Sign up to unlock more features
- Save this deck to your account
- Study flashcards with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from PDFs and documents
- Better text extraction from your PDFs and documents
- Better flashcards with our more advanced AI model
What is the effect on voluntary movement in a lower motor neuron (LMN) lesion?
What are the effects on reflexes, muscle tone, and muscle bulk in an LMN lesion?
What are fasciculations and what causes them?
What are fibrillations and what causes them?
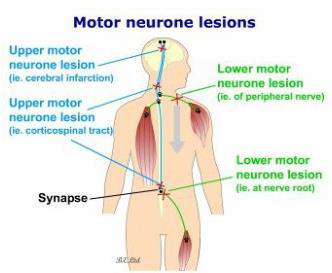
What is the typical pattern of paralysis after an upper motor neuron lesion above the medulla?
After 2 weeks following an upper motor neuron lesion, which improvements occur and what gait does the patient use? 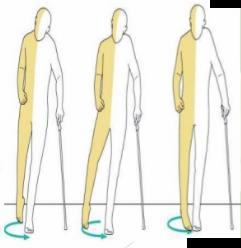
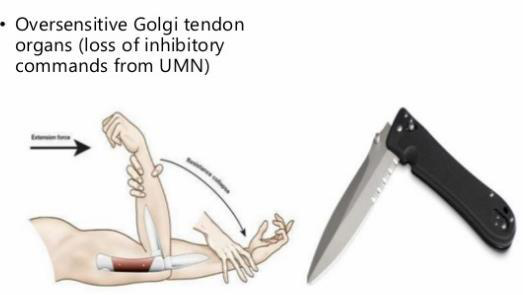
What characterizes clasp-knife spasticity in upper motor neuron lesions?
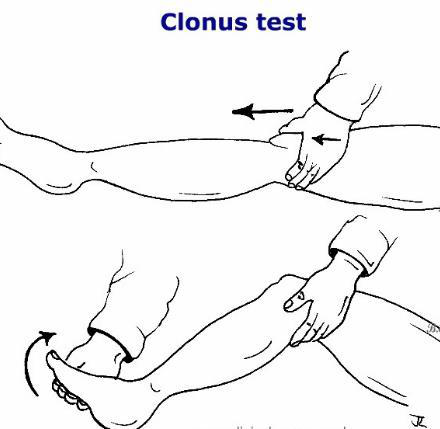
What is clonus and where is it commonly tested?
Why does an affected muscle show minimal (disuse) atrophy in an upper motor neuron lesion?
What are the key contrasting features of chronic UMNL versus LMNL regarding laterality, muscle tone, reflexes, clonus, and atrophy?
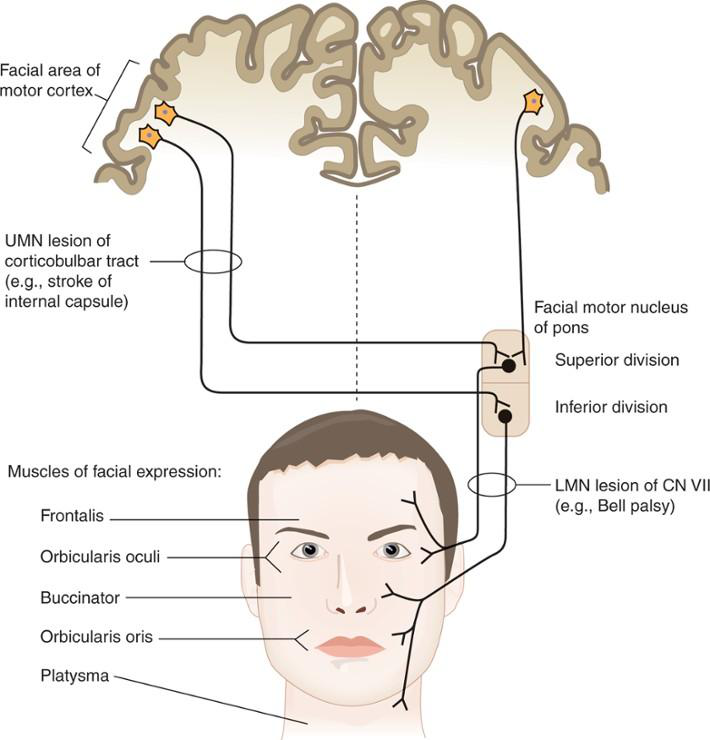
What are the facial findings in an upper motor neuron lesion of the corticobulbar tract?
