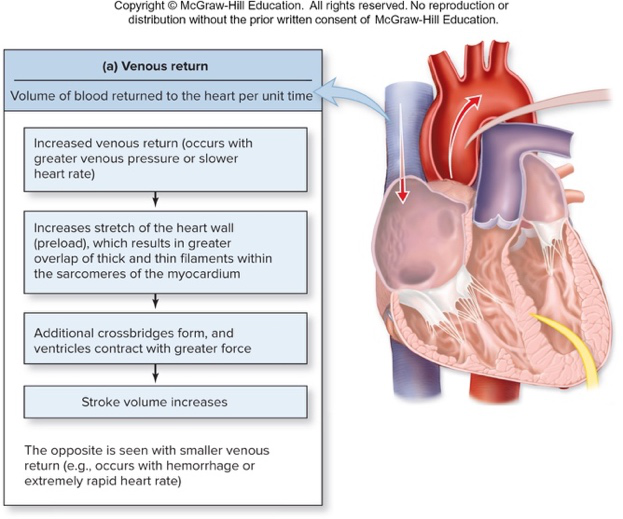
How is venous return related to stroke volume and what ventricular volume does it determine?
State the Frank-Starling law as described in the text.
Name two ways venous return may be increased according to the text.
Give one reason venous pressure increases during exercise described in the text.
List two conditions that decrease venous return as stated in the text.
What is the consequence of decreased venous return on EDV and SV in the text?
How does the Frank-Starling law contribute to balanced ventricular output?
Refer to the venous return diagram for illustration of factors affecting venous return:
What is the primary effect of inotropic agents on the heart?
How do changes in sarcoplasmic Ca2+ affect cardiac contractility?
Name three examples of positive inotropic influences mentioned.
What is a negative inotropic influence listed in the text?
Define afterload in the context of ventricular ejection.
List two causes of increased afterload given in the text.
How does increased afterload affect stroke volume?
What two variables determine cardiac output according to the text?
Name factors that influence stroke volume as listed in the text.
What is bradycardia and what are some abnormal causes mentioned?
What is tachycardia and what causes are given in the text?
Which image illustrates the effects of afterload, venous return, and inotropic agents on EDV, ESV, and SV?
Flashcards in this deck (217)
-
overview anatomy
-
Define 'perfusion' in the context of the cardiovascular system.
Perfusion = delivery of blood per time per gram of tissue (Π mL/min/g)
physiology perfusion -
What are the main functions of the cardiovascular system?
- Deliver O2 and nutrients
- Remove CO2 and wastes
- Provide adequate perfusion
function physiology -
What is the primary difference in direction between arteries and veins?
- Arteries carry blood away from the heart
- Veins carry blood toward the heart
vessels anatomy -
What is the main role of capillaries?
Capillaries are the sites of exchange between blood and air in lungs and between blood and body cells
capillaries exchange -
What does the right side and left side of the heart receive and pump?
- Right side: receives deoxygenated blood and pumps it to lungs
- Left side: receives oxygenated blood and pumps it to the body
circulation heart -
Name the four chambers of the heart and their basic roles.
- Atria (superior): receive blood and send to ventricles
- Ventricles (inferior): pump blood away
heart chambers -
List the great vessels that transport blood to and from the heart and one function for each.
- Superior and inferior vena cava: drain deoxygenated blood into right atrium
- Pulmonary trunk: transports blood from right ventricle
- Pulmonary veins: drain oxygenated blood into left atrium
- Aorta: transports blood from left ventricle
greatvessels anatomy -
What are the two sets of heart valves and their general function?
- Atrioventricular (AV) valves: between atrium and ventricle of each side
- Semilunar valves: at boundary of ventricle and arterial trunk Function: ensure one-way flow of blood through the heart
valves physiology -
Where are the pulmonary and aortic semilunar valves located?
- Pulmonary semilunar valve: between right ventricle and pulmonary trunk
- Aortic semilunar valve: between left ventricle and the aorta
valves anatomy -
Refer to the circulatory diagram: which vessel type is shown exchanging gases in magnified capillaries?
Capillaries are the vessel type shown exchanging gases in the magnified sections
image capillaries -
Refer to the heart anatomy diagram: name one chamber labeled in the diagram.
- Left atrium (Other labeled chambers include right atrium, left ventricle, right ventricle)
image heart -
What is pulmonary circulation?
Pathway that carries deoxygenated blood from the right side of the heart to the lungs where it picks up oxygen and releases carbon dioxide, then returns blood to the left side of the heart.
pulmonary circulation -
What is systemic circulation?
Pathway that carries oxygenated blood from the left side of the heart to systemic cells (e.g., skin, muscles) for exchange of gases, nutrients, and wastes, then returns blood to the right side of the heart.
circulation systemic -
What is the basic overall pattern of blood flow through the heart and body?
right heart → lungs → left heart → systemic tissues → right heart
circulation flow -
What is congestive heart failure (CHF)?
A condition with impaired ability of the heart to pump blood; edema (swelling) is a characteristic symptom.
clinical chf -
What can cause systemic edema in heart failure?
Impaired ventricle function leading to more blood remaining in systemic circulation and additional fluid entering the interstitial space.
chf edema -
What causes pulmonary edema in heart failure and what is its effect?
Impaired ventricle function causing more blood to remain in pulmonary circulation, resulting in swelling and fluid accumulation in the lungs with breathing difficulties and impaired gas exchange.
chf pulmonary -
Where is the heart located and how is it oriented in the thoracic cavity?
- The heart is enclosed in the pericardium within the thoracic cavity
- It sits posterior to the sternum, left of midline, between the lungs in the mediastinum
- It is slightly rotated with the right side more anterior than the left
- The apex projects anteroinferiorly toward the left side
anatomy location -
Show an illustration of the heart's position in the thoracic cavity.
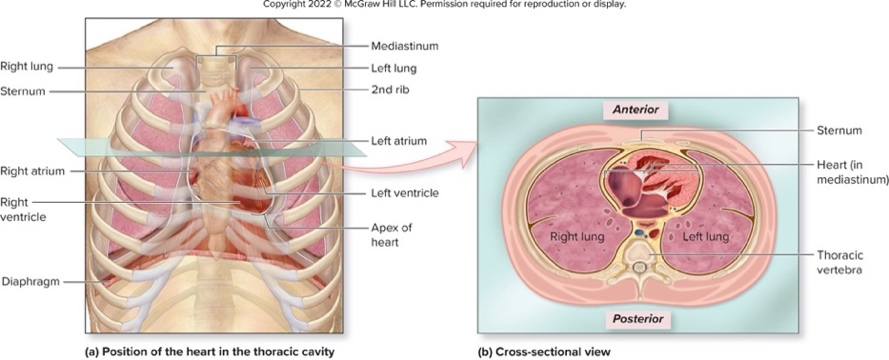 - Illustration of heart positioned between lungs, posterior to sternum, with labeled chambersanatomy image
- Illustration of heart positioned between lungs, posterior to sternum, with labeled chambersanatomy image -
cardiology pericardium
-
pericarditis causes
-
How does pericarditis lead to fluid accumulation?
Inflammation increases capillary permeability, causing fluid to accumulate in the pericardial cavity.
pathophysiology pericarditis -
What is the danger when the pericardial cavity fills with fluid?
The pericardial space becomes a real space that may restrict heart movement and prevent chambers from filling, causing cardiac tamponade.
pericarditis tamponade -
What is a friction rub in pericarditis?
A crackling sound heard with a stethoscope when the inflamed pericardial layers rub against each other.
pericarditis signs -
anatomy anterior
-
anatomy posterior
-
What do the coronary sulcus and interventricular sulci separate?
- Coronary sulcus: separates atria from ventricles
- Interventricular sulci: separate left from right ventricles
anatomy sulci -
How do ventricular wall thicknesses compare and why is the left ventricle thicker?
Ventricles have thicker walls than atria; the left ventricle is thicker than the right because it must generate high pressure to force blood through systemic circulation.
anatomy ventricles -
Which structures do the grooves on the heart surface contain?
The grooves (sulci) contain the coronary vessels that supply blood to the heart wall.
 anatomy coronary
anatomy coronary -
anatomy heart
-
What tissue types compose the epicardium (visceral pericardium)?
