Sign up to unlock more features
- Save this deck to your account
- Study flashcards with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from PDFs and documents
- Better text extraction from your PDFs and documents
- Better flashcards with our more advanced AI model
A 67-year-old woman with _______ is being prepared for discharge after treatment of a _______. What is the most appropriate vaccine for this patient?
This patient has received pneumococcal and influenza vaccines _______ ago. She is currently receiving her first course of _______.
Annual vaccination starting at age > 6 months is recommended by the CDC for _______.
Influenza is a respiratory viral illness that can lead to complications such as _______ and higher risks if not vaccinated in _______ patients.
Symptoms of influenza include _______, _______, _______, and _______.
The best option for this patient is to receive the _______ vaccine over the other vaccines listed.
The _______ vaccine is contraindicated in severely _______ patients due to the risk of viral reactivation.
Meningococcal vaccine is safe for _______ patients but boosters are not routinely necessary.
The pneumococcal vaccine is indicated for adults over _______ years and for patients with high-risk conditions.
Annual _______ for influenza virus should be administered especially to patients like this one who are _______.
The primary viral illness discussed is _______, which can lead to complications such as _______ and _______ in vulnerable patients.
Key symptoms of _______ include fever, chills, myalgias, malaise, headaches, cough, nausea, and vomiting.
The Centers for Disease Control (CDC) advises annual vaccination against _______ starting at age _______.
The influenza vaccine can be given as a _______ of inactivated virus or as a _______.
Inactivated influenza vaccine is safe for administration to _______ who are at risk for severe illness.
Influenza is characterized as a seasonal illness affecting patients primarily in _______.
Patients who are _______ should receive annual vaccination against _______ to prevent complications.
The _______ is a live attenuated vaccine not recommended for severely _______ due to reactivation risk.
The _______ is a conjugate vaccine indicated for all children and can be safely administered to _______.
The _______ is indicated for adults over _______ and for those with high-risk conditions.
A patient who received the _______ 1 year ago does not require a _______.
The _______ is a live attenuated vaccine administered in two doses, typically during childhood.
The _______ is recommended for adults over _______ to prevent _______ and is also a live attenuated vaccine.
The _______ is contraindicated in patients who are _______.
For immunocompromised patients, administering the _______ can prevent severe illness and complications.
The most appropriate next step in diagnosis for a woman with high-risk sexual behavior and recurrent episodes of vaginal candidiasis and genital herpes is _______.
A 27-year-old woman presents with vaginal discharge and itching. Her previous medical history includes three episodes of _______ and three episodes of _______.
Recurrent episodes of _______ and _______ suggest the potential for underlying _______ that may occur with _______.
Routine one-time screening for _______ is recommended for most sexually active individuals over the age of _______.
Testing for HIV typically involves a _______.
If the fourth-generation HIV test is positive, further antibody testing to differentiate between infection with _______ or _______ is indicated.
The gold standard for diagnosing genital herpes is _______, although PCR-based tests are preferred due to higher sensitivity.
The diagnosis of vaginal candidiasis can be made clinically without the use of _______ as yeast forms can be seen on microscopy.
Possible underlying immunodeficiency in sexually active individuals with recurrent genital infections includes a risk for _______.
Patients engaging in high-risk sexual behaviors should be tested for _______ more frequently than those with lower risk.
Highly active antiretroviral therapy (HAART) should be initiated immediately upon a _______ result.
Pelvic examination reveals a _______ with a cottage-cheese consistency, characteristic of _______.
A woman presents with a vaginal discharge and has had multiple partners, indicating a risk for _______.
For patients with high-risk sexual behavior and recurrent episodes of vaginal candidiasis, the most appropriate diagnostic step is to perform _______.
Routine screening for HIV is recommended for sexually active individuals over the age of _______.
Populations at higher risk for HIV include individuals with numerous sexual partners and those who _______.
Co-existing conditions like recurrent vaginal candidiasis may suggest underlying _______ associated with advanced HIV infection.
HIV testing typically involves using a _______.
If the fourth-generation HIV test is positive, further antibody testing is indicated to distinguish between _______ and _______ infections.
In cases where the fourth-generation test is positive but antibody testing yields negative or indeterminate results, it is crucial to measure the _______.
A positive HIV test warrants immediate initiation of _______.
Fungal culture is unnecessary for diagnosing _______ since yeast forms can be identified through microscopy of vaginal secretions.
Genital herpes infection can typically be diagnosed clinically, but laboratory confirmation is necessary during the _______.
While testing for _______ is important, the preferred screening method is cervical cytology or cervical cytology plus a PCR-based assay.
Colposcopy is indicated in patients only if their pap smear reveals _______ such as cervical dysplasia.
HIV testing is especially advised for sexually active patients displaying symptoms like _______.
A patient with recurrent infections may indicate a state of _______ that could be a hallmark of HIV infection.
After starting _______ for cellulitis, a 37-year-old woman developed symptoms leading to suspicion of _______.
Symptoms of {_______} include pruritic rash, _______, and _______ after exposure to an allergen like dicloxacillin.
The patient's vital signs show hypotension at _______ and oxygen saturation of _______ on room air, indicating severe complications.
Immediate treatment for anaphylaxis includes administration of _______ to reverse the IgE-mediated mast cell degranulation.
In anaphylaxis, adjunctive treatments may include _______, glucocorticoids, and _______.
Patients with suspected anaphylaxis should leave with an _______ and instructions on usage, reinforcing the urgency of response.
Incorrect choices for immediate treatment in this anaphylactic case are _______, _______, and _______.
The defining feature of _______ is the rapid onset of symptoms due to IgE-mediated reactions, leading to potential circulatory collapse.
Failure to treat anaphylaxis promptly may result in _______ from hypoxia and/or _______.
In managing anaphylaxis, signs such as _______ and _______ can indicate the seriousness of the condition.
Histaminergic responses in anaphylaxis involve multiple organ systems resulting in _______ and _______.
In cases of _______, administration of _______ is the most appropriate immediate step in management.
Anaphylaxis is a type 1 hypersensitivity reaction characterized by _______.
Symptoms of anaphylaxis include _______, _______, _______, and _______.
The immediate risk in anaphylaxis is _______ and _______.
The diagnosis of anaphylaxis is made _______.
Adjunctive medications in the management of anaphylaxis include _______, _______, and _______.
If medications are suspected to cause anaphylaxis, an allergy warning should be placed in the patient's _______.
All patients discharged after anaphylaxis should be provided with an _______.
Patients should be educated about their allergy and advised to avoid _______ within the same class in the future.
Loratadine is a second-generation antihistamine, considered an _______ in anaphylaxis.
Prednisone is frequently given in anaphylaxis but has little _______ on the disease process.
Stanozolol is a synthetic steroid that is _______ for the treatment of anaphylaxis.
Anaphylaxis should be suspected in patients with acute onset of _______ and evidence of _______.
Additional interventions for anaphylaxis should focus on maintaining _______ and ensuring patency of the _______.
In the management of anaphylaxis, correct dosage of epinephrine is essential for rapid _______ in symptoms.
If a patient presents with symptoms of _______, the first line treatment is adminstration of _______.
Education on recognizing early signs of _______ can be crucial for prompt intervention.
It is important to differentiate between _______ and other causes of dyspnea during anaphylaxis diagnosis.
Administering _______ can help manage blood pressure during anaphylactic shock.
Referral to an _______ may be necessary for patients with recurrent anaphylaxis.
Immediate treatment of anaphylaxis can prevent complications such as _______ and _______.
In anaphylaxis scenario, a patient may present with _______ and _______.
Anaphylaxis can occur after exposure to allergens such as _______, _______, or _______.
A clinical scenario may include a febrile neonate under _______ leading to investigations for potential infections.
Pain management in sickle cell disease is important to reduce patient _______.
The clinical scenario involves a 47-year-old man who presents with a 3-month history of progressively worsening fatigue and a weight loss of _______. What is the most likely confirmatory test for the diagnosis of chronic myelogenous leukemia (CML)?
The presence of which fusion protein is most likely to confirm the diagnosis of chronic myelogenous leukemia (CML)? _______ fusion protein.
Chronic myelogenous leukemia (CML) is characterized by a translocation between chromosomes _______ and _______.
The BCR/ABL fusion protein is associated with the Philadelphia (Ph) chromosome and results in activation of _______ kinase protein, leading to increased hematopoietic proliferation.
Typical laboratory findings in chronic myelogenous leukemia (CML) include leukocytosis with an increase in nearly all cell lines, including _______ and _______.
The treatment for chronic myelogenous leukemia (CML) primarily involves the use of _______ such as imatinib or dasatinib.
In CML, leukostasis is uncommon but can occur; it leads to end organ damage from occlusion of capillaries by _______.
The BRCA1 oncogene is primarily associated with which types of cancer? _______ and _______ cancer.
P-glycoprotein functions as an efflux pump that can lead to _______ in leukemic cells.
The presence of p53 suppressor gene is not a confirmatory marker for chronic myelogenous leukemia (CML), but serves as a _______.
A characteristic feature of acute leukemias, which can be distinguished from chronic myelogenous leukemia (CML), is the presence of _______ in the blood.
The diagnosis of _______ is confirmed by the presence of the _______ resulting from the Philadelphia (Ph) chromosome.
The Philadelphia (Ph) chromosome is formed by a translocation between chromosomes _______ and _______.
Activation of the ABL kinase protein leads to activation of the _______ and _______ pathways, promoting unregulated cellular proliferation in CML.
Typical laboratory findings in CML include _______, with an increase in nearly all cell lines, and characteristic _______ and _______.
Leukostasis, a condition that can arise in CML, is due to the occlusion of capillaries by _______.
Treatment for CML primarily involves _______ such as _______ or _______.
The BRCA1 oncogene is involved in breast and ovarian cancer and is classified as a _______.
Mutations in the BRCA1 gene lead to an increased risk for _______ due to its role in _______.