What are the facial findings in a lower motor neuron facial nerve lesion (facial palsy)?
Examine the photograph: 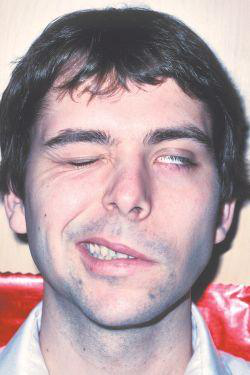
Which side shows facial paralysis and what are the visible signs?
Examine the photograph: 
Which side shows facial paralysis and what are the visible signs?
What is muscle tone and which muscles does it mainly affect?
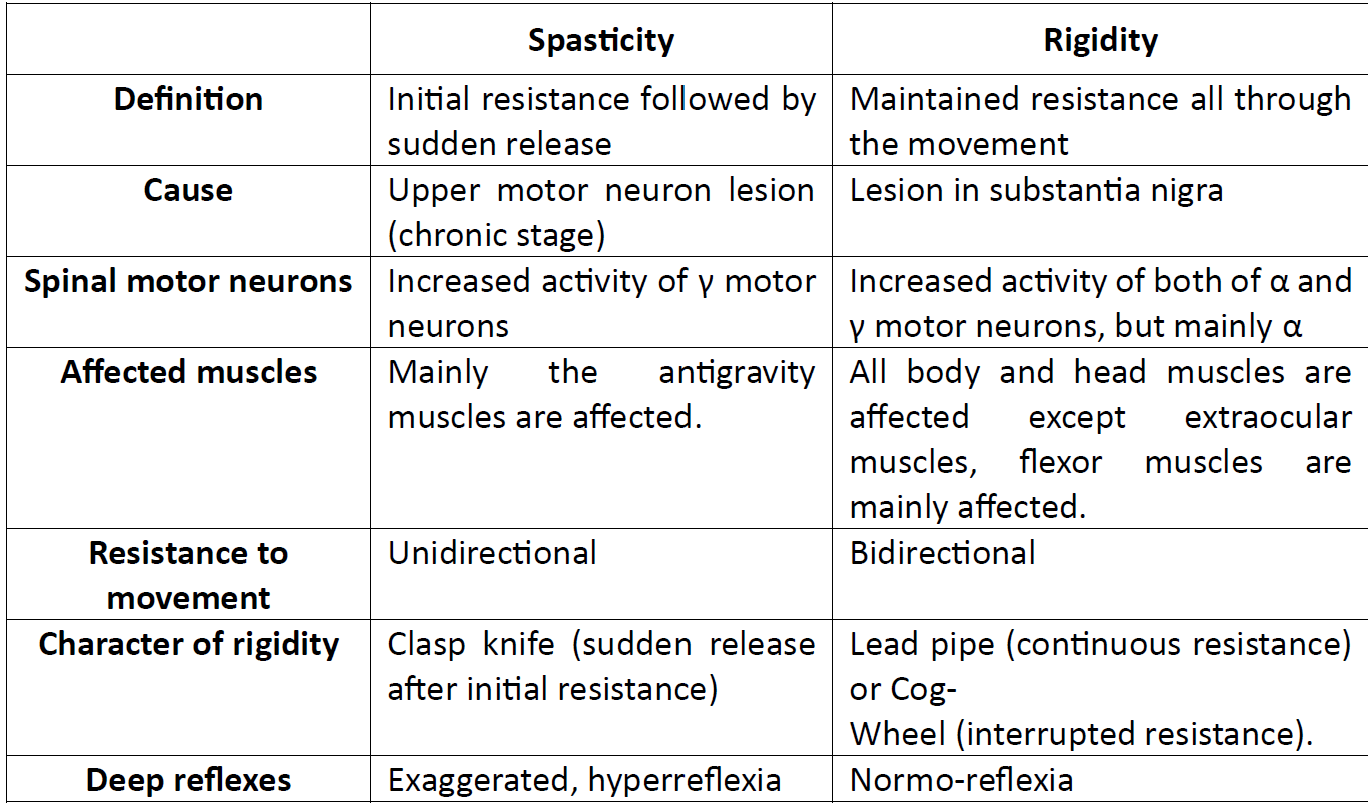
Name the two major types of hypertonia and one key clinical difference between them.