Simple squamous epithelium and areolar connective tissue
histology epicardium -
Which heart wall layer is the thickest and what is it made of?
The myocardium is the thickest layer and is made of cardiac muscle tissue that contracts to pump blood
anatomy myocardium -
What tissues form the endocardium and what is its continuity?
Simple squamous epithelium and areolar connective tissue; it is continuous with the lining of blood vessels
histology endocardium -
anatomy septa
-
anatomy septa
-
What are pectinate muscles and where are they found in the heart?
Ridges on the anterior wall and within the auricle of the right atrium; also present in the left atrium auricle
anatomy atria -
What is the fossa ovalis and what fetal structure did it occupy?
An oval depression on the interatrial septum that occupies the location of the fetal foramen ovale, which shunted blood from right to left atrium
anatomy fetal -
Name three structures that enter the right atrium.
- Coronary sinus
- Superior vena cava
- Inferior vena cava
anatomy atria -
What are trabeculae carneae and where are they located?
Irregular muscular ridges on the internal surface of the ventricle wall
anatomy ventricles -
What are papillary muscles and their function in ventricles?
Cone-shaped projections from internal ventricle wall that anchor chordae tendineae
anatomy ventricles -
What are chordae tendineae composed of and what do they attach to?
Thin strands of collagen fibers attaching to valve leaflets
anatomy valves -
Through which valve does blood exit the right ventricle to the pulmonary trunk?
Pulmonary semilunar valve
anatomy valves -
anatomy valves
-
How many papillary muscles typically anchor chordae tendineae in the right ventricle and in the left ventricle?
Right ventricle typically has 3 papillary muscles; left ventricle has 2 papillary muscles
anatomy ventricles -
Which atrium receives pulmonary veins and exits to the left ventricle through which valve?
Left atrium receives pulmonary veins and exits to the left ventricle through the left AV valve
anatomy atria -
anatomy diagram
-
anatomy diagram
-
valves anatomy
-
histology valves
-
Name the right atrioventricular valve and its distinguishing feature.
- Right AV valve (tricuspid)
- Has three flaps
valves atrioventricular -
Name the left atrioventricular valve and its distinguishing feature.
- Left AV valve (mitral/bicuspid)
- Has two flaps
valves atrioventricular -
What prevents atrioventricular valves from inverting into the atria during ventricular contraction?
- Papillary muscles and tendinous cords
valves mechanics -
How do semilunar valves close when ventricles relax?
When arterial pressure exceeds ventricular pressure, blood starts to slide backward, which catches the cusps and closes the valves.
valves semilunar -
valves pulmonary
-
valves aortic
-
Which heart sounds correspond to closing of AV and semilunar valves?
- S1 = closing of AV valves ("lubb")
- S2 = closing of semilunar valves ("dupp")
sounds clinical -
What is a heart murmur and its two main types?
- Heart murmur: abnormal sound from turbulent blood flow
- Types:
- Valvular insufficiency
- Valvular stenosis
murmur clinical -
What causes valvular insufficiency and its consequence?
Cusps do not close tightly, causing blood regurgitation back through the valve and possible heart enlargement.
murmur insufficiency -
What is valvular stenosis and its effect on cardiac output?
Valve cusps are scarred and cannot open completely, which resists blood flow and reduces chamber output.
murmur stenosis -
What is cardiomegaly and a common cause?
- Cardiomegaly: enlargement of the heart
- Common cause: high blood pressure or coronary heart disease
cardiomegaly clinical -
How does cardiac muscle enlargement affect contraction force in cardiomegaly?
Enlarged cardiac muscle cells result in less overlap of myofilaments and less forceful contraction.
cardiomegaly physiology -
What is the fibrous skeleton of the heart made of and one primary structural role?
- Dense irregular connective tissue
- Provides structural support at the boundary of atria and ventricles
anatomy heart -
valves heart
-
What electrical role does the fibrous skeleton perform?
- Acts as an electrical insulator preventing ventricles and atria from contracting at the same time
conduction heart -
Describe the arrangement of cardiac muscle fibers and one consequence for contraction.
- Spiral bundles of muscle attached to fibrous skeleton
- Ventricular contraction resembles wringing a mop and begins at the apex
muscle contraction -
coronary blood
-
Where do coronary veins drain blood and toward which chamber?
- Drain deoxygenated blood away from heart wall toward the right atrium
coronary veins -
Name two branches of the right coronary artery and one area each supplies.
- Right marginal artery: supplies right heart border
- Posterior interventricular artery: supplies posterior left and right ventricle
coronary right -
Name two branches of the left coronary artery and what they supply.
- Circumflex artery: supplies left atrium and ventricle
- Anterior interventricular artery: supplies anterior ventricles and most of interventricular septum
coronary left -
What does it mean that coronary arteries are 'functional end arteries'?
- Although structural anastomoses exist, blockage of a coronary artery leads to insufficient flow to the heart wall because anastomoses are too small to function as effective alternates
coronary pathology -
How does cardiac contraction affect coronary blood flow during the cardiac cycle?
- Coronary flow is intermittent: vessels are patent when the heart is relaxed and compressed (interrupting flow) when the heart contracts
hemodynamics coronary -
Which cardiac veins and structure collect venous blood from the heart muscle?
- Great cardiac vein (anterior interventricular sulcus)
- Middle cardiac vein (inferior interventricular sulcus)
- Small cardiac vein (next to right marginal artery)
- Coronary sinus receives these veins and drains into the right atrium
 veins coronary
veins coronary -
What structures are anchored by the fibrous rings shown in the heart valve diagram?
- Right atrioventricular valve
- Left atrioventricular valve
- Aortic semilunar valve
- Pulmonary semilunar valve
 valves fibrous
valves fibrous -
What is coronary heart disease?
- Buildup of plaque in coronary arteries (atherosclerosis) that reduces blood flow to the heart muscle
cardiology pathology -
cardiology pathology
-
What conditions can coronary atherosclerosis or coronary spasm lead to?
- Angina pectoris
- Myocardial infarction
cardiology complications -
How is angina pectoris typically experienced?
- Heart pain during strenuous activity, usually felt on the left side of chest, left arm, or jaw; treatments induce vascular dilation
cardiology symptoms -
What defines a myocardial infarction?
- Sudden and complete occlusion of a coronary artery causing myocardium oxygen deprivation and possible tissue death
cardiology myocardial infarction -
List common symptoms of a myocardial infarction.
- Excruciating chest pain radiating down left arm
- Weakness
- Shortness of breath
- Nausea
- Anxiety
- Sweating
cardiology symptoms -
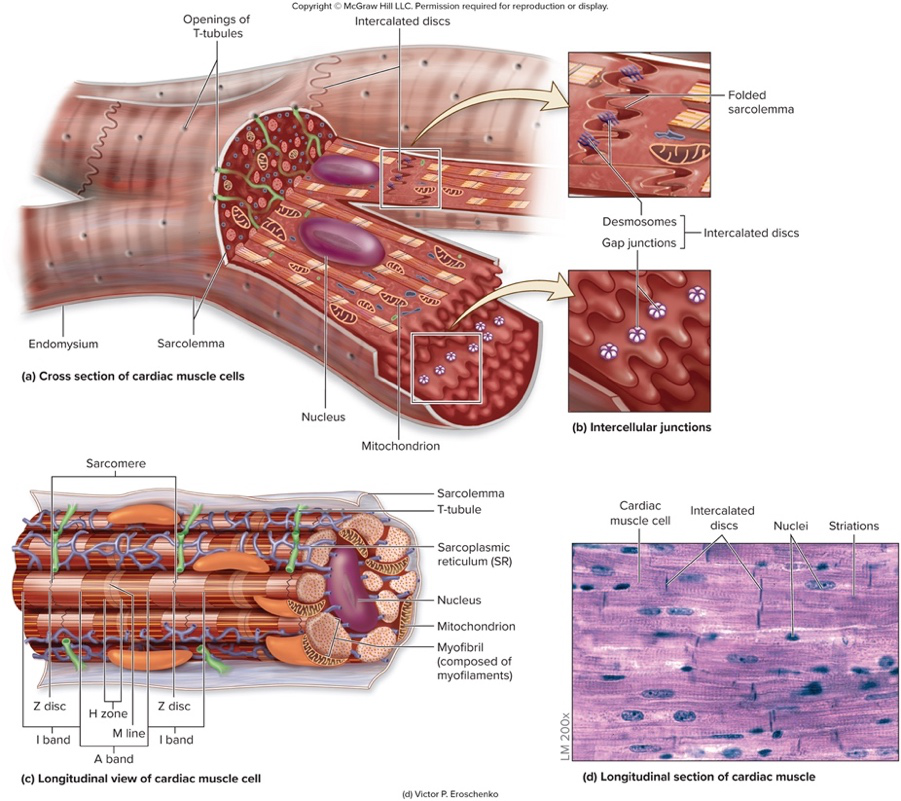
Describe the basic microscopic structure of cardiac muscle cells.
