Salva il tuo mazzo prima che scompaia
Queste flashcard non sono ancora salvate — spariranno se lasci la pagina. Crea un account gratuito per conservarle e sbloccare tutto quello qui sotto.
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
Why is it important to ensure lower extremity function with epidural anesthesia?
What is Mendelson syndrome associated with in terms of gastric pH and volume?
Why is esophageal disease (e.g., varices) a relative contraindication?
What is the effect of reduced left ventricular (LV) preload on stroke volume?
What causes restricted RV filling during positive pressure inspiration?
How does positive pressure inspiration affect right ventricular (RV) filling?
How does positive pressure inspiration affect left ventricular (LV) filling?
What traditional indicators were once used to assess fluid balance, and what has replaced them?
How does surgery affect fluid retention?
Treatment for non-gap acidosis
What is the treatment for Uremia/drug-induced metabolic acidosis?
What is the caution of NaHCO3 in intracellular acidosis?
Relationship Between CO₂ Production and Ventilation (calculation)
What happens to the chloride shift in the lungs?
What is the chloride (Hamburger) shift?
How are hydrogen ions (H⁺) and bicarbonate ions (HCO₃⁻) buffered during gas exchange in the blood?
What is the normal total plasma magnesium level?
What percentage of total body magnesium is found in extracellular fluid?
Where is the majority of magnesium stored in the body?
What does serum magnesium not reflect?
How does magnesium affect calcium's effects?
What is magnesium essential for in the body?
Why is magnesium critical for cardiac function?
Where is most magnesium reabsorbed in the body?
What is the IV dosage for managing pre-eclampsia with magnesium?
What risk increases with magnesium use beyond 48 hours in pre-eclampsia?
How does magnesium act as an opioid-sparing adjunct?
What condition is magnesium used to treat related to bronchospasm?
What cardiac rhythm disturbances can magnesium help manage?
What can hypermagnesemia enhance?
What should be considered in preeclamptic patients receiving magnesium?
What is the normal blood pH range?
What is acidosis defined as?
What is alkalosis defined as?
What does the Henderson-Hasselbalch equation describe?
What does pKa represent in the Henderson-Hasselbalch equation?
What does [A⁻] represent in the equation?
What does [HA] represent in the equation?
What does PaCO₂ represent in the Henderson-Hasselbalch equation?
What is the normal bicarbonate concentration ([HCO₃⁻])?
What is the normal PaCO₂ level?
What is the pH of blood when substituting normal values into the Henderson-Hasselbalch equation?
What does the 0.03 in the Henderson-Hasselbalch equation refer to?
What is the major by-product of aerobic metabolism?
How is most CO₂ buffered in the blood?
What percentage of CO₂ is transported as bicarbonate?
What percentage of CO₂ is bound to hemoglobin?
What percentage of CO₂ is dissolved in plasma?
How does venous blood PvCO₂ compare to arterial blood PaCO₂?
What is the arterial pH?
What is the venous pH?
What is the Bohr effect?
What is the Haldane effect?
How is CO₂ removed from the body?
What happens to pulmonary blood pH as CO₂ is eliminated?
What is the CO₂ transport reaction?
What enzyme is essential for the CO₂ transport reaction?
Where is carbonic anhydrase found?
What does carbonic anhydrase catalyze?
What does carbonic acid quickly dissociate into?
What maintains electrical neutrality in erythrocytes?
What happens to erythrocytes in venous circulation due to Cl⁻?
What is the normal range for PaCO₂?
What indicates a respiratory disorder?
What indicates respiratory acidosis?
What indicates respiratory alkalosis?
What is the normal range for HCO₃⁻?
What indicates a metabolic disorder?
What indicates metabolic acidosis?
What indicates metabolic alkalosis?
What is the normal range for the anion gap?
What does the ROME mnemonic stand for?
What is full compensation?
What is partial compensation?
What is respiratory compensation?
What is metabolic compensation?
What indicates a mixed disorder?
What should you check if PaO₂ is normal?
What is the A-a gradient used for?
What causes respiratory acidosis?
What is the treatment focus for respiratory acidosis?
When is mechanical ventilation indicated for respiratory acidosis?
What is hypercapnia?
What is hypocapnia?
How do kidneys compensate for respiratory acidosis?
How long does full compensation for respiratory acidosis take?
