Sign up to unlock more features
- Save this deck to your account
- Study flashcards with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from PDFs and documents
- Better text extraction from your PDFs and documents
- Better flashcards with our more advanced AI model
What is the primary role of platelets in the vasculature?
How are platelets described metaphorically in the lecture?
What is the cellular origin and nuclear status of platelets?
What is the typical size of platelets according to the notes?
What is the approximate lifespan of a platelet?
What is the normal platelet count range provided in the notes?
Name the main ultrastructural components shown in the platelet diagram.
List the platelet surface receptors provided in the text.
Which substances are contained in platelet dense granules according to the text?
Which substances are listed as contents of the (alpha) granules in the text?
What is Von Willebrand factor (VWF)?
Which binding sites does VWF contain?
What is required for VWF binding sites to become exposed?
What subunits compose the GPIb‑V‑IX complex receptor on platelets?
How is the GPIb‑V‑IX complex connected within the platelet?
Which molecular interactions are shown for the GPIb‑V‑IX complex in the schematic?
What is the VWF-GPIba complex?
What is the primary function of the VWF-GPIba complex?
What are the sequential steps by which von Willebrand factor (VWF) mediates platelet adhesion at a vascular injury site?
Which change in VWF exposes platelet-binding sites for GPIbα?
What is Von Willebrand disease (VWD) and how common is it?
What general cause underlies Von Willebrand disease according to the text?
List the specific functional consequences of VWF genetic defects described in the text.
What is Bernard-Soulier syndrome?
How does the GPIba defect in Bernard-Soulier syndrome affect platelet function?
What is the primary clinical consequence of Bernard-Soulier syndrome?
What are the main steps of platelet activation?
Which cell surface integrin is listed as activated during platelet activation?
What are the purposes of platelet 'activation' in haemostasis?
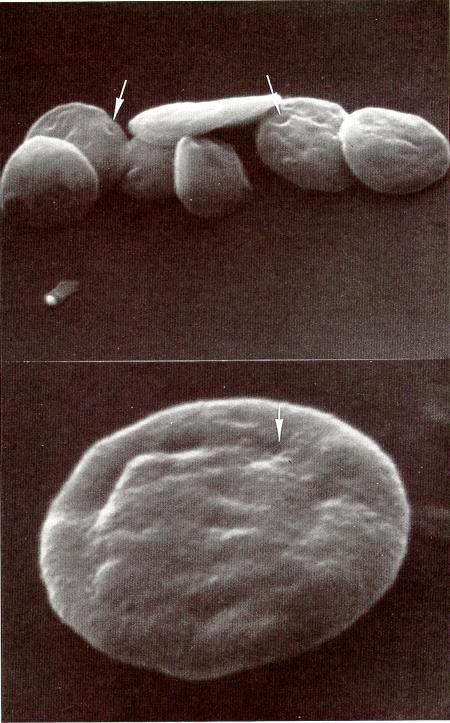
When do platelets undergo a change in shape during adhesion?
What morphological changes do platelets exhibit after adhesion?
What cytoskeletal change underlies platelet shape change?
What are the main platelet granule types and their primary contents/functions?
What is the open canalicular system (OCS) in platelets?
What structural feature on the platelet surface forms the entrances into the OCS?
What is the primary clinical use of inhibitors of platelet activation?
What is the most common example of an inhibitor of platelet activation?
By what mechanism do inhibitors of platelet activation act?
What does 'flip-flop' of phospholipids refer to in platelet membranes?
Why is phospholipid externalization on activated platelets important for coagulation?