- Short, branched cells with one or two central nuclei, arranged in striated sarcomeres and supported by endomysium
histology cardiac -
What specialized membrane and invaginations are present in cardiac muscle cells?
- Sarcolemma (plasma membrane) that invaginates to form T-tubules extending into the sarcoplasmic reticulum
histology membrane -
How are cardiac cells connected and how does this affect heart function?
- Cells connected by intercalated discs containing desmosomes and gap junctions; desmosomes provide mechanical linkage and gap junctions allow action potentials to spread, creating a functional syncytium
histology physiology -
What are key metabolic features of cardiac muscle?
- High energy demand, extensive blood supply, numerous mitochondria, myoglobin and creatine kinase present; able to use fatty acids, glucose, lactic acid, amino acids, and ketone bodies
metabolism cardiac -
Why is cardiac muscle especially susceptible to ischemia?
- Relies mostly on aerobic metabolism, so interference with blood flow (low oxygen) can cause cell death
physiology pathology -
Which image shows cross and longitudinal views of cardiac muscle cells and intercellular junctions? (illustration on answer side)
- Diagrams illustrating cross and longitudinal sections of cardiac muscle cells, highlighting endomysium, sarcolemma, T-tubules, intercalated discs, desmosomes, gap junctions, sarcomere structure
 histology image
histology image -
What is the heart's conduction system?
The conduction system initiates and conducts electrical events to ensure proper timing of contractions.
conduction cardiology -
What is special about the cardiac muscle cells in the conduction system?
They are specialized cardiac muscle cells that have action potentials but do not contract.
cells conduction -
Which structure initiates the heartbeat and where is it located?
- Sinoatrial (SA) node
- Located high in the posterior wall of the right atrium
sa anatomy -
Where is the atrioventricular (AV) node located?
The AV node is located in the floor of the right atrium near the right AV valve.
av anatomy -
Describe the path and division of the atrioventricular (AV) bundle.
The AV bundle extends from the AV node through the interventricular septum and divides into left and right bundles.
conduction bundle -
Where do Purkinje fibers extend and what do they do?
Purkinje fibers extend from the left and right bundles at the heart's apex and course through the walls of the ventricles.
purkinje ventricles -
What are the components and primary inputs of the cardiac center in the medulla oblongata?
It contains cardioacceleratory and cardioinhibitory centers and receives signals from baroreceptors and chemoreceptors in the cardiovascular system.
medulla regulation -
How does the autonomic nervous system influence cardiac activity?
It modifies (does not initiate) cardiac activity via sympathetic and parasympathetic pathways, influencing rate and force of contractions.
autonomic regulation -
What are the specific effects and pathways of parasympathetic innervation of the heart?
Parasympathetic innervation decreases heart rate, starts at the medulla's cardioinhibitory center, is relayed via vagus nerves; the right vagus innervates the SA node and the left vagus innervates the AV node.
parasympathetic vagus -
What are the specific effects and pathways of sympathetic innervation of the heart?
Sympathetic innervation increases heart rate and force of contraction, starts at the medulla's cardioacceleratory center, relayed via neurons from TC-TS segments of the spinal cord, and extends to SA node, AV node, myocardium, and coronary arteries.
sympathetic innervation -
What two events are involved in heart contraction?
1) The conduction system initiates and propagates an action potential 2) Cardiac muscle cells propagate action potentials and contract
contraction physiology -
In what order do the conduction and contraction events occur in the heart?
This process happens first in the atria and then the ventricles.
sequence cardiaccycle -
Illustration: where are major conduction components located? (See diagram on answer side)
Diagram showing SA node, AV node, AV bundle, left/right bundles, and Purkinje fibers.
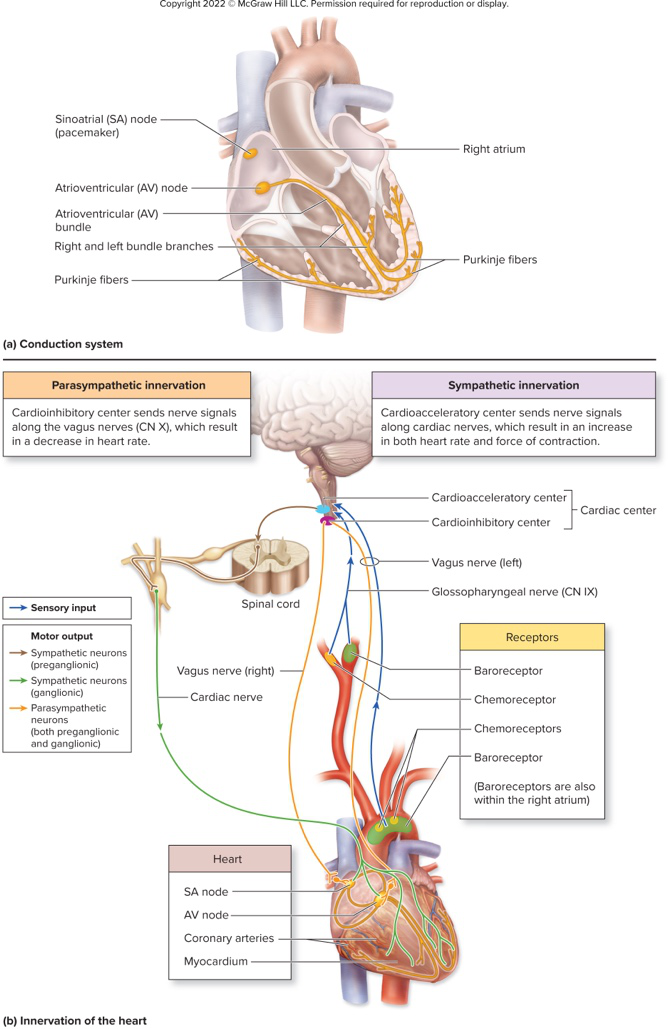 diagram visual
diagram visual -
What role do SA nodal cells play in heart function?
- SA nodal cells initiate the heartbeat
- They spontaneously depolarize and generate action potentials
cardiac conduction -
What is the resting membrane potential (RMP) of SA nodal cells and is it stable?
- RMP ≈ -60 mV
- This RMP is not stable (they do not have a stable RMP)
physiology membrane -
What is the pacemaker potential of SA nodal cells?
- The pacemaker potential is the ability to reach threshold without external stimulation
pacemaker cardiac -
membrane proteins
-
Which specific voltage-gated channels are found in SA nodal cells?
- Slow voltage-gated Na+ channels
- Fast voltage-gated Ca2+ channels
- Voltage-gated K+ channels
ionchannels electrophysiology -
During the 'reaching threshold' phase in SA node AP, which channels open and how does membrane potential change?
- Slow voltage-gated Na+ channels open; Na+ flows in
- Membrane potential changes from -60 mV to -40 mV (threshold)
actionpotential threshold -
What occurs during the depolarization phase of an SA nodal cell action potential?
- Fast voltage-gated Ca2+ channels open; Ca2+ flows in
- Membrane potential goes from -40 mV to just above 0 mV
depolarization calcium -
What ionic events cause repolarization in SA nodal cells?
- Calcium channels close
- Voltage-gated K+ channels open; K+ flows out
- Membrane potential returns to RMP ≈ -60 mV
repolarization potassium -
How often does an SA node action potential start at rest according to the text, and what heart rate does this translate to?