P-glycoprotein is an _______ that can render leukemic cells resistant to chemotherapy by transporting agents out of the cell.
The p53 tumor suppressor gene is mutated in nearly half of all cancers, but its loss of function does not confirm the diagnosis of _______.
t(8,16) translocation is associated with a subtype of _______, not _______.
Patients with acute leukemias have circulating _______ present on the peripheral blood smear.
A 42-year-old woman with paraplegia and recurrent urinary tract infections presents with decreased hemoglobin concentration due to _______. What type of anemia is she likely experiencing?
Chronic inflammation in this patient leads to an increase in _______ production, decreasing responsiveness of the bone marrow to erythropoietin. What condition does this represent?
Impaired iron absorption due to cytokine-induced erythropoietin deficiency leads to functional iron deficiency despite adequate {c1::iron stores}}. What does this result in?
The laboratory findings in this patient with anemia due to chronic disease include normal to slightly increased _______ concentration, decreased _______, and decreased total iron-binding capacity (TIBC). What does each indicate?
To manage anemia of chronic disease effectively, treatment must focus on addressing the underlying _______. What is a common contributing factor to this condition?
Cytokine-induced erythropoietin deficiency contributes to a state of functional _______ due to retained iron within the reticuloendothelial system. How does this affect erythropoiesis?
In the context of anemia, what does the acronym ACD stand for? _______. Which cytokines are involved in this process?
Laboratory results show the following values for the patient: Hemoglobin: 8.7 g/dL, Mean corpuscular volume: 90 μm³. What condition might these results suggest? _______.
Given the patient has no abnormalities other than paraplegia and a history of urinary tract infections, what is the most plausible diagnosis contributing to her anemia? _______.
What is one of the key inflammatory substances that leads to increased hepcidin production? _______. What role does it play in anemia?
This patient’s normocytic anemia can be classified as ACD, which is common in patients with _______. Can you name other conditions associated with this?
Deficiencies such as folic acid or iron can present with similar symptoms to anemia of chronic disease, but what distinguishes ACD is the increased _______ levels affecting iron metabolism.
Chronic inflammation reduces erythropoiesis primarily by decreasing the bone marrow's response to erythropoietin through enhanced production of _______. Name two specific examples.
Cytokine-induced erythropoietin deficiency is the most likely cause of this patient's normocytic anemia, which is commonly referred to as _______. ACD is common in patients with _______.
Chronic inflammation leads to an increase in _______ production, which causes a _______ and retention of iron within the _______.
In ACD, iron is retained within the RES and cannot be effectively accessed for _______, resulting in either _______ and a reduced number of _______.
Laboratory findings in ACD typically show a normal to slightly increased _______, decreased _______, and decreased _______.
Treatment for ACD must focus on treating the underlying disease to decrease _______ which is critical for managing this condition.
Folic acid deficiency is relatively uncommon but may lead to _______ in patients with alcohol use disorder or other nutritional deficiencies. This patient exhibits no risk factors for _______.
Glucose 6-phosphate dehydrogenase deficiency can lead to hemolysis under oxidative stress, presenting with anemia and increased _______, _______, and _______.
Iron deficiency anemia presents similarly to ACD but can be distinguished by iron studies showing decreased _______ and decreased _______.
Myelodysplasia describes a genetically diverse set of disorders affecting _______ of the bone marrow, possibly leading to anemia, neutropenia, or _______.
Educational objectives emphasize that ACD is common in patients with _______ and those with _______.
A 32-year-old African American man with _______ comes for a follow-up examination. Which of the following is the most likely _______? A) Celiac disease, B) Myelodysplastic syndrome, C) Occult gastrointestinal bleeding, D) Pure red cell aplasia, E) Thalassemia.
The lab findings of this 32-year-old African American man with iron deficiency anemia include a hemoglobin of _______ and a hematocrit of _______ today, indicating _______.
In patients with thalassemia, the red cell distribution width (RDW) is typically _______. This differs from other causes of anemia like iron deficiency.
Mild microcytic anemia with a normal RDW and normal iron studies suggests the diagnosis of _______.
The serum iron level for this patient was _______ with a transferrin saturation of _______. This supports the diagnosis of _______ over iron deficiency anemia.
The patient is a _______ with a history of smoking and moderate alcohol consumption, presenting with _______.
The presence of _______ and _______ in the blood smear is indicative of thalassemia.
The hemoglobin levels have increased from _______ six months ago to _______ today, suggesting response to treatment for _______.
The most likely diagnosis in a 32-year-old African American patient with mild _______ and normal RDW who hasn't responded to iron therapy is _______.
Thalassemia interferes with normal synthesis of _______ due to nonfunctional alleles of the _______.
Normal adult hemoglobin consists of two _______ and two _______.
Patients with β-thalassemia have deficient _______, leading to ineffective assembly of normal HbA and formation of insoluble _______.
The severity of α-thalassemia depends on the number of _______.
Microcytosis and _______ on peripheral blood smear are characteristic of both α- and β-thalassemia.
Thalassemia trait is often incorrectly diagnosed as _______.
Oral iron therapy will have no effect on hemoglobin concentrations in patients with _______.
A transferrin saturation of _______ is often used to exclude iron deficiency anemia.
Celiac disease can lead to iron deficiency presenting with _______, increased RDW, and transferrin saturation below 20%.
Myelodysplastic syndrome often presents with cytopenias, but microcytic anemia in isolation would be _______.
Occult gastrointestinal bleeding leads to iron deficiency anemia that should respond to oral _______.
Additional findings for celiac disease may include _______, _______, or other gastrointestinal symptoms.
Halo cells are present in peripheral blood smears of patients with _______.
Combination therapy with folate and iron may be necessary due to normal iron studies in patients with _______.
A definitive way to distinguish α- from β-thalassemia is through _______.
The correct answer in the multiple-choice scenario of a patient with anemia and unresponsive to iron therapy is _______.
In an African American patient with mild microcytic anemia, thalassemia is most likely when hemoglobin concentrations are normal despite several months of iron therapy and the red cell distribution width (RDW) is also normal, indicating that thalassemia is an inherited condition affecting the _______ genes.
Normal adult hemoglobin A (HbA) consists of two _______ subunits and two _______ subunits, which together form a unique conformation that has a high affinity for oxygen.
Deficient _______ genes in β-thalassemia prevent effective assembly of HbA, causing excess _______ chains to form insoluble tetramers.
Patients with a-thalassemia trait can be asymptomatic but commonly present with _______ and may have a minimal decrease in hemoglobin concentration.
Microcytosis and target cells on a peripheral blood smear characterize both a-thalassemia and _______.
To distinguish between thalassemia and iron deficiency anemia, hemoglobin _______ is used, as patients with thalassemia often present with normal iron studies.
In patients diagnosed with thalassemia minor, oral _______ therapy does not affect hemoglobin concentrations because they typically do not have iron deficiency.
A transferrin saturation of _______ is often used to exclude iron deficiency anemia in patients presenting with mild microcytic anemia.
Celiac disease can lead to iron deficiency anemia, presenting with microcytic anemia and an increased _______ alongside expected findings of weight loss and diarrhea.
Myelodysplastic syndrome may present with diverse cytopenias but microcytic anemia in isolation is _______.
Occult gastrointestinal bleeding typically leads to iron deficiency anemia that should respond to _______ therapy, which does not occur in thalassemia.
Pure red blood cell aplasia results in complete destruction of erythrocyte precursors in the bone marrow leading to profound _______.
Normal human hemoglobin A consists of two _______ and two _______ subunits, and mutations in these alleles lead to thalassemia variants.
In the case of thalassemia trait or thalassemia minor, patients present with _______ and normal iron studies.
Peripheral blood smear findings for thalassemia may show _______ indicating thalassemia presence in relevant patients.
The severity of anemia in thalassemia is dependent on the number and _______ of mutations present within the globin genes.
Patients with thalassemia who have multiple nonfunctional alleles may present with increasingly _______ levels of anemia.
In managing a patient with _______ experiencing an acute painful episode, the most appropriate next step in pharmacotherapy is _______.
A 23-year-old man with _______ presents with severe low back pain rated at 8 out of 10. His hemoglobin concentration is _______.
Patients with _______ often experience vaso-occlusive phenomena, which can lead to acute painful episodes referred to as _______.
For acute painful crises in patients with _______, the preferred route of administration for analgesics is _______.
Oral medications such as _______ and _______ are generally ineffective for managing acute pain crises in patients with _______.
In the case of a patient with acute pain crises due to _______, it is crucial to prioritize the administration of _______ over further diagnostics.
A 23-year-old man with sickle cell disease experiences nausea and decreased intake of solids and liquids. This can complicate treatment by requiring a switch to _______ routes for medication delivery.
Rapid assessment is critical in patients with sickle cell disease to rule out concomitant disorders like _______ and _______.
Chronic exposure to opiates in patients with _______ often results in the need for _______ of opiate medication compared to opiate-naive patients.
The lab findings for a 23-year-old man with sickle cell disease show hemoglobin at _______ and creatinine at _______.
Vaso-occlusive events in patients with _______ can manifest as pain in areas such as the _______, abdomen, or long bones.
Patients in pain crises due to _______ may present with additional symptoms including _______.
Among the medications considered for treatment, the most appropriate for acute pain in sickle cell disease is _______ over _______ or lesser opioids.
If a patient experiences hypovolemia during a painful episode of _______, the healthcare provider must also prioritize _______.
In treating acute pain crises in patients with _______, intravenous morphine is preferred as it provides a faster onset of _______.
Administering adequate analgesia for painful crises in patients with _______ is crucial and should not be delayed for diagnostics involving _______.
In the management of sickle cell disease pain episodes, intravenous morphine is considered the first-line medication to manage acute _______.
In patients with _______, acute painful episodes often referred to as _______, occur due to _______.
The most appropriate medication for patients experiencing an acute painful episode due to _______ is _______.