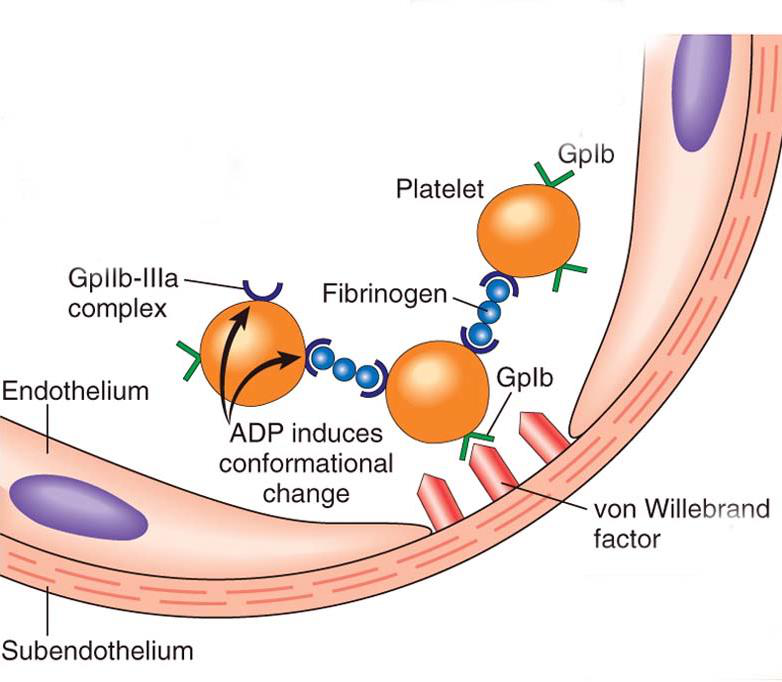
What triggers activation of the platelet membrane glycoprotein complex GPIIb/IIIa and what is its primary function?
Which major ligands does the platelet receptor GPIIb/IIIa bind?
What is the consequence of GPIIb/IIIa deficiency for platelet function at a vessel injury site?
Which clinical disorder is caused by deficiency of the GPIIb/IIIa receptor?
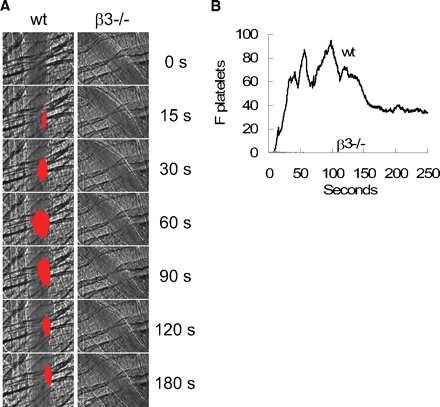
How does platelet aggregation compare between wild-type and beta3-deficient (3-/-) subjects in the provided experiment?
What is abciximab classified as?
What is the primary mechanism of action of abciximab on platelets?
What is the main clinical use of abciximab described in the text?
Flashcards in this deck (48)
-
What is the primary role of platelets in the vasculature?
- Circulate as quiescent cells and survey vascular integrity
- Undergo explosive activation upon vessel wall damage
-
How are platelets described metaphorically in the lecture?
They are described as the 'unmanned drones of the vasculature'
-
What is the cellular origin and nuclear status of platelets?
- Anucleate discs derived from megakaryocyte
-
-
-
What is the normal platelet count range provided in the notes?
Normal platelet count: 150 - 400 x 10 /litre
-
Name the main ultrastructural components shown in the platelet diagram.
- Glycogen
- Phospholipid membrane
- Open canalicular system
- Mitochondrion
- Dense granules
- Alpha granules
-
List the platelet surface receptors provided in the text.
- Gp VI
- Gp Ib-IX-V complex
- Gp IIb-IIIa complex
-
Which substances are contained in platelet dense granules according to the text?
- Ca
- ADP / ATP
- Serotonin
-
Which substances are listed as contents of the (alpha) granules in the text?
- VWF
- Fibrinogen
- Factor V
- PF4
-
-
Which binding sites does VWF contain?
- Binding sites for platelets
- Binding sites for sub-endothelial tissue
-
What is required for VWF binding sites to become exposed?
- VWF must be 'tethered' for its binding sites to be exposed
-
-
How is the GPIb‑V‑IX complex connected within the platelet?
- It is coupled to the underlying cytoskeleton.
-
Which molecular interactions are shown for the GPIb‑V‑IX complex in the schematic?
- Interactions with VWF, P‑selectin, Thrombin, Filamin, and Calmodulin
-
What is the VWF-GPIba complex?