- One AP starts about 0.8 sec after the last
- This translates to 15 heart beats per minute
rate rhythm -
What factors modify the intrinsic firing rate of the SA node?
- Intrinsic firing can be faster (≈100/min in tissue culture)
- Vagal tone (parasympathetic activity via the vagus nerve) slows resting heart rate
autonomic modulation -
Refer to an illustration of SA nodal cell channels (image on answer). Which image shows the SA nodal cell at rest?
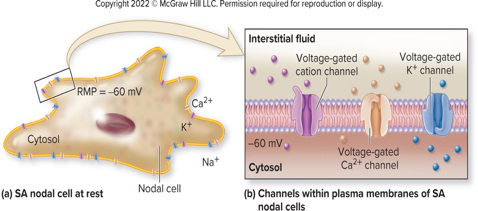 - Diagram shows nodal cell, cytosol, and voltage-gated channels as labeledvisual diagram
- Diagram shows nodal cell, cytosol, and voltage-gated channels as labeledvisual diagram -
Refer to an illustration of nodal action potential phases (image on answer). What phases are illustrated?
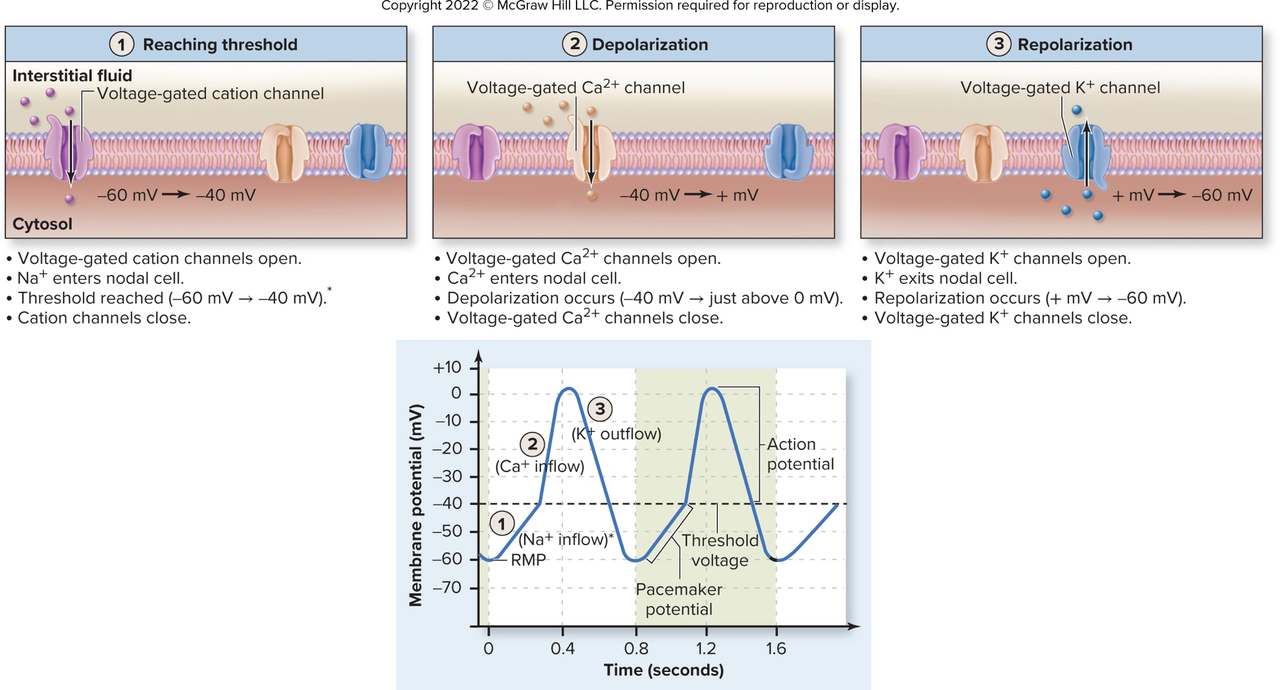 - The image shows: Reaching threshold, Depolarization, Repolarizationvisual phases
- The image shows: Reaching threshold, Depolarization, Repolarizationvisual phases -
What is the first step in spread of the cardiac action potential after initiation at the SA node?
AP is distributed through the atria and reaches the AV node; excitation travels via gap junctions and both atria contract together.
conduction atria -
Why is the action potential delayed at the AV node?
AV nodal cells are slow due to small diameter and few gap junctions; the fibrous skeleton insulates making the AV node the only path and a bottleneck.
avnode conduction -
Give the sequence of structures the AP travels through from AV node to ventricular myocardium.
- AV node
- AV bundle
- Bundle branches
- Purkinje fibers
pathway conduction -
What specialized features of Purkinje fibers speed ventricular excitation?
Purkinje fibers are larger in diameter and conduct action potentials extremely rapidly to ensure near-simultaneous ventricular contraction.
purkinje ventricles -
Where does ventricular stimulation begin and why is this important for ejection?
Stimulation begins at the heart apex to ensure blood is efficiently ejected toward the arterial trunks.
ventricles ejection -
What role do papillary muscles play during ventricular contraction?
Papillary muscles contract to pull on chordae tendinae of AV cusps, starting before ventricular pressure rises to restrain cusps.
papillary valves -
What is an ectopic pacemaker and which structure commonly becomes the default pacemaker if the SA node fails?
An ectopic pacemaker is a pacemaker other than the SA node; the AV node becomes the default pacemaker if the SA node is impaired.
ectopic pacemaker -
What are the inherent spontaneous rates of the AV node and of cardiac muscle if they act as pacemakers?
AV node: 40 to 50 beats/min; cardiac muscle: 20 to 40 beats/min.
rates pacemaker -
What is the resting membrane potential of cardiac muscle cells and which major membrane channels do they contain?
Resting membrane potential is -90 mV; cells contain Na+/K+ pumps, Ca2+ pumps, leakage channels for Na+ and K+, and voltage-gated fast Na+, slow Ca2+, and K+ channels.
cardiac membrane -
Show a diagram illustrating the cardiac conduction pathway (SA node to ventricles).
Diagram:
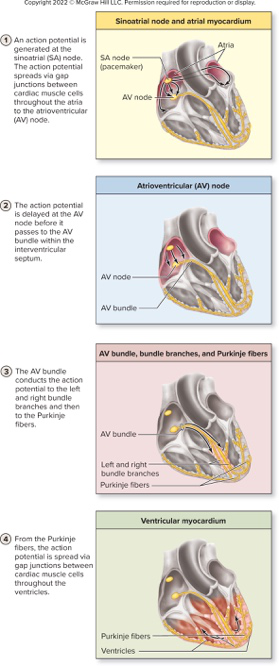 The diagram illustrates the SA node, AV node, AV bundle, bundle branches, Purkinje fibers, and ventricular myocardium.diagram conduction
The diagram illustrates the SA node, AV node, AV bundle, bundle branches, Purkinje fibers, and ventricular myocardium.diagram conduction -
Show an image of cardiac muscle cells at rest with their membrane channels.
Image:
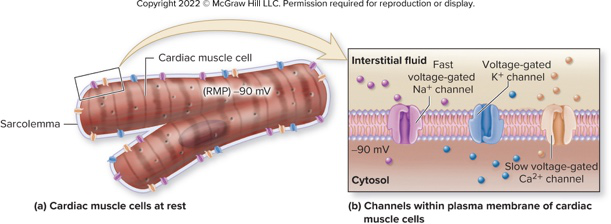 The image depicts the sarcolemma and fast Na+, slow Ca2+, and K+ voltage-gated channels.diagram membrane
The image depicts the sarcolemma and fast Na+, slow Ca2+, and K+ voltage-gated channels.diagram membrane -
What ion movement causes the rapid depolarization phase of a cardiac muscle action potential?
- Fast voltage-gated Na+ channels open; Na+ enters the cell, changing membrane potential from -90 mV to +30 mV
electrophysiology depolarization -
Which channels open during the plateau phase of a cardiac muscle action potential and what ions move?
- Slow voltage-gated Ca2+ channels open (Ca2+ enters) and voltage-gated K+ channels open (K+ leaves)
plateau ions -
How does the plateau phase affect the membrane potential of cardiac muscle cells?