Assessment for accompanying disorders such as acute chest syndrome, myocardial infarction, and _______ is critical during pain crises in patients with _______.
Intravenous administration is preferred for analgesia in acute painful crises of _______ because oral medications may not provide adequate relief due to low _______.
Rapid administration of _______ is crucial for managing pain crises in patients with _______, often guided by an individualized pain pathway.
Chronic exposure to opiates in patients with _______ commonly leads to a need for higher opiate doses compared to _______.
Patients with sickle cell disease may experience pain in various areas, including the _______, _______, _______, and _______.
For acute painful episodes, the preferred treatment involves intravenous _______ rather than oral medications such as _______ or _______.
Intravenous _______ is rarely recommended for acute pain in sickle cell disease due to its challenging pharmacodynamics and _______.
Proper treatment of pain crises in patients with sickle cell disease prioritizes reversing features like _______ and _______.
Acute painful crises in patients with sickle cell disease necessitate simultaneous assessment for conditions such as _______ during pain management.
The patient in this clinical scenario is a 72-year-old man with a history of poorly controlled hypertension. His current blood pressure is _______. What is the greatest risk factor for cerebral infarction in this patient? A) Abnormal serum lipid concentrations B) Family history of cerebral infarction C) _______ D) Increase in serum glucose concentration E) Smoking history
Hypertension is considered the greatest _______ for cerebral infarction. Uncontrolled hypertension increases the risk for _______ by approximately two-fold. These risks remain even when hypertension is _______.
In stroke prevention, initiating _______ is crucial. Additional lifestyle modifications include _______, dietary changes, smoking _______, and _______.
Abnormal serum lipid concentrations are not consistently considered a risk factor for all stroke subtypes. However, they may play a _______ in the development of ischemic strokes in large vessel or _______.
A family history of cerebral infarction is considered an important, non-modifiable risk factor but is not as significant as _______. It has not been consistently demonstrated as a risk factor in large studies.
An increase in serum glucose concentration, particularly in the context of _______, is a significant risk factor for ischemic stroke but is not as impactful as _______.
The greatest modifiable risk factor for cerebral infarction is _______. It contributes significantly to the development of cardiac and renal failure and atherosclerotic disease.
Uncontrolled _______ is associated with an approximately two-fold increase in the risk for ischemic stroke.
Even when _______ is well-controlled, the risk for ischemic stroke remains incompletely eliminated.
Initiation of antihypertensive therapy is an important component of _______, along with lifestyle modification such as weight loss and regular exercise.
Abnormal serum lipid concentrations may play a modest role in the development of _______, especially in large vessel or lacunar distributions.
Family history of cerebral infarction is considered an important _______ but is not as significant as hypertension in stroke risk.
Increase in serum glucose concentration, especially in the setting of diabetes mellitus, is a notable risk factor for _______, but less significant than hypertension.
The relative risk of smoking history for ischemic stroke is less than that of _______.
The educational objective is that _______ is the single most important modifiable risk factor for cerebral infarction.
Uncontrolled hypertension increases the risk for ischemic stroke, contributing significantly to stroke pathophysiology and requiring comprehensive _______.
C) _______ is the correct answer for the greatest modifiable risk factor for cerebral infarction.
A clinical scenario presents a 77-year-old woman with severe degenerative arthritis who has a 2-week history of ringing and pain in her ears. Which of the following laboratory findings is most likely in this patient? Na+: _______, K+: _______, Cl-: _______, HCO3-: _______, pH: _______.
Salicylate poisoning primarily affects the body by causing respiratory alkalosis due to _______. This leads to _______ and delayed _______.
In cases of acute salicylate toxicity, patients typically present with symptoms such as _______, _______, and _______. Other symptoms may include _______ and _______.
Management of acute or chronic salicylate toxicity generally involves systemic _______ using a sodium bicarbonate infusion. In severe cases, patients may require _______.
Mild salicylate toxicity is characterized by an increased _______ and a compensated _______.
Aspirin irreversibly inactivates cyclooxygenase, preventing the conversion of arachidonic acid to _______, which reduces _______.
Salicylate toxicity would not typically cause hyponatremia, hyperkalemia, or hypokalemia. Specifically, hyperkalemia may occur due to _______ or _______.
Key features of patients with chronic salicylate ingestion can include symptoms similar to acute toxicity or mild symptoms such as _______, _______, and _______.
Anion gap metabolic acidosis is secondary to the production of _______ and _______ in salicylate toxicity.
Salicylate toxicity can present with defining features such as _______, _______, _______, _______, _______, _______, and _______.
Aspirin irreversibly inactivates _______, which prevents the conversion of arachidonic acid to _______.
In high doses, salicylate poisoning leads to early _______ followed by a _______ due to decoupling effects on the electron transport chain.
Management of acute or chronic salicylate toxicity includes systemic alkalinization with _______.
Acute salicylate toxicity may present with increased anion gap and _______.
Patients with chronic salicylate ingestion may present identical symptoms to acute toxicity, or with mild symptoms such as _______, _______, _______, or _______.
Salicylate toxicity typically does not result in changes in sodium or potassium serum concentrations in major ways, unlike conditions resulting in _______ or _______.
Patients may need dialysis in cases of severe altered mental status, renal failure, pulmonary edema, or _______.
Incorrect answers to the multiple choice question about salicylate toxicity included: A) _______, B) _______, D) _______.
A 23-year-old woman presents with a lesion on her lip that appeared 1 day ago. She also reports a tingling and burning sensation in that area for the past 4 days. Examination reveals a grouping of discrete, clear, fluid-filled vesicles measuring 5 mm in diameter. The most likely diagnosis is _______.
Herpes simplex virus (HSV) infection commonly causes oral infections known as _______ that begin with vesicle formation at the oral-labial margin.
Prodromal symptoms of herpes simplex may include _______, _______, _______, or _______ in the area prior to vesicular lesions.
Following initial infection, herpes simplex virus may remain _______ in the _______ until reactivation occurs.
Reactivation of herpes simplex can be triggered by factors such as _______, _______, or _______.
Diagnosis of herpes simplex is confirmed with viral culture or _______ testing from the base of the lesion if uncertain.
Antiviral agents that inhibit viral DNA polymerase, including _______, _______, and _______, are used in the treatment of herpes simplex.
Chickenpox, or _______, does not present with localized vesicular lesions at the oral-labial margin, unlike herpes simplex.
Erythema multiforme is characterized by targetoid lesions and may be triggered by _______ (especially _______) or infections.
Erythema nodosum is another condition differentiated from herpes simplex and is characterized by _______ on the lower extremities.
The correct answer for a lesion on the lip with fluid-filled vesicles, tingling, and burning in a 23-year-old woman is _______.
The infection caused by _______ is commonly known as _______.
Herpes labialis typically begins with the formation of _______ at the _______.
The vesicles in herpes labialis lyse and progress to shallow, painful _______ with an _______.
Prodromal symptoms of herpes labialis may include _______, _______, _______, or _______.
Herpes simplex is most often caused by _______ but can also be caused by _______.
Following initial infection, HSV may be latent in the _______ until reactivation.
Reactivation of HSV may be triggered by factors such as _______, _______, or _______.
The diagnosis of herpes labialis can be confirmed with a _______ or a _______.
Treatment for herpes labialis includes antiviral agents that inhibit _______.
Common antiviral agents for herpes simplex include _______, _______, and _______.
The duration of an outbreak of herpes labialis may be shortened by using antiviral agents such as _______.
Unlike herpes simplex, chickenpox is caused by _______ (VZV), also known as _______.
Reactivation of varicella-zoster virus can lead to _______, characterized by multiple vesicular lesions in a _______, dermatomal distribution.
Erythema multiforme is characterized by targetoid lesions on the _______, _______, _______, and _______.
Erythema multiforme may be associated with conditions such as _______, infections, or specific viruses (e.g., _______).
Erythema nodosum presents as painful, immobile nodules on the _______, and lesions are typically _______.
The causes of erythema nodosum can include conditions like _______, _______, or reactions to _______.
Herpes labialis is also known to present with painful vesicles and _______ on the lip during reactivation.
A 42-year-old man has a 3-month history of a progressive rash on his arms and back. The most likely diagnosis is _______.
The rash associated with psoriasis often presents with sharp, defined, _______ plaques covered with _______.
The removal of the white scale of psoriasis leads to _______, known as _______.
Common treatments for psoriasis include: topical _______, topical _______, and if refractory, consider _______ or _______.
Plaque psoriasis is also known as _______.
Other forms of psoriasis include _______, _______, and _______.
Patients with psoriasis may exhibit _______, most commonly _______.
The patient in the clinical scenario presented with a rash that is mildly _______.
An otherwise healthy individual presenting with a rash over 3 months could be indicative of conditions like _______, _______, or _______.
The pulse rate of the patient was recorded at _______.
The blood pressure of the patient was measured at _______.
When diagnosing skin conditions, consider the duration, appearance, and _______ of the rash.
The key features to identify psoriasis include _______ and _______.
Psoriasis is a common inflammatory skin condition caused by _______ leading to _______.
The most common presentation of psoriasis is _______, also known as _______.
Plaque psoriasis presents with _______ with a _______.
Psoriasis lesions commonly appear on the _______ and can cause _______.
Removal of the white scale in psoriasis causes _______ known as _______.
Patients with psoriasis may exhibit nail changes, most commonly _______.
Treatment for psoriasis includes topical therapies such as _______ and _______.
If psoriasis is refractory to topical therapies, then _______, _______, or _______ may be considered.
Atopic dermatitis is commonly known as _______ and may be characterized by _______ and _______ lesions.
Bullous pemphigoid is characterized by antibodies against the _______ and presents with _______.
Dysplastic nevi are benign, acquired melanocytic lesions that may rarely transform into _______.
Lichen simplex chronicus results from repetitive _______ or _______ of the skin.
Pityriasis rosea commonly involves the _______ and proximal _______.