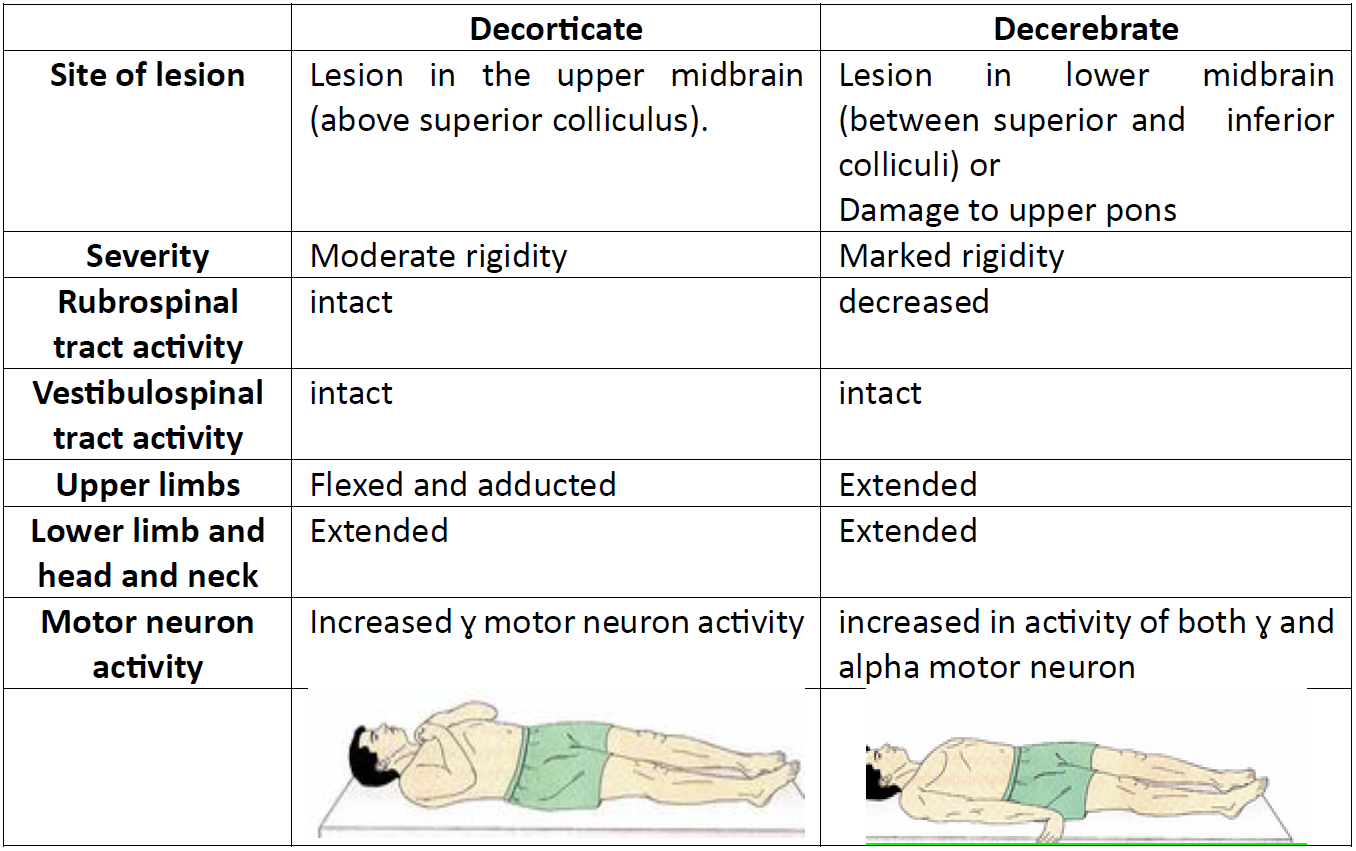
Compare the site of lesion and upper limb posture in decorticate versus decerebrate posturing.
List the main causes of hypotonia (flaccidity) from loss of excitatory supraspinal control of static muscle stretch reflex.
What is mononeuropathy and what are its main effects?
What is polyneuropathy and what are common acquired causes?
What are the sequential sensory changes in peripheral parts (hands and feet)?
What are the motor features of a lower motor neuron lesion (LMNL) in peripheral limbs?
What is syringomyelia and which spinal segments are commonly affected?
What are the characteristic sensory, motor, and autonomic effects of a central cord (syringomyelia) lesion?
What is Tabes Dorsalis and its common cause?
What are the key sensory and motor consequences of late-stage Tabes Dorsalis?
What clinical features define an Argyll-Robertson pupil?