- Interaction between a circulating plasma protein (Von Willebrand Factor; VWF) and a platelet surface receptor (glycoprotein Ib; GPIba).
-
What is the primary function of the VWF-GPIba complex?
- It is crucial for platelet adhesion in high shear conditions.
-
What are the sequential steps by which von Willebrand factor (VWF) mediates platelet adhesion at a vascular injury site?
- VWF becomes tethered to the site of vascular injury
- VWF unravels, exposing binding sites for GPIbα
- Platelets bind to the site of injury via GPIb
-
Which change in VWF exposes platelet-binding sites for GPIbα?
VWF unravels, which exposes binding sites for GPIbα.
-
What is Von Willebrand disease (VWD) and how common is it?
- Von Willebrand disease (VWD): the most common bleeding disorder
- Prevalence: ~1 in 1000
-
What general cause underlies Von Willebrand disease according to the text?
- Cause: Genetic defects in von Willebrand factor (VWF)
-
List the specific functional consequences of VWF genetic defects described in the text.
- Consequences:
- Low VWF levels
- Inability of VWF to bind collagen or platelets
- Failure to bind sub-endothelial tissue or platelets
-
What is Bernard-Soulier syndrome?
- Bernard-Soulier syndrome is a rare genetic defect in GPIba that prevents normal von Willebrand factor (VWF) interaction.
-
How does the GPIba defect in Bernard-Soulier syndrome affect platelet function?
- The GPIba defect prevents normal VWF–GPIb interaction, which prevents normal thrombus formation.
-
What is the primary clinical consequence of Bernard-Soulier syndrome?
- A bleeding tendency due to impaired thrombus formation.
-
What are the main steps of platelet activation?
- Change in platelet shape
- Activation of cell surface integrins (Gpllb/llla)
- Granule secretion
- 'Flip/Flop' of plasma membrane
-
-
What are the purposes of platelet 'activation' in haemostasis?
- Adopt structural changes to help clot formation
- Secretion of factors that facilitate clot formation
- Activate cell surface molecules to make them 'sticky' for other platelets and coagulation factors
-
-
-
What cytoskeletal change underlies platelet shape change?
Reorder of actin and tubulin polymers of the cytoskeleton
Answer image:
-
What are the main platelet granule types and their primary contents/functions?
- Dense granules: rich in chemical messengers that promote further platelet activation and aggregation
- Alpha granules: rich in clotting proteins and contribute to further clot formation
-
What is the open canalicular system (OCS) in platelets?
An extensive system of internal membrane tunnels that serves as a conduit system for granule release.
-
What structural feature on the platelet surface forms the entrances into the OCS?
- Periodic invaginations on a flat platelet surface
-
What is the primary clinical use of inhibitors of platelet activation?
- To prevent arterial thrombosis (lesions rich in aggregated platelets)
-
-
By what mechanism do inhibitors of platelet activation act?
- They inhibit signaling pathways that lead to platelet activation
-
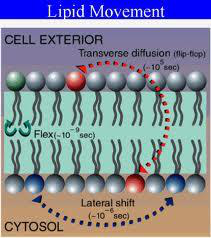
What does 'flip-flop' of phospholipids refer to in platelet membranes?
The transverse movement where negatively charged phospholipids that were on the inner leaflet become externalized to the outer leaflet of the platelet membrane.
-
Why is phospholipid externalization on activated platelets important for coagulation?
- It is necessary for vitamin K-dependent coagulation factor binding
-
What triggers activation of the platelet membrane glycoprotein complex GPIIb/IIIa and what is its primary function?
- Trigger: Platelet activation causes membrane activation of the glycoprotein complex IIb/IIIa
- Primary function: Acts to cause platelet aggregation
-
Which major ligands does the platelet receptor GPIIb/IIIa bind?
- Ligands: von Willebrand factor (VWF) and fibrinogen
-
What is the consequence of GPIIb/IIIa deficiency for platelet function at a vessel injury site?
- Platelet plug fails to accumulate at the site of vessel injury when GPIIb/IIIa is absent.
-
Which clinical disorder is caused by deficiency of the GPIIb/IIIa receptor?