- The membrane remains depolarized during the plateau because Ca2+ entry offsets K+ efflux
plateau membrane -
What initiates contraction in cardiac muscle cells after Ca2+ entry?
- Ca2+ entering sarcoplasm (from interstitial fluid and SR) binds troponin and initiates crossbridge cycling
contraction calcium -
List the main steps of crossbridge cycling in cardiac muscle.
- **Crossbridge formation
- Power stroke
- Release of myosin head
- Reset of myosin head**
crossbridge mechanics -
How is relaxation achieved in cardiac muscle cells after contraction?
- Ca2+ levels decrease as channels close and pumps move Ca2+ into the SR and out of the cell, causing relaxation
relaxation calcium -
Why can cardiac muscle not exhibit tetany?
- Cardiac cells have a long refractory period (about 250 ms) so a new impulse cannot fire until contraction and relaxation finish
refractory tetany -
What is the approximate duration of the refractory period produced by the cardiac plateau phase?
- About 250 ms
duration refractory -
How do voltage-gated Ca2+ channels and K+ channels behave during repolarization of cardiac muscle?
- Voltage-gated Ca2+ channels close while K+ channels remain open, returning membrane potential to -90 mV
repolarization channels -
Illustrate the phases of a cardiac action potential and muscle tension relationship (useful diagram).
- Phases: Depolarization → Plateau → Repolarization. Diagram illustrating action potential and tension:
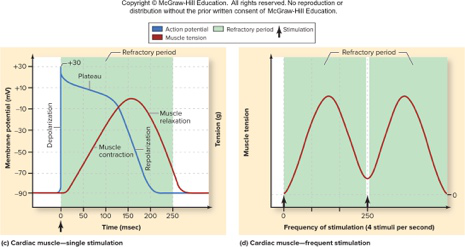
diagram visual - Phases: Depolarization → Plateau → Repolarization. Diagram illustrating action potential and tension:
-
What is an electrocardiogram (ECG/EKG)?
A recording made by skin electrodes that detects electrical signals of cardiac muscle cells.
cardiology ecg -
What does the P wave on an ECG represent?
Electrical changes of atrial depolarization originating in the SA node.
ecg atria -
What cardiac event does the QRS complex reflect?
Electrical changes associated with ventricular depolarization.
ecg ventricles -
What does the T wave on an ECG represent?
Electrical change associated with ventricular repolarization.
ecg repolarization -
Why is atrial repolarization not visible on a typical ECG?
Atrial repolarization is masked by the QRS complex.
ecg atria -
What does the P-Q (PQ) segment correspond to in atrial activity?
The atrial plateau phase during which atria are contracting.
ecg segments -
What does the S-T (ST) segment correspond to in ventricular activity?
The ventricular plateau phase during which ventricles are contracting.
ecg segments -
Define the P-R (P-R) interval on an ECG.
Time from the beginning of the P wave to the beginning of the QRS deflection; time to transmit the action potential through the conduction system.
ecg intervals -
Define the Q-T (Q-T) interval on an ECG.
Time from the beginning of the QRS to the end of the T wave; reflects the time of ventricular action potentials and varies with heart rate.
ecg intervals -
Which ECG intervals or segments are associated with plateaus of cardiac action potentials?
- P-Q segment: atrial plateau
- S-T segment: ventricular plateau
ecg actionpotentials -
How do major electrical events of the heart map to ECG waves and segments?
Atrial depolarization = P wave; atrial plateau = PQ segment; ventricular depolarization = QRS complex; ventricular plateau = ST segment; ventricular repolarization = T wave.
 ecg mapping
ecg mapping -
What clinical risk can be associated with changes in the Q-T interval?
Changes may result in tachyarrhythmia, a rapid, irregular heart rate.
ecg arrhythmia -
arrhythmia cardiology
-
conduction heart
-
What defines a first-degree AV block?
PR prolongation reflecting slow conduction between atria and ventricles.
avblock ecg -
What occurs in a second-degree AV block?
Some atrial action potentials fail to reach the ventricles.
avblock conduction -
What occurs in a third-degree (complete) AV block?
All atrial action potentials fail to reach the ventricles.
avblock conduction -
What are premature ventricular contractions (PVCs) and common triggers?
Premature ventricular contractions are abnormal action potentials in the AV node or ventricles and may result from stress, stimulants, or sleep deprivation.
pvc arrhythmia -
When are premature ventricular contractions considered detrimental?
They are not detrimental unless they occur in large numbers.
pvc clinical -
atrial fibrillation
-
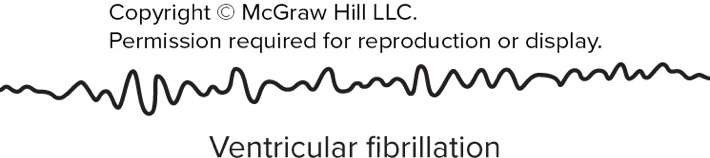
What characterizes ventricular fibrillation and its consequence?
Chaotic electrical activity in ventricles causing uncoordinated contraction, pump failure, and leading to death of heart cells.
ventricular fibrillation -
How is ventricular fibrillation treated acutely?
With a paddle electrode defibrillator or an automated external defibrillator (AED).
treatment emergency -
What is the cardiac cycle?
All events in the heart from the start of one heartbeat to the start of the next.
cardiaccycle physiology -
During the cardiac cycle, what drives blood movement?
Blood moves down its pressure gradient (from high to low); ventricular activity is the most important driving force.
hemodynamics cardiaccycle -
What is the role of valves during the cardiac cycle?
Valves ensure forward flow by closing to prevent backflow.
valves cardiaccycle -
List the valve changes during ventricular contraction.
- AV valves pushed closed
- Semilunar (SL) valves pushed open
- Blood ejected into the artery
ventricle contraction -
What happens to valves during ventricular relaxation?
- Semilunar (SL) valves close
- AV valves open
- No pressure from below keeps AV valves open
ventricle relaxation -
What are the events at the start of the cardiac cycle regarding chamber states and valve positions?
- Four chambers at rest
- Blood returning to both atria
- Passive filling of ventricles
- AV valves open
- Semilunar valves closed
cardiaccycle filling -
Provide an image illustrating ECG examples of AV blocks and arrhythmias (as supplementary material).
See ECG examples:
 ecg visual
ecg visual -
Provide an image illustrating a premature ventricular contraction (PVC) ECG (as supplementary material).
See PVC ECG:
 pvc ecg
pvc ecg -
Provide an image illustrating atrial fibrillation ECG (as supplementary material).
See atrial fibrillation ECG:
 atrial ecg
atrial ecg -
Provide an image illustrating ventricular fibrillation ECG (as supplementary material).
See ventricular fibrillation ECG:
 ventricular ecg
ventricular ecg -
Provide an image illustrating atrial relaxation and ventricular filling stages (as supplementary material).
See diagrams of atrial relaxation and ventricular filling:
 diagrams filling
diagrams filling -
What initiates atrial excitation in the cardiac conduction sequence?
- SA node starts atrial excitation
conduction sanode -
What happens during atrial contraction regarding ventricular filling?
- Atria contract pushing remaining blood into ventricles; ventricles fill to end-diastolic volume (EDV)
cardiaccycle edv -
What initiates ventricular excitation before isovolumic contraction?
- Purkinje fibers initiate ventricular excitation
conduction purkinje -
What occurs to the AV valves and semilunar (SL) valves during isovolumic contraction?
- AV valves are pushed closed; SL valves remain closed because ventricular pressure is still less than arterial trunk pressure
isovolumic valves -
What triggers semilunar valves to open during ventricular ejection?
- Ventricular pressure rises past arterial pressure, forcing semilunar valves open and blood moves to arterial trunks
ejection valves -
Define stroke volume (SV) in the context of the cardiac cycle.
- Stroke volume (SV) is amount of blood ejected by a ventricle
sv cardiaccycle -
Provide the relationship between end systolic volume (ESV), end diastolic volume (EDV), and stroke volume (SV).
- \(ESV = EDV - SV\)
esv edv sv -
Give the numerical example of ESV, EDV, and SV provided in the text.
