Sauvegarde ton deck avant qu'il ne disparaisse
Ces flashcards ne sont pas encore sauvegardées — elles seront perdues si tu quittes. Crée un compte gratuit pour les garder et débloquer tout ce qui suit.
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
COVID-19 is an infection caused by _______, which is a _______ and causes respiratory and systemic disease ranging from asymptomatic to critical illness.
Key steps in COVID-19 pathogenesis: - Virus binds _______ via the _______ and enters respiratory epithelium - Replication triggers _______ - Severe disease: _______ causing ARDS, multiorgan injury and coagulopathy
ARDS in COVID-19 is _______ from a "cytokine storm" within _______ of COVID, often with _______.
Symptoms of COVID-19 by severity: - Mild: _______ - Moderate: _______ - Severe: _______
Extra-respiratory manifestations of COVID-19 include _______.
Major risk factors for severe COVID-19 include _______.
Investigations commonly show _______, raised _______, possible _______, raised _______, and _______ in severe disease; diagnostic test: _______.
Oxygen therapy target for most COVID-19 patients is SpO2 _______, with stepwise escalation: _______.
First-line treatments: _______ for those needing oxygen; _______ for hospitalised patients on O2 if symptom onset is <7 days. Second-line: _______ for systemic inflammation and _______ in hospitalised patients. Prevention: _______.

Influenza is an acute viral respiratory infection caused by _______ or _______ viruses.
Key steps in influenza pathogenesis: - Virus binds respiratory epithelial cells via _______ - _______ → cell death and airway inflammation - _______ causes systemic symptoms
Common systemic symptoms of influenza include _______, _______, _______, _______ and _______.
Respiratory and less common GI symptoms of influenza: - Respiratory: _______, _______, _______ - GI (less common): _______, _______, _______
Major complications of influenza include _______, _______, _______, _______ and _______.
Key risk groups for severe influenza are people _______, _______, with _______, _______ and residents of _______.
Investigations for suspected influenza: clinical diagnosis in mild cases; for confirmation use _______. In severe cases consider _______ and _______ if pneumonia is suspected.
Treatment and prevention: First-line is supportive care and _______ for fever. If severe/hospitalised or immunocompromised, aim within 48 hours to give _______ or _______. Prevention: _______ (live attenuated in children, inactivated in adults).
Influenza classification includes Types, Subtypes/Lineages, Clades and Sub-clades. The provided diagram illustrates these groupings: 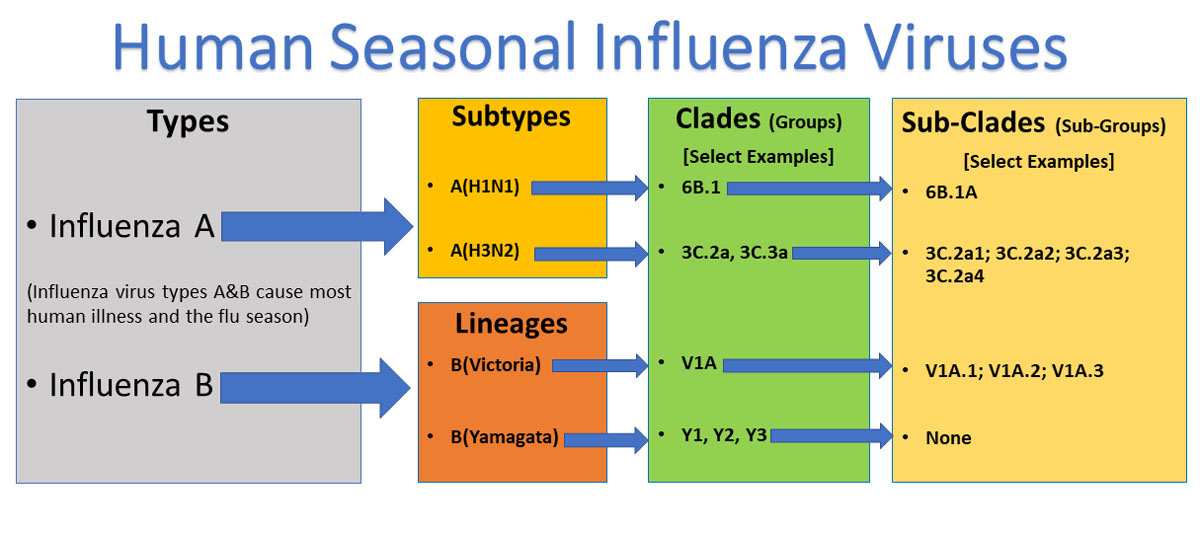 Which hierarchical groups are shown in the diagram? _______
Which hierarchical groups are shown in the diagram? _______
Upper respiratory tract infections (URTIs) are acute infections affecting structures above the vocal cords: _______, _______, _______ or _______.