Pityriasis rosea is often induced by a viral infection including human herpesvirus _______ and _______.
Incorrect choices for diagnosing psoriasis include A) _______, B) _______, C) _______, D) _______, and E) _______.
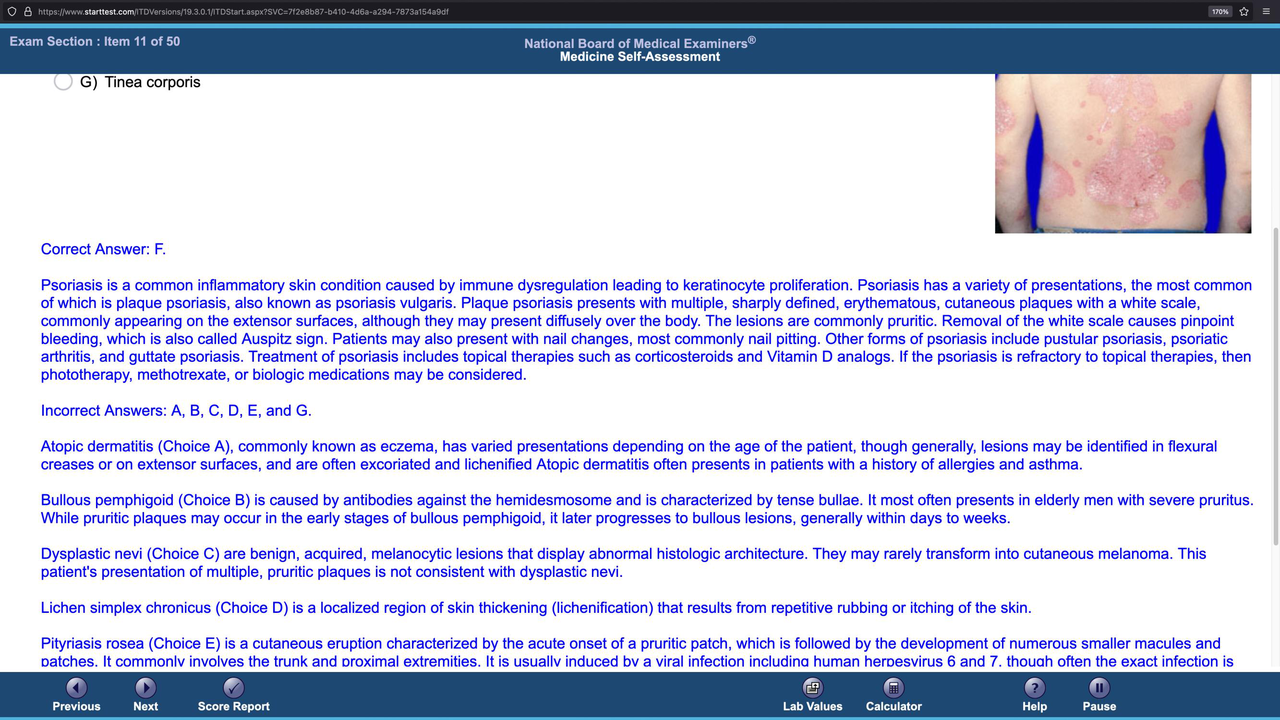 This image shows a rash on a person's back typical for _______.
This image shows a rash on a person's back typical for _______.
Flashcards in this deck (297)
-
A 67-year-old woman with non-Hodgkin lymphoma is being prepared for discharge after treatment of a hypertensive crisis. What is the most appropriate vaccine for this patient?
disease vaccination non-hodgkin_lymphoma -
This patient has received pneumococcal and influenza vaccines one year ago. She is currently receiving her first course of chemotherapy.
disease vaccination chemotherapy -
clinical_decision vaccination cdc
-
Influenza is a respiratory viral illness that can lead to complications such as pneumonia and higher risks if not vaccinated in immunocompromised patients.
disease influenza clinical_decision -
disease symptoms influenza
-
The best option for this patient is to receive the influenza vaccine over the other vaccines listed.
clinical_decision vaccination influenza -
The measles-mumps-rubella vaccine is contraindicated in severely immunocompromised patients due to the risk of viral reactivation.
clinical_decision vaccination immunocompromised -
Meningococcal vaccine is safe for immunocompromised patients but boosters are not routinely necessary.
clinical_decision vaccination immunocompromised -
The pneumococcal vaccine is indicated for adults over 65 years and for patients with high-risk conditions.
clinical_decision vaccination pneumococcal -
Annual vaccination for influenza virus should be administered especially to patients like this one who are immunocompromised.
clinical_decision vaccination immunocompromised -
The primary viral illness discussed is influenza, which can lead to complications such as pneumonia and bacterial superinfection in vulnerable patients.
disease influenza respiratory -
Key symptoms of influenza include fever, chills, myalgias, malaise, headaches, cough, nausea, and vomiting.
disease influenza symptoms -
The Centers for Disease Control (CDC) advises annual vaccination against influenza starting at age greater than 6 months.
vaccination influenza cdc -
The influenza vaccine can be given as a trivalent or quadrivalent intramuscular injection of inactivated virus or as a nasal spray of live attenuated virus.
vaccination influenza types -
Inactivated influenza vaccine is safe for administration to immunocompromised patients who are at risk for severe illness.
vaccination immunocompromised influenza -
Influenza is characterized as a seasonal illness affecting patients primarily in winter and early spring.
disease influenza seasonality -
Patients who are immunocompromised should receive annual vaccination against influenza to prevent complications.
vaccination immunocompromised clinical_decision -
The measles-mumps-rubella vaccine is a live attenuated vaccine not recommended for severely immunocompromised patients due to reactivation risk.
vaccination immunocompromised measles -
The meningococcal vaccine is a conjugate vaccine indicated for all children and can be safely administered to immunocompromised patients.
vaccination meningococcal children -
The pneumococcal vaccine is indicated for adults over 65 years of age and for those with high-risk conditions.
vaccination pneumococcal adults -
vaccination pneumococcal booster
-
The varicella vaccine is a live attenuated vaccine administered in two doses, typically during childhood.
vaccination varicella childhood -
The zoster vaccine is recommended for adults over 60 years to prevent shingles and is also a live attenuated vaccine.
vaccination zoster shingles -
vaccination immunocompromised zoster
-
For immunocompromised patients, administering the inactivated influenza virus vaccine can prevent severe illness and complications.
vaccination immunocompromised influenza -
The most appropriate next step in diagnosis for a woman with high-risk sexual behavior and recurrent episodes of vaginal candidiasis and genital herpes is HIV testing.
diagnosis hiv women's_health -
A 27-year-old woman presents with vaginal discharge and itching. Her previous medical history includes three episodes of candidal vaginitis and three episodes of genital herpes.
clinical_scenario vaginal_discharge candidiasis herpes -
Recurrent episodes of vaginal candidiasis and genital herpes suggest the potential for underlying immunodeficiency that may occur with advanced HIV infection.
immunodeficiency hiv sexual_health -
Routine one-time screening for HIV is recommended for most sexually active individuals over the age of 13 years.
screening hiv public_health -
testing hiv diagnosis
-
If the fourth-generation HIV test is positive, further antibody testing to differentiate between infection with HIV-1 or HIV-2 is indicated.
hiv testing serology -
The gold standard for diagnosing genital herpes is viral culture, although PCR-based tests are preferred due to higher sensitivity.
herpes testing diagnosis -
The diagnosis of vaginal candidiasis can be made clinically without the use of fungal culture as yeast forms can be seen on microscopy.
candidiasis clinical_diagnosis lab_testing -
Possible underlying immunodeficiency in sexually active individuals with recurrent genital infections includes a risk for HIV infection.
immunodeficiency risk_factors sexual_health -
Patients engaging in high-risk sexual behaviors should be tested for HIV more frequently than those with lower risk.
screening hiv sexual_health -
Highly active antiretroviral therapy (HAART) should be initiated immediately upon a positive HIV test result.
treatment hiv haart -
Pelvic examination reveals a white vaginal discharge with a cottage-cheese consistency, characteristic of candidal vaginitis.
vaginal_discharge candidiasis clinical_findings -
A woman presents with a vaginal discharge and has had multiple partners, indicating a risk for sexually transmitted infections.
sexual_health stis risk_assessment -
For patients with high-risk sexual behavior and recurrent episodes of vaginal candidiasis, the most appropriate diagnostic step is to perform HIV testing.
diagnosis hiv -
diagnosis hiv
-
Populations at higher risk for HIV include individuals with numerous sexual partners and those who exchange sex for money.
risk_factors hiv -
Co-existing conditions like recurrent vaginal candidiasis may suggest underlying immunodeficiency associated with advanced HIV infection.
clinical_decision hiv -
HIV testing typically involves using a fourth-generation combined HIV 1/2 antigen and antibody test.
diagnosis hiv -
If the fourth-generation HIV test is positive, further antibody testing is indicated to distinguish between HIV-1 and HIV-2 infections.
diagnosis hiv -
In cases where the fourth-generation test is positive but antibody testing yields negative or indeterminate results, it is crucial to measure the HIV viral load.
diagnosis hiv -
treatment hiv
-
Fungal culture is unnecessary for diagnosing vaginal candidiasis since yeast forms can be identified through microscopy of vaginal secretions.
diagnosis vaginal_candidiasis -
Genital herpes infection can typically be diagnosed clinically, but laboratory confirmation is necessary during the first episode.
diagnosis genital_herpes -
While testing for HPV is important, the preferred screening method is cervical cytology or cervical cytology plus a PCR-based assay.
diagnosis hpv -
Colposcopy is indicated in patients only if their pap smear reveals abnormal findings such as cervical dysplasia.
diagnosis colposcopy -
HIV testing is especially advised for sexually active patients displaying symptoms like recurrent vaginal infections.
clinical_decision hiv -
A patient with recurrent infections may indicate a state of immunodeficiency that could be a hallmark of HIV infection.