- Example: 60 mL = 130 mL - 70 mL
example volumes -
What describes isovolumic relaxation after ventricular ejection?
- Ventricles relax and expand; arterial pressure is greater than ventricular pressure so SL valves close; AV valves remain closed; no blood enters or leaves ('isovolumic')
isovolumic relaxation -
What happens during atrial relaxation and ventricular filling at the start of the cycle?
- All chambers relaxed; atrial blood pressure forces AV valves open and blood flows into ventricles; SL valves remain closed because arterial pressure is greater than ventricular pressure
filling avvalves -
What is meant by ventricular balance between left and right sides of the heart?
- Equal amounts of blood are pumped by left and right sides; left heart pumps farther and must be stronger (thicker), but ejected volumes must be the same or edema can occur
ventricle balance -
Refer to a diagram illustrating cardiac cycle phases and ECG/pressure/volume graphs. What phases are labeled in that diagram?
- Phases labeled: atrial relaxation and ventricular filling; atrial contraction and ventricular filling; isovolumic contraction; ventricular ejection; isovolumic relaxation
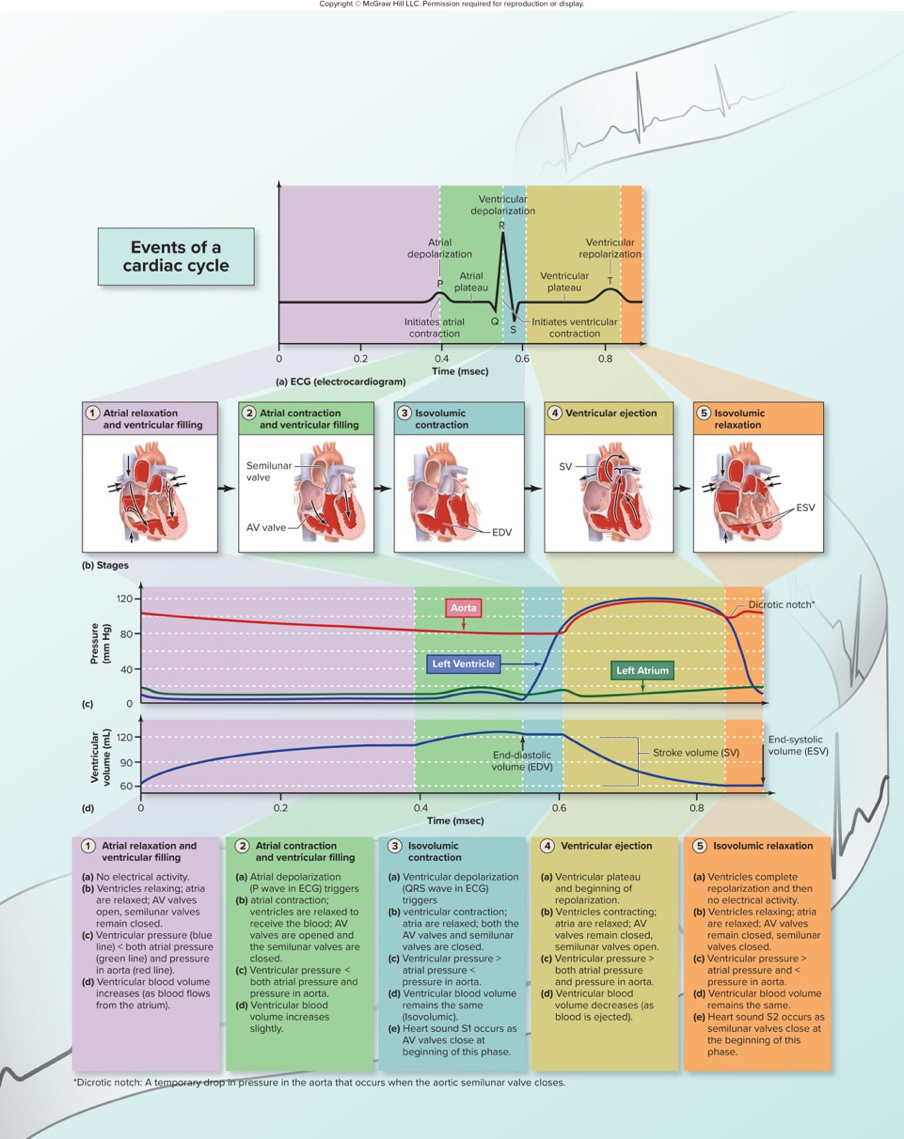 diagram cardiaccycle
diagram cardiaccycle -
What is cardiac output (CO)?
Amount of blood pumped by a single ventricle in one minute; measured in liters per minute.
cardiology definitions -
Which two variables determine cardiac output?
- Heart rate (beats per minute)
- Stroke volume (blood ejected per beat)
cardiology physiology -
Why do individuals with smaller hearts typically have higher resting heart rates?
Smaller hearts have smaller stroke volumes and must compensate with faster heart rates to maintain resting CO.
cardiology physiology -
How does the heart of an endurance athlete differ in stroke volume and resting heart rate?
Endurance athletes have thicker heart walls and stronger hearts, producing larger stroke volume and slower resting heart rate.
cardiology athlete -
What is cardiac reserve and how is it calculated?
Capacity to increase CO above rest level; calculated by subtracting resting CO from CO during exercise.
cardiology exercise -
Typical increases in CO during exercise for nonathletes and athletes?
- Healthy nonathlete: CO can increase four-fold
- Athlete: CO can increase up to seven-fold
cardiology exercise -
What are chronotropic agents and what cells do they alter?
Agents that change heart rate by altering activity of nodal cells (SA and/or AV node).
cardiology pharmacology -
Name mechanisms by which sympathetic stimulation raises heart rate.
Sympathetic stimulation causes NE release from nerves and EPI/NE release from adrenal glands; NE/EPI bind to ẞ1-adrenergic receptors on nodal cells, increasing their firing rate.
cardiology autonomic -
What intracellular signaling cascade is activated by ẞ1-adrenergic receptors on nodal cells?
G-protein → adenylate cyclase → cAMP → protein kinase cascade, which phosphorylates Ca2+ channels to enhance Ca2+ influx.
cardiology signal -
How does thyroid hormone affect heart rate via nodal cells?
Increases number of ẞ1-adrenergic receptors on nodal cells, enhancing responsiveness to NE/EPI.
endocrine cardiology -
How do caffeine, nicotine, and cocaine each increase heart rate?
- Caffeine: inhibits breakdown of cAMP
- Nicotine: increases release of NE
- Cocaine: inhibits reuptake of NE, prolonging its action
pharmacology cardiology -
Refer to the diagram of an SA nodal cell and modulatory agents. Which URL shows this diagram?
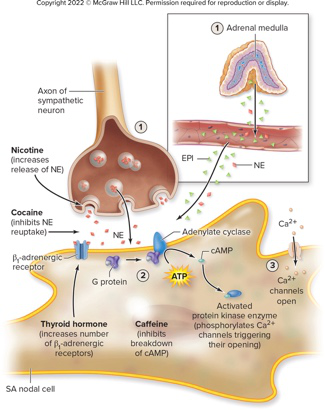 The diagram illustrates SA nodal cell, NE, EPI, sympathetic axon, nicotine, cocaine, thyroid hormone, caffeine, ATP, cAMP, G protein, and Ca2+.image diagram
The diagram illustrates SA nodal cell, NE, EPI, sympathetic axon, nicotine, cocaine, thyroid hormone, caffeine, ATP, cAMP, G protein, and Ca2+.image diagram -
cardiac chronotropy
-
How does parasympathetic activity slow the heart via nodal cells?
- Parasympathetic axons release acetylcholine (ACh) onto nodal cells
- ACh binds muscarinic receptors which are K+ channels
- Channels open, K+ exits, making the cell more negative and slowing threshold reach
parasympathetic conduction -
What is the mechanism of action of beta-blocker drugs mentioned in the text?
- Interfere with EPI and NE binding to beta receptors
pharmacology beta-blockers -
For what clinical purpose are beta-blocker drugs used in the text?
- Used to treat high blood pressure
pharmacology hypertension -
Which receptors send signals to the cardiac center to influence autonomic output?