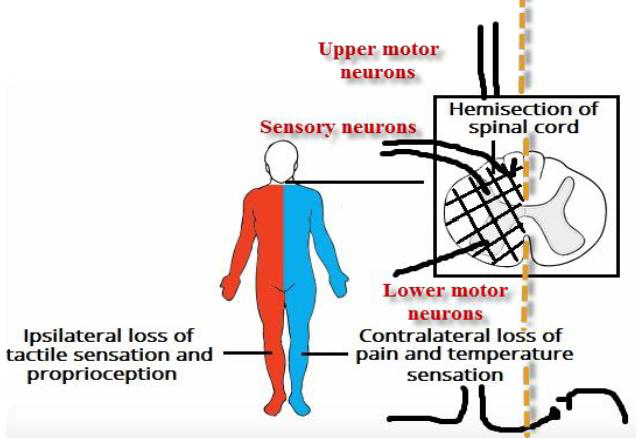
What are the main motor and sensory deficits in Brown-Séquard (hemisection) syndrome?
Name common causes of complete transection of the spinal cord.
What are the sensory and voluntary motor effects of complete spinal cord transection, and how does lesion level affect paralysis?
What is the definition of spinal shock?
What are the key manifestations of spinal shock?
What routine care measures reduce the risk of complications during the stage of spinal shock?
What serious outcome can result from inappropriate care during the stage of spinal shock?
Name one mechanism that can cause recovery of reflex excitability after spinal shock.
How does bladder function behave during recovery of reflexes after spinal shock?
What stimuli can elicit the mass reflex after spinal cord injury and what are its main immediate responses?
What mechanisms explain the mass reflex, and what later motor changes may follow?
What is the primary cause of Thalamic (E-) syndrome?
What are the main immediate and delayed sensory manifestations of Thalamic (E-) syndrome?
Flashcards in this deck (40)
-
What is the effect on voluntary movement in a lower motor neuron (LMN) lesion?
- Localized ipsilateral flaccid paralysis of a muscle or group of muscles supplied by the affected nerves.
lmn motor -
What are the effects on reflexes, muscle tone, and muscle bulk in an LMN lesion?
- Reflexes: decreased or lost (hyporeflexia or areflexia)
- Tone: hypotonia or atonia (flaccidity)
- Muscle bulk: marked atrophy due to loss of activity and loss of trophic effects
 reflexes atrophy
reflexes atrophy -
What are fasciculations and what causes them?
- Definition: Jerky, visible contractions of groups of muscle fibers.
- Can be: felt and seen
- Cause: Pathologic discharge of spinal motor neurons
lmn fasciculation neurology -
What are fibrillations and what causes them?
- Definition: Fine, irregular contractions of individual fibers, detectable electrophysiologically but invisible to the eye.
- Cause: Denervation hypersensitivity of denervated muscles to circulating acetylcholine
 lmn fibrillation neurology
lmn fibrillation neurology -
What is the typical pattern of paralysis after an upper motor neuron lesion above the medulla?
- Generalized contralateral paralysis of half of the body (contralateral hemiplegia)
neurology motor -
After 2 weeks following an upper motor neuron lesion, which improvements occur and what gait does the patient use?
- Improvement: gross movements of axial and proximal limb muscles improve (not regeneration)
- Permanent loss: fine movements of distal muscles
- Gait: circumduction
- Cause: intact ipsilateral corticospinal fibers terminating on medial a cells mediate gross movements
recovery gait -
What characterizes clasp-knife spasticity in upper motor neuron lesions?
- Initial high resistance to passive stretch followed by sudden loss of resistance due to activation of an oversensitive Golgi tendon organ
 neurology spasticity umn
neurology spasticity umn -
What is clonus and where is it commonly tested?
- Repeated cycles of stretch–inverse stretch reflex in a hyperreflexic muscle; commonly tested as patellar clonus (knee) and ankle clonus (ankle)
 neurology reflexes umn
neurology reflexes umn -
Why does an affected muscle show minimal (disuse) atrophy in an upper motor neuron lesion?
- Because voluntary activity is lost while reflex activity is exaggerated
- Trophic effects on muscle metabolism are preserved since the lower motor neuron supply is intact
neurology umn atrophy -
What are the key contrasting features of chronic UMNL versus LMNL regarding laterality, muscle tone, reflexes, clonus, and atrophy?
- Chronic UMNL: Contralateral; spastic paralysis; increased tone; hyperreflexia; clonus present; disuse atrophy on long term
- LMNL: Ipsilateral; flaccid paralysis; decreased tone; hyporeflexia; clonus absent; immediate denervation atrophy
neurology umn lmn reflexes -
What are the facial findings in an upper motor neuron lesion of the corticobulbar tract?