Common clinical types of URTIs include: - _______ - _______ - _______ - _______ - _______ - _______
Typical URTI symptoms include: _______, _______, _______, _______ and sometimes _______.
Red-flag URTI signs requiring urgent attention: _______, _______, _______, _______, _______, _______. 
URTI risk factors include being _______, _______, having _______, seasonal peaks (_______), _______ and _______.
Investigations for mild URTI are _______; if severe/atypical consider _______ (strep culture/rapid antigen) and _______ (viral PCR for COVID/influenza).
First-line supportive URTI treatment: _______, _______, _______ or _______ plus analgesics/antipyretics (_______, _______).
Recommended antibiotics for specific bacterial URTIs: _______ for strep throat (Group A), _______ for bacterial sinusitis and _______ for otitis media.
Antiviral guidance: _______ is indicated for influenza in _______ patients.
Lower respiratory tract infections (LRTIs) are infections below the larynx involving: - _______ - _______ - _______
Common types of LRTIs include: - _______ - _______ - _______ - _______ - _______ - _______ - _______
Typical viral causes listed for acute bronchitis and bronchiolitis include: _______, _______, _______, _______, _______
Common bacterial pathogens causing community-acquired pneumonia (CAP) are _______ and _______.
Key symptoms of LRTIs include: - _______ - _______ - _______ - _______ - _______ - _______
Risk factors for LRTIs include: _______, age _______, chronic lung disease (_______), _______, _______, _______, and _______ stay.
Investigations for suspected LRTI include blood tests: _______, _______, _______, _______, plus _______ and _______ and _______ for influenza/COVID, and _______ for imaging.
A chest X-ray showing consolidation suggests _______.
First-line antibiotic for uncomplicated acute bronchitis given here is _______.
Empirical treatment for CAP in moderate disease is _______ and for severe CAP is _______.
HAP treatment: early (<5 days) options include _______; late-onset or high-risk HAP uses _______.
VAP recommended empirical therapy is _______, adding _______ if there is MRSA risk.
For COPD exacerbation, antibiotics are recommended only if there is increased _______ and _______; first-line is _______ and second-line _______.
Flashcards in this deck (40)
-
COVID-19 is an infection caused by SARS‑CoV‑2, which is a positive-sense RNA coronavirus and causes respiratory and systemic disease ranging from asymptomatic to critical illness.
covid virology pathogenesis -
Key steps in COVID-19 pathogenesis: - Virus binds ACE2 receptor via the spike protein and enters respiratory epithelium - Replication triggers immune response - Severe disease: cytokine storm causing ARDS, multiorgan injury and coagulopathy
pathogenesis covid -
ARDS in COVID-19 is hypoxaemic respiratory failure from a "cytokine storm" within 1 week of COVID, often with bilateral opacities on CXR.
complications ards covid -
Symptoms of COVID-19 by severity: - Mild: fever, cough, fatigue, anosmia, myalgia, sore throat - Moderate: SOB and O2 sat 90–94% - Severe: hypoxia <90%, ARDS, multi-organ failure
presentation symptoms covid -
Extra-respiratory manifestations of COVID-19 include GI (diarrhoea/nausea), neuro (headache, confusion, anosmia), cardiac (myocarditis), and skin (rashes/COVID toes).
manifestations covid systems -
Major risk factors for severe COVID-19 include age >65, male sex, comorbidities (DM, CKD, COPD, CVD, obesity), immunosuppression, third trimester pregnancy, and unvaccinated status.
riskfactors covid -
Investigations commonly show lymphopenia, raised CRP and D-dimer, possible mild thrombocytopenia, raised ferritin/LDH, and troponin in severe disease; diagnostic test: RT-PCR nasopharyngeal swab.
investigations covid labs -
Oxygen therapy target for most COVID-19 patients is SpO2 92–96%, with stepwise escalation: nasal cannula → face mask → high-flow nasal O2 → CPAP → mechanical ventilation.