- Baroreceptors and chemoreceptors
autonomic reflexes -
reflex atria
-
Describe the sequence triggered by increased venous return in the atrial reflex.
- Atrial wall baroreceptors stimulated → increased signals to cardioacceleratory center → increased sympathetic excitation to heart → HR increases
bainbridge physiology -
What three main factors influence stroke volume (SV) as listed in the text?
- Venous return
- Inotropic agents
- Afterload
cardiac stroke-volume -
How is venous return related to stroke volume and what ventricular volume does it determine?
- Venous return is directly related to SV and determines end-diastolic volume (EDV)
venous-return edv -
State the Frank-Starling law as described in the text.
- As EDV varies, greater stretch of heart wall results in more optimal filament overlap so heart contracts more forcefully and SV increases
frank-starling mechanics -
Name two ways venous return may be increased according to the text.
- Increased venous pressure
- Increased time to fill
venous-return exercise -
Give one reason venous pressure increases during exercise described in the text.
- Muscles squeeze veins
exercise venous-return -
List two conditions that decrease venous return as stated in the text.
- Low blood volume (hemorrhage)
- High heart rate
venous-return pathology -
What is the consequence of decreased venous return on EDV and SV in the text?
- Smaller EDV and preload → smaller SV
edv stroke-volume -
How does the Frank-Starling law contribute to balanced ventricular output?
- If one side receives more blood it contracts more forcefully, leading to greater fill and stronger contraction on the other side
frank-starling homeostasis -
Refer to the venous return diagram for illustration of factors affecting venous return:
- See diagram:
- Image illustrates venous return (supplementary)
venous-return image - See diagram:
-
What is the primary effect of inotropic agents on the heart?
They change stroke volume by altering myocardial contractility (force of contraction).
cardiology inotropy -
How do changes in sarcoplasmic Ca2+ affect cardiac contractility?
Ca2+ levels in the sarcoplasm directly relate to the number of cross bridges formed, so increased Ca2+ raises contractility and decreased Ca2+ lowers it.
physiology calcium -
Name three examples of positive inotropic influences mentioned.
- Epinephrine (EPI) and Norepinephrine (NE) via β1 receptors
- Thyroid hormone increasing β1 receptor number
- Drugs such as digitalis
inotropy agents -
What is a negative inotropic influence listed in the text?
Factors that decrease available Ca2+, for example electrolyte imbalances like increased K+ or H+ and Ca2+ channel-blocking drugs.
inotropy pharmacology -
Define afterload in the context of ventricular ejection.
Afterload is the resistance in arteries to ejection of blood by ventricles; the pressure that must be exceeded before blood is ejected.
hemodynamics afterload -
List two causes of increased afterload given in the text.
- Atherosclerosis (plaque in vessel linings)
- Smaller arterial lumen with aging leading to greater resistance
afterload pathology -
How does increased afterload affect stroke volume?
Increased afterload raises arterial resistance and decreases stroke volume.
strokevolume afterload -
What two variables determine cardiac output according to the text?
Cardiac output varies directly with heart rate and stroke volume.
cardiacoutput physiology -
Name factors that influence stroke volume as listed in the text.
- State of the myocardium
- Venous return (alters stretch/EDV)
- Inotropic agents (influence crossbridge formation)
- Afterload (increased afterload decreases SV)
strokevolume determinants -
What is bradycardia and what are some abnormal causes mentioned?
Bradycardia is a persistently low resting heart rate below 60 beats/min; abnormal causes include hypothyroidism, electrolyte imbalance, and congestive heart failure.
rhythm bradycardia -
What is tachycardia and what causes are given in the text?
Tachycardia is a persistently high resting heart rate above 100 beats/min; causes include heart disease, fever, and anxiety.
rhythm tachycardia -
Which image illustrates the effects of afterload, venous return, and inotropic agents on EDV, ESV, and SV?
See diagram:
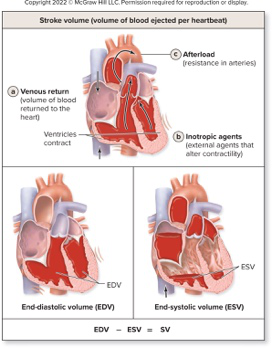 — it shows how afterload, venous return, and inotropic agents affect EDV, ESV, and SV.diagram visual
— it shows how afterload, venous return, and inotropic agents affect EDV, ESV, and SV.diagram visual
Cardiovascular system — quick overview
- Components: heart + blood vessels; moves blood to deliver O2/nutrients and remove CO2/wastes.
- Perfusion: blood delivered per time per gram of tissue (mL/min/g); requires continuous pumping and patent vessels.
Pulmonary vs systemic circulation
- Pulmonary: right heart → lungs (pick up O2, release CO2) → left heart.
- Systemic: left heart → systemic tissues (exchange gases/nutrients/wastes) → right heart.
- Basic loop: right heart → lungs → left heart → body → right heart.
Heart location and coverings
- Lies in the mediastinum, posterior to sternum, slightly left; apex points anteroinferiorly.
- Pericardium: fibrous sac + serous layers (parietal and visceral/epicardium) with pericardial cavity.
- Pericarditis: inflammation → fluid accumulation → possible cardiac tamponade (impaired filling).
External anatomy & chambers
- Four chambers: two atria (receive blood) and two ventricles (pump blood away).
- Great vessels: SVC/IVC → right atrium; pulmonary trunk/veins connect ventricles and lungs; aorta from left ventricle.
- Surface grooves: coronary sulcus (atria–ventricle boundary) and interventricular sulci (between ventricles) house coronary vessels.
Heart wall layers and wall thickness
- Layers: epicardium (visceral pericardium), myocardium (cardiac muscle), endocardium (endothelium).
- Ventricles thicker than atria; left ventricle thickest because it pumps to systemic circuit.
Internal features of chambers
- Right atrium: pectinate muscles, fossa ovalis, receives SVC/IVC/coronary sinus.
- Ventricles: trabeculae carneae; papillary muscles attach chordae tendineae to AV valve cusps.
- Valves ensure one-way flow: AV valves (tricuspid/right, bicuspid/mitral/left) and semilunar valves (pulmonary, aortic).
Valves, fibrous skeleton, and heart sounds
- AV valves close at ventricular contraction; papillary muscles + chordae prevent prolapse.
- Semilunar valves close when arterial pressure exceeds ventricular pressure.
- Fibrous skeleton: dense connective tissue rings that anchor valves and electrically insulate atria from ventricles.
- Heart sounds: S1 = AV valves closing; S2 = semilunar valves closing. Murmurs arise from turbulent flow (insufficiency or stenosis).
Coronary circulation (blood supply to heart)
- Coronary arteries (left/right) branch from ascending aorta; major branches: anterior interventricular, circumflex, right marginal, posterior interventricular.
- Coronary flow is intermittent: vessels are compressed during ventricular systole and fill mainly during diastole.
- Coronary veins drain into coronary sinus → right atrium.
- Clinical: atherosclerosis, spasm → angina or myocardial infarction (MI).
Cardiac muscle microscopic structure & metabolism
- Cardiac muscle fibers are short, branched, striated, with one or two central nuclei and abundant mitochondria.
- Cells connected by intercalated discs (desmosomes for strength, gap junctions for electrical coupling → functional syncytium).
- Mostly aerobic metabolism; uses fatty acids, glucose, lactate, amino acids, ketones — vulnerable to ischemia.
Conduction system & autonomic control
- Conduction components: SA node (pacemaker), atrial pathways, AV node, AV bundle (His), left/right bundle branches, Purkinje fibers.
- Sequence: SA node → atrial depolarization → AV node (delay) → AV bundle → bundle branches → Purkinje fibers → ventricular depolarization.
- Delay at AV node allows ventricular filling.
- Autonomic input: parasympathetic (vagus) decreases HR; sympathetic increases HR and contractility and dilates coronary vessels.
Electrical activity: nodal vs ventricular cells
- SA nodal (pacemaker) cells: unstable membrane potential (pacemaker potential); typical values: \(RMP\approx -60\text{ mV}\), threshold near \(-40\text{ mV}\).