- Upper face is spared
- Lower face is affected
- Contralateral effects
umn facial -
What are the facial findings in a lower motor neuron facial nerve lesion (facial palsy)?
- Upper face is affected
- Lower face is affected
- Ipsilateral effects
 lmn facial
lmn facial -
Examine the photograph:
Which side shows facial paralysis and what are the visible signs?
- Left-sided facial paralysis
- Drooping mouth
- Partially closed eye
neurology facial motor -
Examine the photograph:
Which side shows facial paralysis and what are the visible signs?
- Right-sided facial paralysis
- Drooping mouth
- Inability to close the eye
neurology facial motor -
What is muscle tone and which muscles does it mainly affect?
- Muscle tone: a state of sub-tetanic continuous contraction of skeletal muscle caused by the static component of the stretch reflex.
- Mainly affects antigravity muscles (flexors of upper limbs; extensors of lower limbs; neck and trunk extensors; elevators of lower jaw).
tone antigravity physiology -
Name the two major types of hypertonia and one key clinical difference between them.
- Spasticity: initial resistance followed by sudden release (clasp-knife); caused by upper motor neuron lesion.
- Rigidity: maintained resistance throughout movement (lead-pipe or cog-wheel); associated with lesion in substantia nigra.
 hypertonia spasticity rigidity
hypertonia spasticity rigidity -
Compare the site of lesion and upper limb posture in decorticate versus decerebrate posturing.
- Decorticate: lesion in the upper midbrain (above superior colliculus); upper limbs flexed and adducted
- Decerebrate: lesion in lower midbrain (between colliculi) or upper pons; upper limbs extended
 posturing localization neurology
posturing localization neurology -
List the main causes of hypotonia (flaccidity) from loss of excitatory supraspinal control of static muscle stretch reflex.
- Neocerebellar (cerebellar) lesions
- Chorea
- Lower motor neuron lesion (e.g., tabes dorsalis, polyneuritis, myasthenia gravis)
- Acute stage of upper motor neuron lesion
- Lesion of area 4
- Increased serum Ca++ level
hypotonia causes motor -
What is mononeuropathy and what are its main effects?
- Definition: Lesion of a peripheral nerve.
- Effects: Loss of all sensations in the area supplied by the affected nerve and motor affection in muscles innervated by that nerve.
mononeuropathy peripheral -
What is polyneuropathy and what are common acquired causes?
- Definition: Lesion of multiple peripheral nerves that supply the distal parts of upper and lower limbs.
- Acquired causes: Metabolic disorders (e.g. Diabetes mellites), Physical injury (trauma) to nerves, Tumors, Toxins, Autoimmune responses, Nutritional deficiencies (e.g. vitamin B12), Alcoholism, Vascular.
 polyneuropathy peripheral
polyneuropathy peripheral -
What are the sequential sensory changes in peripheral parts (hands and feet)?
- Numbness, tingling, pricking sensations (paresthesia)
- Then, hypoesthesia (diminished all sensations)
- Then, anesthesia (loss of all sensations)
- Distribution: gloves and stockings sensory loss
 sensory peripheral
sensory peripheral -
What are the motor features of a lower motor neuron lesion (LMNL) in peripheral limbs?
- Muscle weakness (paresis)
- Then, paralysis of muscles
- Loss of reflexes of muscles
- Muscle wasting (atrophy)
motor lmn -
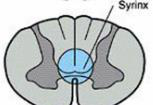
What is syringomyelia and which spinal segments are commonly affected?
- Definition: A cyst or glial tissue/fluid accumulation that enlarges and causes cavitation around the central canal of the spinal cord.
- Common segments: Cervical (may extend to thoracic and medulla oblongata).
syringomyelia spinalcord definition -
What are the characteristic sensory, motor, and autonomic effects of a central cord (syringomyelia) lesion?
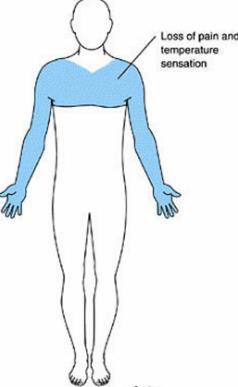
- Sensory: Bilateral loss of pain and temperature in a 'jacket/cape' distribution due to damage to crossing spinothalamic fibers; dorsal column touch preserved (dissociated sensory loss).
- Motor: LMN signs from anterior horn cell damage; UMN signs from corticospinal tract damage.