clinical_decision hiv -
After starting dicloxacillin for cellulitis, a 37-year-old woman developed symptoms leading to suspicion of anaphylaxis.
clinical_scenario anaphylaxis -
Symptoms of {anaphylaxis} include pruritic rash, dyspnea, and wheezing after exposure to an allergen like dicloxacillin.
symptoms anaphylaxis -
The patient's vital signs show hypotension at 86/64 mm Hg and oxygen saturation of 92% on room air, indicating severe complications.
vital_signs anaphylaxis -
Immediate treatment for anaphylaxis includes administration of epinephrine to reverse the IgE-mediated mast cell degranulation.
treatment anaphylaxis -
In anaphylaxis, adjunctive treatments may include inhaled ẞ-agonists, glucocorticoids, and antihistamines.
treatment anaphylaxis -
Patients with suspected anaphylaxis should leave with an epinephrine autoinjector and instructions on usage, reinforcing the urgency of response.
post-treatment anaphylaxis -
Incorrect choices for immediate treatment in this anaphylactic case are Loratadine, Prednisone, and Stanozolol.
incorrect_treatments anaphylaxis -
The defining feature of anaphylaxis is the rapid onset of symptoms due to IgE-mediated reactions, leading to potential circulatory collapse.
definition anaphylaxis -
risks anaphylaxis
-
In managing anaphylaxis, signs such as angioedema and bronchospasm can indicate the seriousness of the condition.
symptoms anaphylaxis -
Histaminergic responses in anaphylaxis involve multiple organ systems resulting in vasodilation and airway obstruction.
physiology anaphylaxis -
In cases of anaphylaxis, administration of epinephrine is the most appropriate immediate step in management.
emergency anaphylaxis -
Anaphylaxis is a type 1 hypersensitivity reaction characterized by IgE-mediated mast cell degranulation.
immunology anaphylaxis -
symptoms anaphylaxis
-
risk anaphylaxis
-
diagnosis anaphylaxis
-
Adjunctive medications in the management of anaphylaxis include inhaled ẞ-adrenergic agonists, glucocorticoids, and histamine blockers.
medications anaphylaxis -
If medications are suspected to cause anaphylaxis, an allergy warning should be placed in the patient's chart.
management anaphylaxis -
discharge anaphylaxis
-
Patients should be educated about their allergy and advised to avoid antibiotics within the same class in the future.
education anaphylaxis -
medication anaphylaxis
-
Prednisone is frequently given in anaphylaxis but has little immediate effect on the disease process.
medication anaphylaxis -
medication anaphylaxis
-
Anaphylaxis should be suspected in patients with acute onset of dyspnea and evidence of distributive shock.
diagnosis anaphylaxis -
Additional interventions for anaphylaxis should focus on maintaining adequate blood pressure and ensuring patency of the airway.
interventions anaphylaxis -
In the management of anaphylaxis, correct dosage of epinephrine is essential for rapid improvement in symptoms.
management anaphylaxis -
If a patient presents with symptoms of anaphylaxis, the first line treatment is adminstration of intramuscular epinephrine.
emergency treatment -
education anaphylaxis
-
It is important to differentiate between allergic reactions and other causes of dyspnea during anaphylaxis diagnosis.
diagnosis anaphylaxis -
intervention anaphylaxis
-
management anaphylaxis
-
Immediate treatment of anaphylaxis can prevent complications such as hypoxia and distributive shock.
emergency anaphylaxis -
symptoms anaphylaxis
-
Anaphylaxis can occur after exposure to allergens such as antibiotics, bee stings, or certain foods.
triggers anaphylaxis -
A clinical scenario may include a febrile neonate under 28 days leading to investigations for potential infections.
clinical_scenario neonate -
pain sickle_cell
-
The clinical scenario involves a 47-year-old man who presents with a 3-month history of progressively worsening fatigue and a weight loss of 14-kg. What is the most likely confirmatory test for the diagnosis of chronic myelogenous leukemia (CML)?
clinical_scenario cml diagnosis -
The presence of which fusion protein is most likely to confirm the diagnosis of chronic myelogenous leukemia (CML)? BCR/ABL fusion protein.
cml diagnosis bcr/abl -
Chronic myelogenous leukemia (CML) is characterized by a translocation between chromosomes 9 and 22.
cml translocation -
The BCR/ABL fusion protein is associated with the Philadelphia (Ph) chromosome and results in activation of ABL kinase protein, leading to increased hematopoietic proliferation.
cml bcr/abl protein_activation -
Typical laboratory findings in chronic myelogenous leukemia (CML) include leukocytosis with an increase in nearly all cell lines, including basophilia and eosinophilia.
cml lab_findings -
The treatment for chronic myelogenous leukemia (CML) primarily involves the use of tyrosine kinase inhibitors such as imatinib or dasatinib.
cml treatment -
In CML, leukostasis is uncommon but can occur; it leads to end organ damage from occlusion of capillaries by malignant cells.
cml leukostasis -
brca1 cancer
-
P-glycoprotein functions as an efflux pump that can lead to chemotherapy resistance in leukemic cells.
p-glycoprotein resistance -
The presence of p53 suppressor gene is not a confirmatory marker for chronic myelogenous leukemia (CML), but serves as a tumor suppressor.
p53 tumor_suppressor -
A characteristic feature of acute leukemias, which can be distinguished from chronic myelogenous leukemia (CML), is the presence of circulating blasts in the blood.
acute_leukemia cml -
The diagnosis of chronic myelogenous leukemia (CML) is confirmed by the presence of the BCR/ABL fusion protein resulting from the Philadelphia (Ph) chromosome.
cml diagnosis oncology -
genetics cml
-
Activation of the ABL kinase protein leads to activation of the JAK/STAT and Ras/MAPK/ERK pathways, promoting unregulated cellular proliferation in CML.
cml pathophysiology cell_signaling -
Typical laboratory findings in CML include leukocytosis, with an increase in nearly all cell lines, and characteristic basophilia and eosinophilia.
cml laboratory_findings -
Leukostasis, a condition that can arise in CML, is due to the occlusion of capillaries by malignant cells.
cml complications -
cml treatment medication
-
The BRCA1 oncogene is involved in breast and ovarian cancer and is classified as a tumor suppressor gene.
oncogenes cancer -
Mutations in the BRCA1 gene lead to an increased risk for breast cancer due to its role in DNA repair.
oncogenes breast_cancer -
P-glycoprotein is an efflux pump that can render leukemic cells resistant to chemotherapy by transporting agents out of the cell.
cml drug_resistance -
The p53 tumor suppressor gene is mutated in nearly half of all cancers, but its loss of function does not confirm the diagnosis of CML.
cml tumor_suppressor -
aml cml
-
acute_leukemia diagnosis
-
A 42-year-old woman with paraplegia and recurrent urinary tract infections presents with decreased hemoglobin concentration due to cytokine-induced erythropoietin deficiency. What type of anemia is she likely experiencing?
anemia clinical_scenario -
Chronic inflammation in this patient leads to an increase in hepcidin production, decreasing responsiveness of the bone marrow to erythropoietin. What condition does this represent?
anemia chronic_disease pathophysiology -
Impaired iron absorption due to cytokine-induced erythropoietin deficiency leads to functional iron deficiency despite adequate {c1::iron stores}}. What does this result in?
anemia iron pathophysiology -
The laboratory findings in this patient with anemia due to chronic disease include normal to slightly increased ferritin concentration, decreased serum iron concentration, and decreased total iron-binding capacity (TIBC). What does each indicate?
anemia laboratory_findings -
To manage anemia of chronic disease effectively, treatment must focus on addressing the underlying disease. What is a common contributing factor to this condition?
anemia management clinical_decision -
Cytokine-induced erythropoietin deficiency contributes to a state of functional iron deficiency due to retained iron within the reticuloendothelial system. How does this affect erythropoiesis?
anemia iron_metabolism -
In the context of anemia, what does the acronym ACD stand for? Anemia of Chronic Disease. Which cytokines are involved in this process?
anemia chronic_disease -
Laboratory results show the following values for the patient: Hemoglobin: 8.7 g/dL, Mean corpuscular volume: 90 μm³. What condition might these results suggest? Normocytic anemia.
anemia laboratory_findings -
Given the patient has no abnormalities other than paraplegia and a history of urinary tract infections, what is the most plausible diagnosis contributing to her anemia? Chronic Disease.
anemia diagnosis -
What is one of the key inflammatory substances that leads to increased hepcidin production? Tumor necrosis factor-a. What role does it play in anemia?
anemia inflammation -
This patient’s normocytic anemia can be classified as ACD, which is common in patients with chronic infections. Can you name other conditions associated with this?
anemia chronic_disease -
Deficiencies such as folic acid or iron can present with similar symptoms to anemia of chronic disease, but what distinguishes ACD is the increased hepcidin levels affecting iron metabolism.
anemia distinction -
Chronic inflammation reduces erythropoiesis primarily by decreasing the bone marrow's response to erythropoietin through enhanced production of inflammatory cytokines. Name two specific examples.
anemia pathophysiology -
Cytokine-induced erythropoietin deficiency is the most likely cause of this patient's normocytic anemia, which is commonly referred to as anemia of chronic disease (ACD). ACD is common in patients with rheumatologic disorders, renal disease, malignancies, and chronic infections.
anemia chronic_disease cytokines -
Chronic inflammation leads to an increase in hepcidin production, which causes a decreased responsiveness of the bone marrow to erythropoietin and retention of iron within the reticuloendothelial system (RES).
inflammation iron_metabolism hepcidin -
In ACD, iron is retained within the RES and cannot be effectively accessed for erythropoiesis, resulting in either normocytic or microcytic anemia and a reduced number of reticulocytes.
anemia erythropoiesis hematology -
Laboratory findings in ACD typically show a normal to slightly increased ferritin concentration, decreased serum iron concentration, and decreased total iron-binding capacity (TIBC).