- Glanzmann's thrombasthenia
-
How does platelet aggregation compare between wild-type and beta3-deficient (3-/-) subjects in the provided experiment?
- Beta3-deficient (3-/-) subjects show reduced platelet aggregation compared with wild-type (wt).
Answer image:
-
-
What is the primary mechanism of action of abciximab on platelets?
- Blocks GPIIb/IIIa, thereby inhibiting platelet aggregation
-
What is the main clinical use of abciximab described in the text?
- Prevents formation of blood clots during procedures to open blocked arteries
Platelets — quick overview
- Definition: Small, anucleate cell fragments from megakaryocytes that patrol the vasculature and respond to injury.
- Size: \(2\)–\(4\,\mu m\).
- Lifespan: \(\sim 10\ \text{days}\).
- Normal count: \(150\)–\(400\times 10^9\ \text{L}^{-1}\).
- Function: maintain vascular integrity, form primary haemostatic plug after injury.
Ultrastructure & key components
- Major compartments: phospholipid membrane, open canalicular system (OCS), mitochondria, dense granules, alpha granules.
- Surface receptors (important): GPIb-IX-V complex, GPVI, GPIIb/IIIa.
- Dense granules: contain Ca2+, ADP/ATP, serotonin — promote activation and recruitment.
- Alpha granules: contain VWF, fibrinogen, factor V, platelet factor 4 — supply clotting and adhesive proteins.
Image — platelet ultrastructure
How platelets find and stick to injured vessel (adhesion)
- First step: exposed subendothelial matrix (e.g., collagen) at injury site captures circulating proteins and platelets.
- Key mediator: Von Willebrand factor (VWF) — a multimeric plasma protein that must tether/unravel to expose platelet-binding sites.
- When VWF unravels it exposes binding sites for GPIba (part of the GPIb-IX-V complex) and for collagen.
Image — VWF unwinding
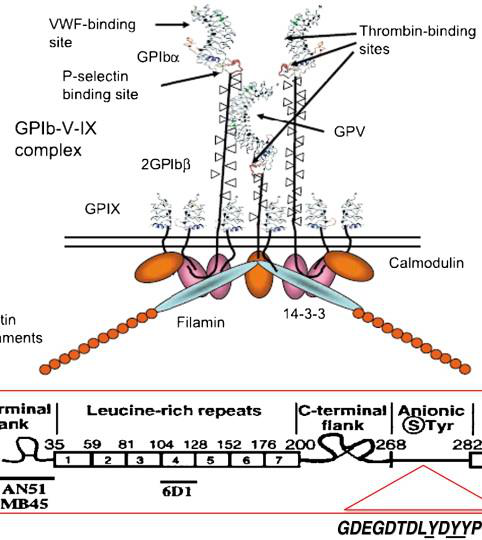
GPIb-IX-V complex (platelet receptor)
- Composed of subunits GPIba, GPIb, GPIX, GPV and linked to the cytoskeleton.
- Function: binds unfolded/tethered VWF under high shear, initiating platelet tethering and slowing of platelets near the lesion.
Image — GPIb-IX-V schematic
VWF–GPIba interaction — why it matters
- Under high shear (arteries), direct platelet adhesion to collagen is inefficient; VWF acting through GPIba is essential.
- If VWF tethering or GPIba binding is impaired, platelet adhesion at sites of high shear fails and bleeding occurs.
Important clinical defects in adhesion
- Von Willebrand disease (VWD): most common bleeding disorder; caused by quantitative (low VWF) or qualitative (impaired binding to collagen/platelets) defects in VWF.
- Bernard–Soulier syndrome: rare genetic defect in GPIb\/a (GPIb-IX-V) that prevents normal VWF interaction and causes bleeding tendency.
Platelet activation — overview
- Activation converts a quiescent platelet into a haemostatic cell capable of adhesion, secretion, and aggregation.
- Four main changes on activation:
- Shape change (discoid → spherical with pseudopodia).
- Activation of integrins (notably GPIIb\/IIIa).
- Granule secretion (dense and alpha granules).
- Phospholipid "flip-flop" exposing anionic surface.