- Autonomic: Lateral horn damage causing autonomic dysfunction, commonly Horner's syndrome.
 syringomyelia sensory motor autonomic
syringomyelia sensory motor autonomic -
What is Tabes Dorsalis and its common cause?
- Tabes Dorsalis: atrophy of dorsal roots of the spinal cord central to the DRG, commonly affecting lumbosacral segments
- Cause: a complication of neurosyphilis
neurology tabes neurosyphilis -
What are the key sensory and motor consequences of late-stage Tabes Dorsalis?
- Sensory: loss of all sensations in affected dermatomes; first lost = vibration; last lost = slow pain
- Coordination: sensory ataxia requiring vision; stamping (steppage) gait
- Motor: decreased or absent reflexes from deafferentation
tabes sensory reflexes -
What clinical features define an Argyll-Robertson pupil?
- Loss of pupillary light reflex
- Pupil size and near response preserved
neuro ophthalmology pupils -
What are the main motor and sensory deficits in Brown-Séquard (hemisection) syndrome?
- At the level: LMN flaccid paralysis with loss of reflexes; loss of all sensations in the affected dermatome
- Below the level: Ipsilateral UMN spastic paralysis and loss of dorsal column sensations; contralateral loss of spinothalamic sensations
 neuro spinal brown-sequard
neuro spinal brown-sequard -
Name common causes of complete transection of the spinal cord.
- Gunshot injuries
- Dislocation of spine
- Vascular accident
spinalcord causes -
What are the sensory and voluntary motor effects of complete spinal cord transection, and how does lesion level affect paralysis?
- Sensory: complete, permanent loss of all sensations below lesion (damaged sensory tracts lack neurilemma).
- Voluntary motor: complete, permanent loss of voluntary movements below lesion (paralysis).
- Level examples:
- Above C5: fatal (respiratory failure).
- Below C5 (cervical): quadriplegia; diaphragmatic breathing.
- Mid-thoracic: paraplegia; upper limbs intact.
spinalcord effects -
What is the definition of spinal shock?
- Complete loss of all reflexes below the level of the lesion.
neurology spinalshock -
What are the key manifestations of spinal shock?
- Loss of stretch reflex, atonia, areflexia, flaccid muscles
- Loss of flexor withdrawal and superficial reflexes
- Loss of autonomic reflexes causing bladder/rectum retention and overflow dribbling
- Loss of vasomotor tone with hypotension
- Cyanosed, cold, dry paralyzed limbs; bedsores; muscle atrophy; bone demineralization with hypercalcemia
neurology manifestations -
What routine care measures reduce the risk of complications during the stage of spinal shock?
- Physiotherapy to prevent muscle atrophy
- Antibiotics to resist infections of bedsores
- Frequent mobilization in bed to avoid bed sores
- Good nutrition
- Urinary catheter and rectal enema
 spinalshock care bedsores
spinalshock care bedsores -
What serious outcome can result from inappropriate care during the stage of spinal shock?
Severe bedsores and urinary tract infections can cause toxemia that depresses CNS functions, including vital centers, which may lead to death.
spinalshock complications toxemia -
Name one mechanism that can cause recovery of reflex excitability after spinal shock.
- Development of denervation hypersensitivity by remaining spinal neurons, enabling them to respond to afferent stimulation
spinal reflexes -
How does bladder function behave during recovery of reflexes after spinal shock?
- Automatic bladder evacuation similar to infants: fills to about 150 ml then reflexive evacuation without voluntary control
spinal autonomic -
What stimuli can elicit the mass reflex after spinal cord injury and what are its main immediate responses?
- Stimuli: scratching skin over lower limbs or anterior abdominal wall
- Immediate responses: spasm of flexor muscles in both limbs; evacuation of rectum and bladder; profuse sweating below lesion; contraction of abdominal muscles; erection; elevation of ABP
neuro spinalcord massreflex -
What mechanisms explain the mass reflex, and what later motor changes may follow?
- Mechanisms: denervation hypersensitivity; release from inhibitory gamma motor neurons; increased spinal collaterals causing irradiation and reverberation
- Later changes: increased extensor tone (paraplegia in extension); flexor withdrawal with crossed extensor reflex; return of infantile reflexes (grasp, positive Babinski)
mechanism spasticity neurophysiology -
What is the primary cause of Thalamic (E-) syndrome?
- Hematoma or thrombosis of the thalamo-geniculate artery
thalamus etiology neurology -
What are the main immediate and delayed sensory manifestations of Thalamic (E-) syndrome?