laboratory_findings ferritin iron_studies -
Treatment for ACD must focus on treating the underlying disease to decrease inflammation which is critical for managing this condition.
treatment chronic_disease inflammation -
Folic acid deficiency is relatively uncommon but may lead to macrocytic anemia in patients with alcohol use disorder or other nutritional deficiencies. This patient exhibits no risk factors for folate deficiency.
anemia folate nutrition -
Glucose 6-phosphate dehydrogenase deficiency can lead to hemolysis under oxidative stress, presenting with anemia and increased indirect bilirubin, lactate dehydrogenase, and hemoglobinuria.
hemolysis g6pd bilirubin -
Iron deficiency anemia presents similarly to ACD but can be distinguished by iron studies showing decreased ferritin concentration and decreased iron saturation.
anemia iron_deficiency differential_diagnosis -
Myelodysplasia describes a genetically diverse set of disorders affecting multipotent stem cells of the bone marrow, possibly leading to anemia, neutropenia, or thrombocytopenia.
myelodysplasia bone_marrow hematology -
Educational objectives emphasize that ACD is common in patients with rheumatologic diseases, renal disease, and those with chronic or frequent infections.
education chronic_disease infection -
A 32-year-old African American man with iron deficiency anemia comes for a follow-up examination. Which of the following is the most likely diagnosis? A) Celiac disease, B) Myelodysplastic syndrome, C) Occult gastrointestinal bleeding, D) Pure red cell aplasia, E) Thalassemia.
clinical_scenario anemia diagnosis -
The lab findings of this 32-year-old African American man with iron deficiency anemia include a hemoglobin of 10.9 g/dL and a hematocrit of 33% today, indicating mild microcytic anemia.
lab_findings anemia iron_deficiency -
In patients with thalassemia, the red cell distribution width (RDW) is typically normal. This differs from other causes of anemia like iron deficiency.
thalassemia anemia lab_values -
Mild microcytic anemia with a normal RDW and normal iron studies suggests the diagnosis of thalassemia.
diagnosis anemia thalassemia -
The serum iron level for this patient was 60 µg/dL with a transferrin saturation of 25%. This supports the diagnosis of thalassemia over iron deficiency anemia.
serum_iron transferrin_saturation thalassemia -
The patient is a 32-year-old African American man with a history of smoking and moderate alcohol consumption, presenting with iron deficiency anemia.
demographics anemia risk_factors -
blood_smear thalassemia anemia
-
The hemoglobin levels have increased from 10.7 g/dL six months ago to 10.9 g/dL today, suggesting response to treatment for iron deficiency anemia.
hemoglobin treatment response -
The most likely diagnosis in a 32-year-old African American patient with mild microcytic anemia and normal RDW who hasn't responded to iron therapy is thalassemia.
diagnosis thalassemia -
Thalassemia interferes with normal synthesis of hemoglobin A (HbA) due to nonfunctional alleles of the α- or β-globin genes.
disease hemoglobin genetics -
hemoglobin anatomy
-
Patients with β-thalassemia have deficient β-globin genes, leading to ineffective assembly of normal HbA and formation of insoluble tetramers.
disease thalassemia -
genetics thalassemia
-
Microcytosis and target cells on peripheral blood smear are characteristic of both α- and β-thalassemia.
diagnosis blood -
diagnosis anemia
-
Oral iron therapy will have no effect on hemoglobin concentrations in patients with thalassemia trait.
treatment thalassemia -
lab_findings anemia
-
Celiac disease can lead to iron deficiency presenting with microcytic anemia, increased RDW, and transferrin saturation below 20%.
diagnosis celiac_disease -
Myelodysplastic syndrome often presents with cytopenias, but microcytic anemia in isolation would be atypical.
diagnosis myelodysplastic_syndrome -
Occult gastrointestinal bleeding leads to iron deficiency anemia that should respond to oral iron therapy.
diagnosis anemia -
Additional findings for celiac disease may include weight loss, diarrhea, or other gastrointestinal symptoms.
symptoms celiac_disease -
diagnosis thalassemia
-
Combination therapy with folate and iron may be necessary due to normal iron studies in patients with thalassemia.
treatment thalassemia -
diagnosis lab_findings
-
The correct answer in the multiple-choice scenario of a patient with anemia and unresponsive to iron therapy is Thalassemia (E).
diagnosis multiple_choice -
In an African American patient with mild microcytic anemia, thalassemia is most likely when hemoglobin concentrations are normal despite several months of iron therapy and the red cell distribution width (RDW) is also normal, indicating that thalassemia is an inherited condition affecting the globin genes.
thalassemia anemia diagnosis -
Normal adult hemoglobin A (HbA) consists of two alpha-globin subunits and two beta-globin subunits, which together form a unique conformation that has a high affinity for oxygen.
hemoglobin structure -
Deficient beta-globin genes in β-thalassemia prevent effective assembly of HbA, causing excess alpha-globin chains to form insoluble tetramers.
beta-thalassemia hemoglobin -
Patients with a-thalassemia trait can be asymptomatic but commonly present with microcytosis and may have a minimal decrease in hemoglobin concentration.
a-thalassemia symptoms -
Microcytosis and target cells on a peripheral blood smear characterize both a-thalassemia and beta-thalassemia.
microcytosis thalassemia -
To distinguish between thalassemia and iron deficiency anemia, hemoglobin electrophoresis is used, as patients with thalassemia often present with normal iron studies.
diagnosis iron_deficiency -
In patients diagnosed with thalassemia minor, oral iron therapy does not affect hemoglobin concentrations because they typically do not have iron deficiency.
treatment iron_therapy -
A transferrin saturation of 18 to 20% is often used to exclude iron deficiency anemia in patients presenting with mild microcytic anemia.
transferrin_saturation diagnosis -
Celiac disease can lead to iron deficiency anemia, presenting with microcytic anemia and an increased RDW alongside expected findings of weight loss and diarrhea.
celiac_disease anemia -
Myelodysplastic syndrome may present with diverse cytopenias but microcytic anemia in isolation is atypical.
myelodysplastic_syndrome diagnosis -
Occult gastrointestinal bleeding typically leads to iron deficiency anemia that should respond to oral iron therapy, which does not occur in thalassemia.
occult_bleeding iron_therapy -
Pure red blood cell aplasia results in complete destruction of erythrocyte precursors in the bone marrow leading to profound anemia.
erythrocyte anemia -
Normal human hemoglobin A consists of two alpha-globin and two beta-globin subunits, and mutations in these alleles lead to thalassemia variants.
hemoglobin mutations -
In the case of thalassemia trait or thalassemia minor, patients present with mild microcytic anemia and normal iron studies.
thalassemia symptoms -
Peripheral blood smear findings for thalassemia may show target cells indicating thalassemia presence in relevant patients.
blood_smear diagnosis -
The severity of anemia in thalassemia is dependent on the number and nature of mutations present within the globin genes.
severity anemia -
Patients with thalassemia who have multiple nonfunctional alleles may present with increasingly severe levels of anemia.
anemia severity -
In managing a patient with sickle cell disease experiencing an acute painful episode, the most appropriate next step in pharmacotherapy is intravenous morphine.
sickle_cell_disease pain_management clinical_decision -
A 23-year-old man with sickle cell disease presents with severe low back pain rated at 8 out of 10. His hemoglobin concentration is 7.2 g/dL.
sickle_cell_disease clinical_scenario -
Patients with sickle cell disease often experience vaso-occlusive phenomena, which can lead to acute painful episodes referred to as pain crises.
sickle_cell_disease pain_management -
For acute painful crises in patients with sickle cell disease, the preferred route of administration for analgesics is parenteral.
sickle_cell_disease pain_management -
Oral medications such as oral celecoxib and oral oxycodone are generally ineffective for managing acute pain crises in patients with sickle cell disease.
sickle_cell_disease pain_management -
In the case of a patient with acute pain crises due to sickle cell disease, it is crucial to prioritize the administration of analgesia over further diagnostics.
sickle_cell_disease clinical_decision -
A 23-year-old man with sickle cell disease experiences nausea and decreased intake of solids and liquids. This can complicate treatment by requiring a switch to parenteral routes for medication delivery.
sickle_cell_disease clinical_scenario -
Rapid assessment is critical in patients with sickle cell disease to rule out concomitant disorders like acute chest syndrome and myocardial infarction.
sickle_cell_disease diagnosis -
Chronic exposure to opiates in patients with sickle cell disease often results in the need for higher doses of opiate medication compared to opiate-naive patients.
sickle_cell_disease pain_management -
The lab findings for a 23-year-old man with sickle cell disease show hemoglobin at 7.2 g/dL and creatinine at 2.6 mg/dL.
sickle_cell_disease lab_findings -
Vaso-occlusive events in patients with sickle cell disease can manifest as pain in areas such as the back, abdomen, or long bones.
sickle_cell_disease pain_management -
Patients in pain crises due to sickle cell disease may present with additional symptoms including pale conjunctivae.
sickle_cell_disease clinical_scenario -
Among the medications considered for treatment, the most appropriate for acute pain in sickle cell disease is intravenous morphine over oral pills or lesser opioids.
sickle_cell_disease pain_management -
If a patient experiences hypovolemia during a painful episode of sickle cell disease, the healthcare provider must also prioritize fluid resuscitation.
sickle_cell_disease clinical_decision -
In treating acute pain crises in patients with sickle cell disease, intravenous morphine is preferred as it provides a faster onset of pain relief.
sickle_cell_disease pain_management -
Administering adequate analgesia for painful crises in patients with sickle cell disease is crucial and should not be delayed for diagnostics involving acute chest syndrome.
sickle_cell_disease pain_management -
In the management of sickle cell disease pain episodes, intravenous morphine is considered the first-line medication to manage acute pain.
sickle_cell_disease pain_management -
In patients with sickle cell disease, acute painful episodes often referred to as pain crises, occur due to vaso-occlusive phenomena.