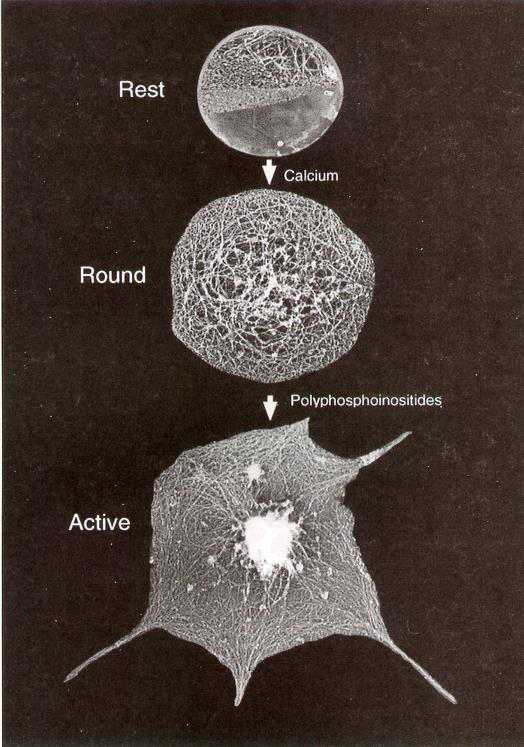
Image — platelet shape change (SEM)
1) Shape change
- Occurs within seconds after adhesion; actin and microtubule reorganisation produces spherical shape and filopodia to increase surface contact and stability.
2) Granule release
- Dense granules: release small-molecule agonists (ADP, Ca2+, serotonin) that amplify activation and recruit platelets.
- Alpha granules: release adhesive and clotting proteins (VWF, fibrinogen, factor V, PF4) to support aggregation and coagulation.
Open canalicular system (OCS)
- Membrane invaginations forming tunnels linking interior granules to the surface; acts as a conduit for rapid secretion and membrane expansion during activation.
Image — OCS (platelet surface invaginations)
3) Phospholipid "flip-flop"
- Activation externalises negatively charged phospholipids (e.g., phosphatidylserine) previously on the inner leaflet.
- This anionic surface is required for assembly/binding of several coagulation complexes and vitamin K–dependent factors on the platelet surface.
Image — lipid bilayer and flip-flop
4) GPIIb\/IIIa activation and platelet aggregation
- GPIIb\/IIIa (integrin αIIbβ3) undergoes a conformational change on activation, allowing it to bind fibrinogen and VWF and cross-link adjacent platelets, forming an aggregate.
- Without functional GPIIb\/IIIa, platelets cannot form a stable plug (see Glanzmann thrombasthenia).
Image — GPIIb\/IIIa interacting with fibrinogen/VWF
Clinical correlates related to aggregation
- Glanzmann thrombasthenia: genetic deficiency of GPIIb\/IIIa → defective aggregation and mucocutaneous bleeding.
- GPIIb\/IIIa inhibitors (e.g., Abciximab): monoclonal antibodies that block the receptor to prevent platelet aggregation during coronary interventions.
Image — aspirin (common platelet inhibitor)

Pharmacologic inhibition of platelet activation
- Aspirin: irreversibly inhibits COX-1 in platelets, reducing thromboxane A2 synthesis and impairing activation/aggregation.
- GPIIb\/IIIa antagonists (Abciximab): block final common pathway of platelet aggregation.
Key takeaways (high-yield)
- Platelet adhesion under high shear relies on VWF tethering and the GPIb-IX-V receptor.
- Activation causes shape change, granule release, phospholipid externalisation, and integrin activation (GPIIb\/IIIa) — together produce aggregation and support coagulation.
- Major disorders: VWD (VWF defects), Bernard–Soulier (GPIb defect), Glanzmann thrombasthenia (GPIIb\/IIIa defect).
- Antiplatelet drugs target different stages: aspirin (activation signaling) and GPIIb\/IIIa inhibitors (aggregation).
Quick self-test questions
- What receptor mediates VWF-dependent adhesion under high shear?
- Which granule type releases ADP and serotonin?
- Name two clinical syndromes caused by defects in GPIb or GPIIb\/IIIa.