- Immediate: Crossed hemi-anesthesia; secondary hyperalgesia; sensory ataxia
- Delayed: Crude sensation recovery with poor localization; fine sensation never recovers; secondary hyperalgesia; paroxysmal pain attacks; thalamic hyperpathia; emotional disturbances; motor ataxia
thalamus sensory clinical
Overview
- This document summarizes clinical features of motor (UMN vs LMN) lesions, muscle tone disorders, and sensory pathway lesions at peripheral, spinal and central levels.
- Focus on key signs used in localization: paralysis pattern, tone changes, reflexes, atrophy, sensory distribution and special syndromes.
I. Lower Motor Neuron (LMN) Lesion
Definition & causes
- Lesion of spinal motor neurons, anterior horn cells, or cranial nerve nuclei/roots. Common cause: poliomyelitis, peripheral nerve injury.
Key clinical features
- Voluntary movement: Localized, ipsilateral flaccid paralysis of a muscle or muscle group supplied by the affected nerve.
- Reflexes & tone: Loss or marked reduction of stretch and tendon reflexes (hyporeflexia/areflexia) and hypotonia/atonia (flaccidity) due to interruption of the reflex arc.
- Muscle state: Marked denervation atrophy (wasting) from loss of trophic support and inactivity.
- Spontaneous activity: Fasciculations (visible jerky contractions of muscle bundles) and fibrillations (fine, single-fiber discharges seen on EMG) due to motor neuron instability.
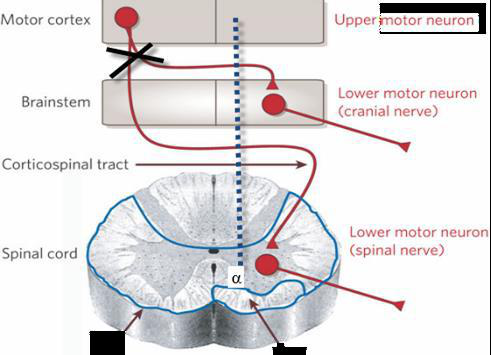
II. Upper Motor Neuron (UMN) Lesion
Definition & causes
- Lesion of descending cortical motor pathways (corticospinal/corticobulbar) from cortex to spinal motor neurons or cranial nerve nuclei. Common causes: stroke, tumor, trauma.
Key clinical features
- Voluntary movement: Typically contralateral hemiplegia (if lesion above decussation); if below medulla, deficits may be ipsilateral.
- Time course: After ~2 weeks some recovery of axial and proximal gross movements may occur, but fine distal movements often remain permanently impaired.
- Reflexes & tone: Hyperreflexia, spasticity (hypertonia), and positive Babinski sign. Spasticity often affects antigravity muscles and may show clasp-knife phenomenon.
- Clonus: Repeated stretch-induced cycles seen in hyperreflexic muscles (e.g., ankle or patellar clonus).
- Muscle state: Mild disuse atrophy only (LMN intact) — no marked denervation atrophy.
Comparison (clinical highlights)
- LMN: flaccid paralysis, decreased tone/reflexes, marked atrophy, fasciculations present.
- UMN: spastic paralysis, increased tone/reflexes, minimal atrophy, Babinski +, clonus possible.
Facial weakness: Corticobulbar vs Facial Nerve (CN VII)
- UMN (corticobulbar) lesion: Contralateral lower face weakness; upper face spared due to bilateral cortical innervation.
- LMN (facial nerve/nucleus) lesion: Ipsilateral weakness of both upper and lower face.
III. Disorders of Muscle Tone
Definition
- Muscle tone: Passive resistance of a relaxed muscle to passive stretch; largely due to static component of the stretch reflex, especially in antigravity muscles.
Hypertonia types
- Spasticity: UMN lesion; velocity-dependent increased tone with initial resistance then sudden release (clasp-knife). Affects mainly antigravity muscles.
- Rigidity: Extrapyramidal (e.g., substantia nigra); uniform resistance (lead-pipe) or interrupted resistance (cogwheel). Not velocity dependent.
Posturing patterns
- Decorticate: Lesion above upper midbrain — flexed/adducted upper limbs, extended lower limbs (moderate rigidity).
- Decerebrate: Lesion at lower midbrain/upper pons — extension of limbs and neck (more severe rigidity).
Causes of hypotonia (flaccidity)
- Acute UMN lesion, cerebellar disease, chorea, LMN lesions (e.g., polyneuritis, myasthenia gravis), lesions of primary motor cortex, hypercalcemia.