- Phases: slow Na+ influx (pacemaker depolarization) → opening of fast Ca2+ channels (depolarization) → K+ efflux (repolarization).
- Ventricular (cardiac muscle) cells: resting potential \(\approx -90\text{ mV}\).
- Action potential phases: rapid Na+ depolarization → long Ca2+–K+ plateau → repolarization (K+ out).
- Long plateau produces long refractory period (~250 ms) → prevents tetany.
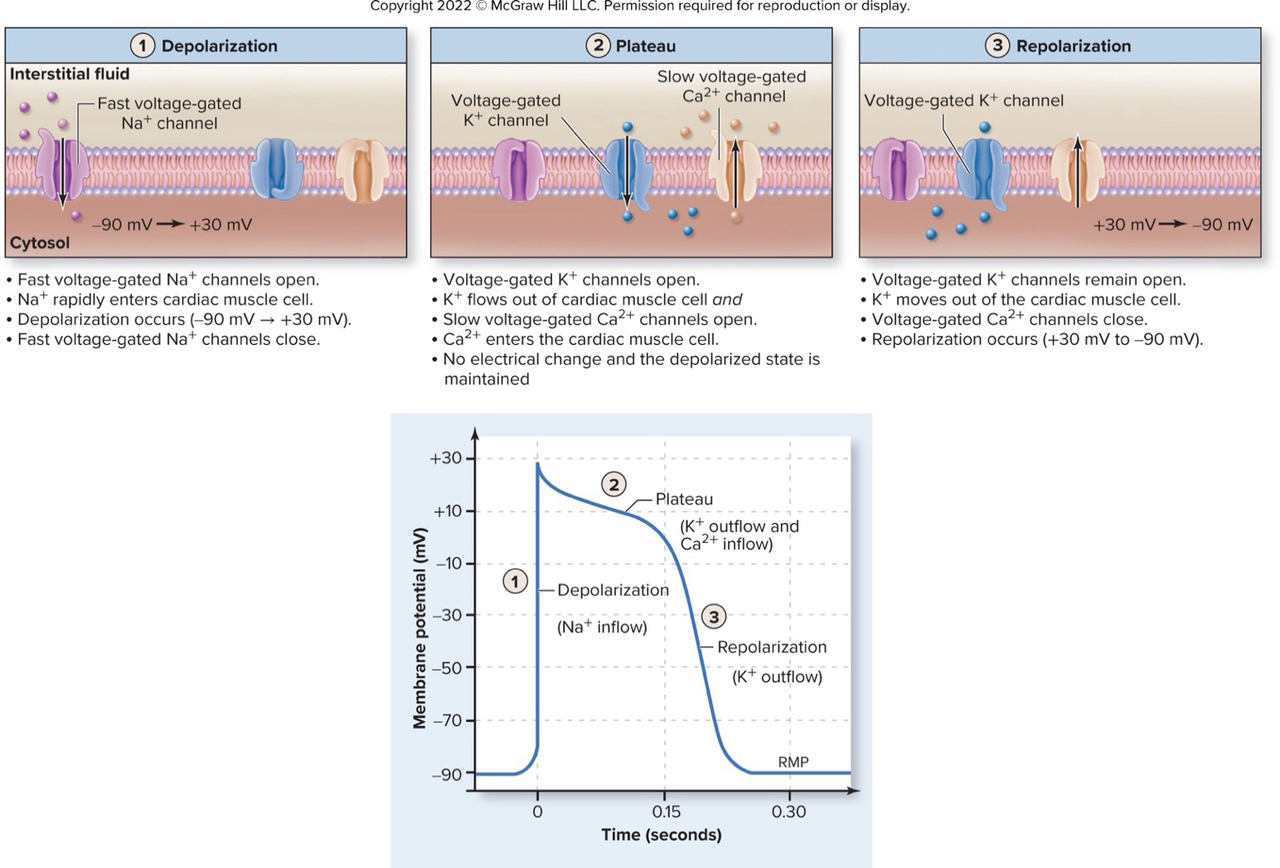 Alt text: Cardiac muscle action potential phases: depolarization, plateau, repolarization.
Alt text: Cardiac muscle action potential phases: depolarization, plateau, repolarization.
ECG basics
- ECG waves: P = atrial depolarization, QRS = ventricular depolarization (atrial repolarization hidden), T = ventricular repolarization.
- Important intervals: P–R (P–Q) = conduction through atria and AV node; Q–T = ventricular AP duration.
- ECG segments (PQ, ST) reflect plateau phases (no gross electrical change).
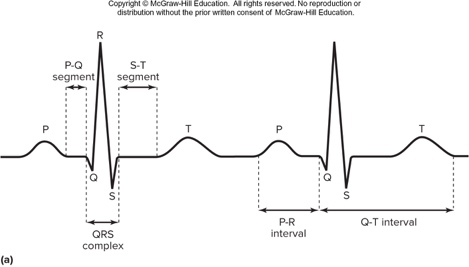 Alt text: ECG with P, QRS, and T waves labeled.
Alt text: ECG with P, QRS, and T waves labeled.
- Clinical arrhythmias: AV blocks (1st–3rd degree), PVCs, atrial fibrillation, ventricular fibrillation (life‑threatening), treated with pacemaker or defibrillation as needed.
Cardiac cycle — phases and key volumes/pressures
- Cardiac cycle = all events from start of one heartbeat to the next; includes systole (contraction) and diastole (relaxation).
- Main phases: atrial contraction → isovolumic ventricular contraction → ventricular ejection → isovolumic relaxation → passive ventricular filling.
- Important volumes:
- End-diastolic volume (EDV): volume in ventricle at end of filling.
- End-systolic volume (ESV): volume after ejection.
- Stroke volume (SV): blood ejected per beat: \(SV = EDV - ESV\) (example: \(60\,\text{mL} = 130\,\text{mL} - 70\,\text{mL}\)).
Alt text: Cardiac cycle phases with ECG, pressure, and volume curves.
Cardiac output and its determinants
- Cardiac output (CO): volume pumped by one ventricle per minute: \(CO = HR \times SV\) (L/min).
- Stroke volume (SV) depends on: preload (venous return), contractility (inotropic state), and afterload (arterial resistance).
Frank–Starling law (preload)
- Greater EDV → increased sarcomere stretch → stronger contraction → increased SV; this balances output between right and left sides.
Inotropic agents (contractility)
- Positive inotropes (↑ Ca2+ availability): e.g., sympathetic NE/EPI via β1 receptors, digitalis; increase SV.
- Negative inotropes: reduce Ca2+ availability (e.g., Ca2+ channel blockers) and lower SV.
Afterload
- Resistance ventricles must overcome to eject blood (arterial pressure). Increased afterload (e.g., atherosclerosis) reduces SV.
Heart-rate control (chronotropic influences)
- Positive chronotropes: sympathetic stimulation, NE/EPI, thyroid hormone, caffeine, nicotine, cocaine (increase SA node firing).
- Negative chronotropes: parasympathetic (ACh via vagus opens K+ channels), beta‑blockers (block β1 receptors).
- Atrial (Bainbridge) reflex: increased venous return → atrial stretch → reflex tachycardia to prevent overfilling.
Selected clinical correlations (concise)
- Congestive heart failure (CHF): pump failure → systemic or pulmonary edema depending on ventricle involved.
- Pericarditis: can cause tamponade (impaired filling) and friction rub on auscultation.
- Myocardial infarction: occluded coronary artery → ischemia → necrosis; acute chest pain, diaphoresis, nausea.
- Arrhythmias: conduction blocks or fibrillation may require pacing or defibrillation.
High-yield formulas & values
- \(CO = HR \times SV\) (cardiac output)
- \(SV = EDV - ESV\) (stroke volume)
- Typical pacemaker RMP: \(\approx -60\text{ mV}\) (SA node); ventricular RMP \(\approx -90\text{ mV}\).
Study tips
- Memorize conduction sequence and ECG correlations (SA → P wave; AV delay → PR interval; ventricles → QRS; repolarization → T).
- Practice labeling cardiac cycle pressure/volume curves and relating valve state to pressure differences.
- Relate physiology to clinical problems: how valve disease, infarction, or arrhythmias alter volumes, pressures, and ECG.