management oxygen covid -
First-line treatments: dexamethasone for those needing oxygen; IV remdesivir for hospitalised patients on O2 if symptom onset is <7 days. Second-line: tocilizumab for systemic inflammation and prophylactic LMWH/UFH in hospitalised patients. Prevention: vaccine.
treatment covid pharmacology -
Influenza is an acute viral respiratory infection caused by influenza A or influenza B viruses.
infectiousdisease influenza overview -
Key steps in influenza pathogenesis: - Virus binds respiratory epithelial cells via Hemagglutinin (HA) - Viral replication → cell death and airway inflammation - Host immune response causes systemic symptoms
pathogenesis influenza virology -
Common systemic symptoms of influenza include fever, chills, myalgia, headache and malaise.
symptoms influenza clinical -
Respiratory and less common GI symptoms of influenza: - Respiratory: cough, sore throat, nasal congestion - GI (less common): nausea, vomiting, diarrhea
symptoms influenza clinical -
Major complications of influenza include viral or secondary pneumonia, COPD/asthma exacerbation, myocarditis, encephalitis and multi organ failure.
complications influenza clinical -
Key risk groups for severe influenza are people over 65 years, pregnant, with chronic heart, lung, liver, or renal disease, immunocompromised and residents of long-term care facilities.
riskfactors influenza publichealth -
Investigations for suspected influenza: clinical diagnosis in mild cases; for confirmation use RT-PCR from nasopharyngeal swab. In severe cases consider FBC, CRP and CXR if pneumonia is suspected.
investigations diagnosis influenza -
Treatment and prevention: First-line is supportive care and paracetamol for fever. If severe/hospitalised or immunocompromised, aim within 48 hours to give oseltamivir (oral) or zanamivir (inhaled). Prevention: annual influenza vaccine (live attenuated in children, inactivated in adults).
treatment prevention influenza -
Influenza classification includes Types, Subtypes/Lineages, Clades and Sub-clades. The provided diagram illustrates these groupings:
Which hierarchical groups are shown in the diagram? Types, Subtypes/Lineages, Clades, Sub-cladesclassification influenza virology -
Upper respiratory tract infections (URTIs) are acute infections affecting structures above the vocal cords: nose, pharynx, larynx or sinuses.
ent urti -
Common clinical types of URTIs include: - Common cold - Pharyngitis/Tonsillitis - Laryngitis - Sinusitis/rhinosinusitis - Otitis media/eustachian tube dysfunction - Epiglottitis
types urti -
Typical URTI symptoms include: nasal congestion, rhinorrhoea, sore throat, cough and sometimes low-grade fever.
symptoms urti -
Red-flag URTI signs requiring urgent attention: stridor, drooling, severe pain, high fever, neck stiffness, immunosuppression.
redflag safety -
URTI risk factors include being young, immunosuppressed, having asthma/COPD, seasonal peaks (winter viruses), smoking and close contact.
risk epidemiology -
Investigations for mild URTI are clinical; if severe/atypical consider throat swab (strep culture/rapid antigen) and nasopharyngeal swab (viral PCR for COVID/influenza).
investigations diagnosis -
First-line supportive URTI treatment: rest, hydration, saline nasal spray or steam inhalation plus analgesics/antipyretics (paracetamol, ibuprofen).
treatment management -
Recommended antibiotics for specific bacterial URTIs: Phenoxymethylpenicillin for strep throat (Group A), Amoxicillin for bacterial sinusitis and Amoxicillin for otitis media.
antibiotics treatment -
Antiviral guidance: Oseltamivir is indicated for influenza in high-risk patients.
antivirals treatment -
Lower respiratory tract infections (LRTIs) are infections below the larynx involving: - trachea - bronchi/bronchioles - lung parenchyma (alveoli)
lrti definition respiratory -
Common types of LRTIs include: - Acute bronchitis - Bronchiolitis - Community-acquired pneumonia (CAP) - Healthcare-associated pneumonia (HAP) - Ventilator-associated pneumonia (VAP) - Exacerbation of COPD - COVID-19 / Influenza pneumonia
types lrti -
Typical viral causes listed for acute bronchitis and bronchiolitis include: influenza A/B, RSV, COVID, adenovirus, parainfluenza
etiology viral bronchitis -
Common bacterial pathogens causing community-acquired pneumonia (CAP) are Streptococcus pneumoniae and Haemophilus influenzae.