IV. Sensory Lesions — Levels & Patterns
- Lesion locations: peripheral nerve, spinal cord, brainstem, thalamus, sensory cortex.
1) Peripheral nerve lesions
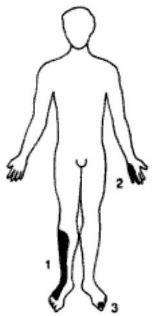
- Mononeuropathy: sensory loss confined to one nerve's distribution plus corresponding LMN signs in its muscles.
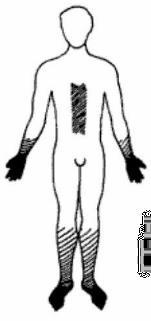
- Polyneuropathy: distal, symmetric sensory loss ("glove and stocking"), paresthesias → hypoesthesia → anesthesia; motor involvement causes distal weakness, hyporeflexia and wasting. Causes include diabetes, toxins, B12 deficiency, alcoholism.
2) Spinal cord lesions
- Important syndromes are listed below with essential signs.
Syringomyelia (central cord)
- Cavity (syrinx) around central canal, often cervical; expands and interrupts crossing spinothalamic fibers.
- Classic early sign: bilateral loss of pain & temperature in a "cape" or "jacket" distribution over shoulders/upper limbs with preserved dorsal column modalities (dissociated sensory loss).
- Progressive involvement may produce anterior horn (LMN) signs at level and corticospinal (UMN) signs below level; autonomic involvement (e.g., Horner's syndrome) possible.
Tabes dorsalis (posterior column)
- Late neurosyphilis causing dorsal root/column degeneration; early lancinating leg pain, later loss of proprioception and vibration, sensory ataxia (positive Romberg), high-stepping (stamping) gait.
- Reflexes and muscle tone in related segments are reduced due to deafferentation.
Brown-Séquard (hemisection)
- At level: ipsilateral LMN signs and segmental sensory loss.
- Below level: ipsilateral UMN signs (spasticity), ipsilateral dorsal column loss (vibration/proprioception), and contralateral loss of pain/temp (spinothalamic) beginning ~1–2 levels below lesion.
Complete transection
- Complete loss of all sensation and voluntary movement below level of lesion; the clinical picture depends on level (e.g., injuries above C5 compromise respiration).
V. Spinal Shock, Recovery & Complications
Spinal shock (acute)
- Sudden loss of all reflexes, flaccidity, urinary/rectal retention, hypotension due to loss of sympathetic tone. Duration typically 2–6 weeks in humans.
- Complications during shock: decreased perfusion of limbs, bedsores, infection, muscle atrophy, bone demineralization.
Recovery of reflexes (if well managed)
- Reflexes gradually return due to denervation hypersensitivity and collateral sprouting; sequence: tone and flexor reflexes return, then deep tendon jerks (knee then ankle), and automatic bladder/rectal reflexes but not voluntary control.
- Mass reflexes: exaggerated autonomic and motor responses (sweating, bladder/rectal emptying, spasm) to cutaneous stimuli may occur.
Care priorities during spinal shock
- Prevent pressure ulcers and infections (frequent repositioning, wound care, antibiotics), maintain nutrition, physiotherapy to limit atrophy, bladder/bowel care (catheterization/enema).
VI. Thalamic (Dejerine-Roussy) Syndrome — key points
- Caused by thalamogeniculate artery lesion (thalamic infarct). Initial contralateral hemisensory loss, later persistent disturbed sensation: poorly localized crude sensation, secondary hyperalgesia, paroxysmal pain, emotional changes and sensory ataxia.
Quick clinical signs checklist (localization)
- Flaccid paralysis + hyporeflexia + fasciculations → LMN lesion.
- Spastic paralysis + hyperreflexia + Babinski + clonus → UMN lesion.
- Lower face only weak → UMN (corticobulbar); whole half-face weak → LMN (facial nerve).
- "Glove-and-stocking" distal loss → polyneuropathy.
- Cape distribution pain/temp loss with preserved touch → syringomyelia (central cord).
- Ipsilateral proprioception loss + contralateral pain/temp loss → Brown-Séquard hemisection.
Practical tips for exams
- Test tone, power, reflexes (deep & superficial), plantar response (Babinski), clonus, and look for fasciculations and wasting.
- Map sensory loss precisely (dermatomes vs peripheral nerve territories) to distinguish root/cord/nerve lesions.
- Always consider level of lesion for spinal cord injuries (respiratory risk above C5).