sickle_cell_disease pain_management acute_pain -
The most appropriate medication for patients experiencing an acute painful episode due to sickle cell disease is intravenous morphine.
sickle_cell_disease medication pain_management -
Assessment for accompanying disorders such as acute chest syndrome, myocardial infarction, and infection is critical during pain crises in patients with sickle cell disease.
sickle_cell_disease diagnosis acute_pain -
Intravenous administration is preferred for analgesia in acute painful crises of sickle cell disease because oral medications may not provide adequate relief due to low oral tolerance.
sickle_cell_disease pain_management medication -
Rapid administration of analgesia is crucial for managing pain crises in patients with sickle cell disease, often guided by an individualized pain pathway.
sickle_cell_disease pain_management analgesia -
Chronic exposure to opiates in patients with sickle cell disease commonly leads to a need for higher opiate doses compared to opiate-naive patients.
sickle_cell_disease pain_management opioids -
Patients with sickle cell disease may experience pain in various areas, including the hands, feet, abdomen, and long bones.
sickle_cell_disease pain_management symptoms -
For acute painful episodes, the preferred treatment involves intravenous opiates rather than oral medications such as celecoxib or oxycodone.
sickle_cell_disease treatment pain_management -
Intravenous meperidine is rarely recommended for acute pain in sickle cell disease due to its challenging pharmacodynamics and kinetics.
sickle_cell_disease medication pain_management -
Proper treatment of pain crises in patients with sickle cell disease prioritizes reversing features like hypoxia and hypovolemia.
sickle_cell_disease treatment acute_pain -
Acute painful crises in patients with sickle cell disease necessitate simultaneous assessment for conditions such as acute chest syndrome during pain management.
sickle_cell_disease acute_pain diagnosis -
The patient in this clinical scenario is a 72-year-old man with a history of poorly controlled hypertension. His current blood pressure is 150/105 mm Hg. What is the greatest risk factor for cerebral infarction in this patient? A) Abnormal serum lipid concentrations B) Family history of cerebral infarction C) Hypertension D) Increase in serum glucose concentration E) Smoking history
hypertension cerebral_infarction stroke cardiology -
Hypertension is considered the greatest modifiable risk factor for cerebral infarction. Uncontrolled hypertension increases the risk for ischemic stroke by approximately two-fold. These risks remain even when hypertension is well-controlled.
hypertension risk_factors ischemic_stroke -
In stroke prevention, initiating antihypertensive therapy is crucial. Additional lifestyle modifications include weight loss, dietary changes, smoking cessation, and regular exercise.
stroke_prevention lifestyle_modifications -
Abnormal serum lipid concentrations are not consistently considered a risk factor for all stroke subtypes. However, they may play a modest role in the development of ischemic strokes in large vessel or lacunar distributions.
serum_lipids stroke_subtypes -
A family history of cerebral infarction is considered an important, non-modifiable risk factor but is not as significant as hypertension. It has not been consistently demonstrated as a risk factor in large studies.
family_history stroke_risk -
An increase in serum glucose concentration, particularly in the context of diabetes mellitus, is a significant risk factor for ischemic stroke but is not as impactful as hypertension.
glucose_levels stroke_risk -
The greatest modifiable risk factor for cerebral infarction is Hypertension. It contributes significantly to the development of cardiac and renal failure and atherosclerotic disease.
medicine hypertension cerebral_infarction -
Uncontrolled hypertension is associated with an approximately two-fold increase in the risk for ischemic stroke.
medicine hypertension ischemic_stroke -
Even when hypertension is well-controlled, the risk for ischemic stroke remains incompletely eliminated.
medicine hypertension ischemic_stroke -
Initiation of antihypertensive therapy is an important component of stroke prevention, along with lifestyle modification such as weight loss and regular exercise.
medicine hypertension stroke_prevention -
Abnormal serum lipid concentrations may play a modest role in the development of ischemic strokes, especially in large vessel or lacunar distributions.
medicine lipids ischemic_stroke -
Family history of cerebral infarction is considered an important non-modifiable risk factor but is not as significant as hypertension in stroke risk.
medicine family_history cerebral_infarction -
Increase in serum glucose concentration, especially in the setting of diabetes mellitus, is a notable risk factor for ischemic stroke, but less significant than hypertension.
medicine glucose ischemic_stroke -
medicine smoking ischemic_stroke
-
The educational objective is that hypertension is the single most important modifiable risk factor for cerebral infarction.
medicine risk_factors cerebral_infarction -
Uncontrolled hypertension increases the risk for ischemic stroke, contributing significantly to stroke pathophysiology and requiring comprehensive management.
medicine management hypertension -
C) Hypertension is the correct answer for the greatest modifiable risk factor for cerebral infarction.
medicine exam_question hypertension -
A clinical scenario presents a 77-year-old woman with severe degenerative arthritis who has a 2-week history of ringing and pain in her ears. Which of the following laboratory findings is most likely in this patient? Na+: 132, K+: 4.6, Cl-: 94, HCO3-: 18, pH: 7.38.
clinical_scenario lab_values salicylate_toxicity -
Salicylate poisoning primarily affects the body by causing respiratory alkalosis due to stimulation of respiratory centers. This leads to hyperventilation and delayed anion-gap metabolic acidosis.
drug salicylate_toxicity physiology -
In cases of acute salicylate toxicity, patients typically present with symptoms such as hyperventilation, gastrointestinal upset, and tinnitus. Other symptoms may include agitation and delirium.
clinical_scenario symptoms salicylate_toxicity -
Management of acute or chronic salicylate toxicity generally involves systemic alkalinization using a sodium bicarbonate infusion. In severe cases, patients may require dialysis.
clinical_decision management salicylate_toxicity -
Mild salicylate toxicity is characterized by an increased anion gap and a compensated metabolic acidosis.
clinical_finding metabolic_acidosis salicylate_toxicity -
Aspirin irreversibly inactivates cyclooxygenase, preventing the conversion of arachidonic acid to thromboxane A2, which reduces platelet activation.
drug mechanism aspirin -
Salicylate toxicity would not typically cause hyponatremia, hyperkalemia, or hypokalemia. Specifically, hyperkalemia may occur due to renal insufficiency or aldosterone deficiency.
lab_values salicylate_toxicity electrolytes -
Key features of patients with chronic salicylate ingestion can include symptoms similar to acute toxicity or mild symptoms such as tinnitus, nausea, and diaphoresis.
clinical_scenario symptoms salicylate_toxicity -
Anion gap metabolic acidosis is secondary to the production of lactate and ketoacids in salicylate toxicity.
physiology metabolic_acidosis salicylate_toxicity -
Salicylate toxicity can present with defining features such as hyperventilation, gastrointestinal upset, hyperthermia, tinnitus, agitation, delirium, and hallucinations.
salicylate_toxicity symptoms clinical_features -
Aspirin irreversibly inactivates cyclooxygenase, which prevents the conversion of arachidonic acid to thromboxane A2.
aspirin mechanism pharmacology -
In high doses, salicylate poisoning leads to early respiratory alkalosis followed by a delayed anion-gap metabolic acidosis due to decoupling effects on the electron transport chain.
salicylate_toxicity acidosis respiratory_alcalosis -
Management of acute or chronic salicylate toxicity includes systemic alkalinization with sodium bicarbonate infusion.
salicylate_toxicity treatment clinical_management -
salicylate_toxicity metabolic_acidosis anion_gap
-
Patients with chronic salicylate ingestion may present identical symptoms to acute toxicity, or with mild symptoms such as tinnitus, nausea, vomiting, or diaphoresis.
salicylate_toxicity chronic_exposure symptoms -
Salicylate toxicity typically does not result in changes in sodium or potassium serum concentrations in major ways, unlike conditions resulting in hyperkalemia or hyponatremia.
salicylate_toxicity electrolytes clinical_features -
Patients may need dialysis in cases of severe altered mental status, renal failure, pulmonary edema, or clinical deterioration.
salicylate_toxicity management severe_cases -
Incorrect answers to the multiple choice question about salicylate toxicity included: A) hyponatremia, B) hypokalemia, D) hyperkalemia.
salicylate_toxicity incorrect_answers clinical_decision -
A 23-year-old woman presents with a lesion on her lip that appeared 1 day ago. She also reports a tingling and burning sensation in that area for the past 4 days. Examination reveals a grouping of discrete, clear, fluid-filled vesicles measuring 5 mm in diameter. The most likely diagnosis is Herpes simplex.
diagnosis herpes -
Herpes simplex virus (HSV) infection commonly causes oral infections known as herpes labialis that begin with vesicle formation at the oral-labial margin.
disease herpes -
Prodromal symptoms of herpes simplex may include burning, tingling, itching, or pain in the area prior to vesicular lesions.
symptoms herpes -
Following initial infection, herpes simplex virus may remain latent in the trigeminal ganglion until reactivation occurs.
disease herpes -
Reactivation of herpes simplex can be triggered by factors such as stress, sunlight, or local trauma.
triggers herpes -
Diagnosis of herpes simplex is confirmed with viral culture or polymerase chain reaction testing from the base of the lesion if uncertain.
diagnosis herpes -
Antiviral agents that inhibit viral DNA polymerase, including acyclovir, valacyclovir, and famciclovir, are used in the treatment of herpes simplex.
treatment drugs herpes -
Chickenpox, or varicella zoster virus, does not present with localized vesicular lesions at the oral-labial margin, unlike herpes simplex.
disease chickenpox -
Erythema multiforme is characterized by targetoid lesions and may be triggered by drugs (especially antibiotics) or infections.
disease erythema -
Erythema nodosum is another condition differentiated from herpes simplex and is characterized by painful nodules on the lower extremities.
disease erythema -
The correct answer for a lesion on the lip with fluid-filled vesicles, tingling, and burning in a 23-year-old woman is Herpes simplex.