etiology bacterial cap -
Key symptoms of LRTIs include: - Cough - Fever / chills - Dyspnoea - Wheeze - Pleuritic chest pain - Fatigue / malaise
symptoms presentation -
Risk factors for LRTIs include: Smoking, age <5 or >65, chronic lung disease (COPD & Asthma), bronchiectasis, diabetes mellitus, immunosuppression, and recent hospital stay.
risk epidemiology -
Investigations for suspected LRTI include blood tests: FBC, CRP, U&E, LFT, plus sputum culture and blood culture if severe and viral PCR for influenza/COVID, and CXR for imaging.
investigations diagnosis -
A chest X-ray showing consolidation suggests pneumonia.
investigations cxr -
First-line antibiotic for uncomplicated acute bronchitis given here is Amoxicillin.
treatment bronchitis antibiotics -
Empirical treatment for CAP in moderate disease is co-amoxiclav + doxycycline/clarithromycin and for severe CAP is benzylpenicillin + clarithromycin.
treatment cap antibiotics -
HAP treatment: early (<5 days) options include co-amoxiclav OR doxycycline; late-onset or high-risk HAP uses piperacillin-tazobactam (Tazocin).
treatment hap -
VAP recommended empirical therapy is piperacillin-tazobactam (Tazocin), adding vancomycin if there is MRSA risk.
treatment vap antibiotics -
For COPD exacerbation, antibiotics are recommended only if there is increased sputum purulence, sputum volume and dyspnoea; first-line is doxycycline and second-line amoxicillin.
treatment copd antibiotics
COVID-19 — key points
- Definition: Infection caused by SARS‑CoV‑2, a positive‑sense RNA coronavirus causing respiratory and systemic disease from asymptomatic to critical illness.
Pathogenesis
- Entry: Virus binds ACE2 receptor via spike protein and infects respiratory epithelium.
- Course: Local replication → innate/adaptive immune response; severe cases show hyperinflammation ("cytokine storm").
- Severe effects: ARDS, multiorgan injury and coagulopathy.
Clinical features
- Mild: Fever, cough, fatigue, anosmia, myalgia, sore throat.
- Moderate: Shortness of breath, SpO2 \(90\%\)–\(94\%\).
- Severe: Hypoxia SpO2 \(<90\%\), ARDS, multi‑organ failure, ICU requirement.
- Extra‑respiratory: GI (diarrhoea, nausea), neuro (headache, confusion, anosmia), cardiac (myocarditis), skin (rashes, "COVID toes").
- ARDS definition: Hypoxaemic respiratory failure from hyperinflammation within ~1 week of illness with bilateral opacities on chest imaging.
Risk factors for severe disease
- Age >65, male sex, comorbidities (DM, CKD, COPD, CVD, obesity), immunosuppression, pregnancy (third trimester), unvaccinated.
Investigations
- Microbiology: RT‑PCR from nasopharyngeal swab = gold standard; lateral flow for screening.
- Bloods: Lymphopenia, elevated CRP, raised D‑dimer, mild thrombocytopenia, high ferritin/LDH; troponin if cardiac involvement.
- Other: ABG for hypoxia, CXR (bilateral infiltrates), CT chest (ground‑glass, consolidation), ECG/echo if cardiac signs.
Management overview
- Oxygen targets: maintain SpO2 \(92\%\)–\(96\%\).
- Escalation (stepwise): 1) nasal cannula, 2) face mask, 3) high‑flow nasal oxygen, 4) CPAP, 5) invasive mechanical ventilation.
- First‑line drug therapies: Dexamethasone for patients requiring supplemental oxygen; remdesivir IV for hospitalized patients on oxygen with symptom onset <7 days.
- Second‑line / adjuncts: Tocilizumab for severe systemic inflammation (IL‑6 inhibition); prophylactic LMWH/UFH for hospitalized patients to reduce thrombotic risk.
- Prevention: Vaccination.
Influenza — essentials
- Definition: Acute respiratory infection caused by influenza A or B viruses.
Pathogenesis
- Virus attaches via hemagglutinin to respiratory epithelial cells → replication, cell death and airway inflammation → systemic symptoms from host response.
Clinical features
- Systemic: Fever, chills, myalgia, headache, malaise, fatigue.