diagnosis herpes -
disease herpes labialis
-
disease herpes labialis
-
The vesicles in herpes labialis lyse and progress to shallow, painful ulcers with an erythematous border.
disease herpes ulcers -
disease herpes prodromal
-
disease herpes hsv
-
disease herpes latency
-
disease herpes triggers
-
The diagnosis of herpes labialis can be confirmed with a viral culture or a polymerase chain reaction test.
diagnosis herpes hsv -
drug herpes treatment
-
drug herpes antiviral
-
The duration of an outbreak of herpes labialis may be shortened by using antiviral agents such as acyclovir.
drug herpes treatment -
Unlike herpes simplex, chickenpox is caused by varicella-zoster virus (VZV), also known as human herpesvirus-3.
disease chickenpox vzv -
Reactivation of varicella-zoster virus can lead to shingles, characterized by multiple vesicular lesions in a unilateral, dermatomal distribution.
disease shingles vzv -
Erythema multiforme is characterized by targetoid lesions on the palms, soles, trunk, and oral mucosa.
disease erythema multiforme -
Erythema multiforme may be associated with conditions such as drugs, infections, or specific viruses (e.g., herpes simplex virus).
disease erythema triggers -
Erythema nodosum presents as painful, immobile nodules on the shins, and lesions are typically bilateral.
disease erythema nodosum -
The causes of erythema nodosum can include conditions like inflammatory bowel disease, sarcoidosis, or reactions to medications.
disease erythema causes -
Herpes labialis is also known to present with painful vesicles and punched-out erosions on the lip during reactivation.
diagnosis herpes labialis -
A 42-year-old man has a 3-month history of a progressive rash on his arms and back. The most likely diagnosis is Psoriasis.
diagnosis psoriasis -
The rash associated with psoriasis often presents with sharp, defined, erythematous plaques covered with white scale.
clinical_features psoriasis -
clinical_features psoriasis
-
Common treatments for psoriasis include: topical corticosteroids, topical Vitamin D analogs, and if refractory, consider phototherapy or biologics.
treatment psoriasis -
diagnosis psoriasis
-
diagnosis psoriasis
-
clinical_features psoriasis
-
symptoms psoriasis
-
An otherwise healthy individual presenting with a rash over 3 months could be indicative of conditions like Psoriasis, Atopic dermatitis, or Tinea corporis.
differential_diagnosis rash -
clinical_signs
-
clinical_signs
-
diagnosis rash
-
pathophysiology psoriasis
-
Psoriasis is a common inflammatory skin condition caused by immune dysregulation leading to keratinocyte proliferation.
disease psoriasis skin_condition -
disease psoriasis
-
disease psoriasis skin_condition
-
disease psoriasis symptoms
-
disease psoriasis diagnosis
-
disease psoriasis nail_changes
-
disease psoriasis treatment
-
If psoriasis is refractory to topical therapies, then phototherapy, methotrexate, or biologic medications may be considered.
disease psoriasis treatment -
Atopic dermatitis is commonly known as eczema and may be characterized by excoriated and lichenified lesions.
disease atopic_dermatitis -
Bullous pemphigoid is characterized by antibodies against the hemidesmosome and presents with tense bullae.
disease bullous_pemphigoid -
Dysplastic nevi are benign, acquired melanocytic lesions that may rarely transform into cutaneous melanoma.
disease dysplastic_nevi -
disease lichen_simplex_chronicus
-
disease pityriasis_rosea
-
disease pityriasis_rosea viral_infection
-
Incorrect choices for diagnosing psoriasis include A) Atopic dermatitis, B) Bullous pemphigoid, C) Dysplastic nevi, D) Lichen simplex chronicus, and E) Pityriasis rosea.
disease psoriasis incorrect_choices -
disease psoriasis images
Vaccination for Immunocompromised Patients
Case Summary
A 67-year-old woman with non-Hodgkin lymphoma post-chemotherapy requires vaccination post-discharge.
Recommended Vaccine
- Influenza Vaccine: Administer annually, especially in immunocompromised individuals to prevent severe illness.
- Administration: Can be given intramuscularly (inactivated) or as a nasal spray (live attenuated).
Incorrect Options
- Measles-mumps-rubella (MMR): Live vaccine contraindicated in severely immunocompromised patients.
- Meningococcal Vaccine: Indicated for certain populations but boosters not routinely necessary.
- Pneumococcal Vaccine: Not required since she received it last year.
- Varicella Vaccine: Live vaccine not safe for the immunocompromised.
Educational Objective
Immunocompromised patients should receive the influenza vaccine annually.
Diagnosis of Vaginal Discharge
Patient Profile
A 27-year-old woman presents with vaginal discharge, itchy for 1 week, and a history of recurrent candidal vaginitis.
Recommended Diagnosis Step
- HIV Testing: Critical due to high-risk sexual behavior and recurrent infections.
Incorrect Options
- Fungal Culture: Often not necessary; candidiasis can be diagnosed clinically.
- Herpes Culture: Verify only if lesions present; recurrent episodes usually don't require this.
- HPV Culture: Not first-line for current symptoms.
- Colposcopy: Only after abnormal Pap smear results.
Educational Objective
Screening for HIV is essential in high-risk populations to identify potential immunodeficiency.
Management of Anaphylaxis
Case Summary
A 37-year-old woman exhibits symptoms of anaphylaxis after dicloxacillin therapy.
Immediate Management
- Epinephrine Administration: First-line treatment for anaphylactic reactions to rapidly reverse symptoms.
Incorrect Options
- Loratadine: Antihistamine, not a first-line treatment.
- Prednisone: Usually adjunct, not immediate responders.
- Stanozolol: Not indicated for anaphylaxis management.
Educational Objective
Recognize anaphylaxis promptly and administer epinephrine immediately to prevent severe complications.
Diagnosis of Anemia
Patient Profile
A 42-year-old woman with recurrent UTIs has a low hemoglobin level.
Likely Diagnosis
- Cytokine-Induced Erythropoietin Deficiency: Indicates anemia of chronic disease (ACD), common in patients with chronic inflammation.
Incorrect Options
- Folic Acid Deficiency: Generally leads to macrocytic anemia, not observed here.
- G6PD Deficiency: Causes hemolytic anemia but not in this case.
- Iron Deficiency: Typically responds to iron therapy; this patient does not.
- Myelodysplasia: Uncommon in patients under 50 without other cell line abnormalities.
Educational Objective
Understanding anemia types helps direct appropriate testing/management strategies.
Diagnosing Thalassemia
Patient Profile
A 32-year-old African American man with microcytic anemia fails to improve with iron therapy.
Likely Diagnosis
- Thalassemia: Characterized by microcytic anemia, normal RDW, and unchanged iron studies.
Incorrect Options
- Celiac Disease: More indicative of iron deficiency.
- Myelodysplastic Syndrome: Usually presents with more diverse symptoms.
- Occult GI Bleeding: Would typically respond to iron supplementation.
- Pure Red Cell Aplasia: Rarely characterized solely by isolated anemia.
Educational Objective
Thalassemia may mimic iron deficiency but requires different management.
Acute Pain Management in Sickle Cell Disease
Patient Profile
A 23-year-old man with sickle cell disease presents with severe low back pain.
Recommended Treatment
- Intravenous Morphine: Optimal for immediate pain management in acute crises.
Incorrect Options
- Oral Medications: Insufficient for acute crises; IV route preferred for rapid relief.
- Intramuscular Ketorolac: Also inadequate for severe pain management.
- Intravenous Meperidine: Not preferred due to unpredictable effects.
Educational Objective
Immediate pain control is crucial in managing vaso-occlusive crises in sickle cell patients.
Risk Factors for Cerebral Infarction
Patient Profile
A 72-year-old man with a history of poorly controlled hypertension and other risk factors.
Greatest Risk Factor
- Hypertension: Major modifiable risk in stroke development.
Incorrect Options
- Serum Lipid Abnormalities: Less consistently linked to all stroke types.
- Family History: Important but not as significant as hypertension.
- Increased Serum Glucose: Relevant, but not as impactful as hypertension.
- Smoking History: Important but secondary to hypertension.
Educational Objective
Focus on controlling hypertension to mitigate stroke risk.
Laboratory Findings in Salicylate Toxicity
Patient Profile
A 77-year-old woman with degenerative arthritis develops pain in her ears after taking aspirin.
Expected Findings
- Compensated Metabolic Acidosis: Due to aspirin's effects on metabolism.
- Respiratory alkalosis followed by metabolic acidosis due to increased lactic acid.
Incorrect Options
- Hyponatremia or Takiness: Not typical findings in salicylate toxicity.
- K+ Levels: Likely unaffected directly.
Educational Objective
Understanding the metabolic changes in salicylate toxicity aids in effective management.
Herpes Simplex Diagnosis
Patient Profile
A 23-year-old woman presents with a lip lesion showing discrete vesicles.
Likely Diagnosis
- Herpes Simplex: Characteristic vesicular outbreak at the lip margin, often preceded by tingling.
Incorrect Options
- Chickenpox: Presents differently with generalized rash.
- Erythema Multiforme: Characterized by target lesions, not vesiculated lesions.
- Erythema Nodosum & Tinea Corporis: Not consistent with clinical findings.
Educational Objective
Recognizing oral herpes aids in timely antiviral therapy.
Identifying Psoriasis
Patient Profile
A 42-year-old man presents with an itchy rash over his arms and back.
Likely Diagnosis
- Psoriasis: Characterized by erythematous plaques with silver scales, commonly on extensor surfaces.
Incorrect Options
- Atopic Dermatitis: Typically occurs in flexural areas, not as described.
- Bullous Pemphigoid: Features tense bullae, not plaques.
- Dysplastic Nevi & Tinea Corporis: Not consistent with the presentation.
- Pityriasis Rosea: Typically follows a specific pattern after a herald patch.
Educational Objective
Recognizing the signs of psoriasis ensures appropriate topical treatments.