- Respiratory: Cough, sore throat, nasal congestion.
- GI: Nausea/vomiting/diarrhoea (less common).
Complications
- Primary viral or secondary bacterial pneumonia, COPD/asthma exacerbation, myocarditis, encephalitis, multi‑organ failure.
Risk factors
- Age >65, pregnancy, chronic cardiorespiratory/hepatic/renal disease, immunocompromise, long‑term care residents.
Investigations
- Clinical diagnosis usually adequate for mild illness; confirm with RT‑PCR on nasopharyngeal swab when important for management.
- FBC/CRP if severe; CXR if suspected pneumonia.
Treatment
- Supportive care: Antipyretics (paracetamol), fluids, rest.
- Antivirals: Oseltamivir (oral) or zanamivir (inhaled) ideally within 48 hours for uncomplicated disease at high risk; give to severe, hospitalized or immunocompromised patients even if beyond 48 hours per clinical judgement.
- Prevention: Annual influenza vaccination (live attenuated for some children, inactivated for adults).
Upper respiratory tract infections (URTIs)
- Definition: Acute infections of the nose, pharynx, larynx or sinuses (above the vocal cords).
Common types
- Common cold, pharyngitis/tonsillitis, laryngitis, sinusitis/rhinosinusitis, otitis media, epiglottitis.
Symptoms
- Nasal congestion/rhinorrhoea, sneezing, sore throat, cough, hoarseness; fever usually low unless bacterial.
- Red flags: Stridor, drooling, severe neck pain/stiffness, high fever, severe pain, signs of airway compromise or immunosuppression — urgent assessment required.
Investigations
- Usually clinical; throat swab for Group A strep (rapid antigen or culture) if bacterial pharyngitis suspected. Nasopharyngeal PCR if testing for influenza/COVID is needed.
Treatment
- Supportive: Rest, fluids, analgesics (paracetamol, ibuprofen), saline nasal spray.
- Antibiotics (when indicated):
- Strep throat (Group A): phenoxymethylpenicillin.
- Bacterial sinusitis or otitis media: amoxicillin.
- Antivirals: Oseltamivir for influenza in high‑risk patients.
Lower respiratory tract infections (LRTIs)
- Definition: Infections below the larynx: trachea, bronchi, bronchioles and lung parenchyma.
Types & common pathogens
- Acute bronchitis / bronchiolitis: usually viral (influenza A/B, RSV, SARS‑CoV‑2, adenovirus, parainfluenza).
- Community‑acquired pneumonia (CAP): Streptococcus pneumoniae, Haemophilus influenzae.
- Healthcare‑associated / hospital‑acquired pneumonia (HAP): Gram‑negative organisms, water‑associated resistant bugs.
- Ventilator‑associated pneumonia (VAP): often multi‑drug resistant organisms.
Symptoms
- Cough, fever, dyspnoea, wheeze, pleuritic chest pain, malaise.
Risk factors
- Smoking, age (<5 or >65), chronic lung disease (COPD, bronchiectasis), diabetes, immunosuppression, recent hospitalization.
Investigations
- Bloods: FBC, CRP, U&E, LFTs; blood cultures and sputum culture if moderate–severe.
- Microbiology: Viral PCR for influenza/COVID when indicated.
- Imaging: CXR to detect consolidation consistent with pneumonia.
Empiric treatment summary
- Acute bronchitis (bacterial suspicion): amoxicillin.
- CAP:
- Mild: amoxicillin.
- Moderate: co‑amoxiclav + doxycycline or clarithromycin.
- Severe: benzylpenicillin + clarithromycin.
- HAP: early onset (<5 days) — co‑amoxiclav or doxycycline; late onset/high‑risk — piperacillin‑tazobactam.
- VAP: piperacillin‑tazobactam; add vancomycin if MRSA risk.
- COPD exacerbation: give antibiotics only if increased sputum purulence/volume and worsened dyspnoea; 1st line doxycycline, 2nd line amoxicillin.
Practical tips for clinical exams
- Triage by oxygen requirement and red flags (airway compromise, sepsis, severe hypoxia).
- Use SpO2 targets and stepwise oxygen escalation to guide immediate management.
- Distinguish URTI vs LRTI by presence of focal consolidation, systemic features and imaging.
- Consider risk factors to decide on antivirals, antibiotics and inpatient care.