What causes respiratory alkalosis?
What are the common causes of respiratory alkalosis?
How do kidneys compensate for respiratory alkalosis?
What is the primary goal in treating respiratory alkalosis?
What are the causes of metabolic acidosis?
What is the Anion Gap formula?
What is the normal range for Anion Gap?
What is the difference between gap and non-gap acidosis?
How does the body compensate for metabolic acidosis?
What is the Respiratory Compensation Rule?
When is sodium bicarbonate used in anion gap acidosis?
What is the treatment for lactic acidosis?
What is the treatment for DKA?
What causes metabolic alkalosis?
How does the body compensate for metabolic alkalosis?
How does PaCO₂ change with each 1 mEq/L rise in HCO₃⁻?
What is the first step in treating metabolic alkalosis?
What is acetazolamide used for in metabolic alkalosis?
What role does spironolactone play in metabolic alkalosis?
What is the treatment for severe or refractory cases of metabolic alkalosis?
What is the 4:2:1 Rule for fluid maintenance?
How do you calculate the estimated fluid deficit?
What is the fluid replacement for very minimal trauma?
What is the fluid replacement for minimal trauma?
What is the fluid replacement for moderate trauma?
What is the fluid replacement for severe trauma?
What is the crystalloid replacement ratio for blood loss?
What is the colloid/blood replacement ratio for blood loss?
What is the maintenance IV fluid rate for a 17 kg patient?
What is the maintenance IV fluid rate for an 8 kg patient?
What is the maintenance IV fluid rate for a 120 kg patient?
What misconception existed about preoperative fasting?
What is the issue with 'third space' fluid loss?
What is the current practice for blood loss replacement?
What was the historical approach to managing post-induction hypotension?
Why is urine output unreliable during surgery?
What are the limitations of using filling pressures?
What is the primary goal of goal-directed fluid therapy?
What does the Frank-Starling mechanism describe?
What happens with excessive volume in the heart?
What is the risk of both under- and over-resuscitation?
What does reduced cross-bridges lead to?
What is required to measure volume directly?
What influences filling pressure?
What conditions alter compliance?
What does contractility reflect?
Is contractility dependent on preload and afterload?
What happens to output with increased contractility?
What happens to output with decreased contractility?
What does Starling's Law state?
Is increasing preload the same as increasing contractility? (Regarding Starling's Law)
What is the goal of Goal-Directed Fluid Management?
What do small fluid boluses help assess?
What can fluid status do during surgery?
What are dynamic indicators of preload responsiveness?
What can a small bolus do in patients with poor cardiac function?
What do patients on the lower part of the Starling curve experience?
What does enhanced stretch lead to?
What is the state of patients who are volume responsive?
What does the plateau region of the Starling curve indicate?
What happens if more fluid is given during preload independence?
What are the consequences of excessive preload?
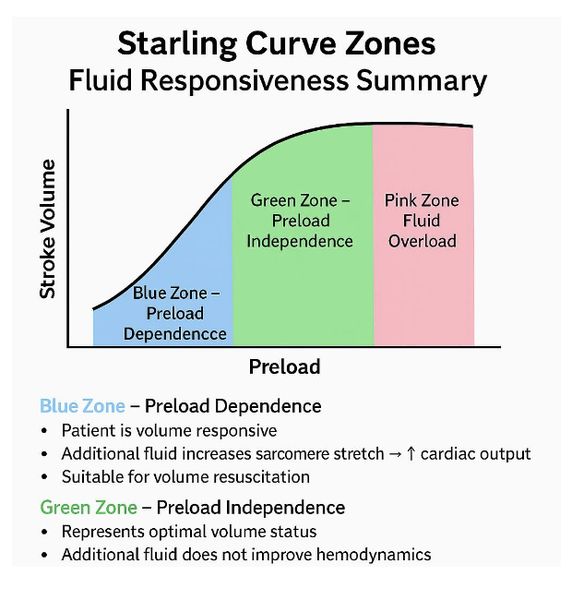
What is the blue zone on the Starling curve?
What is the green zone on the Starling curve?
What is the pink zone on the Starling curve?
What does advanced monitoring enhance?
What do most monitoring devices use for calculations?
What is pulse pressure variation derived from?
What does pulse pressure variation measure?
What does pulse contour analysis assess?
What does pulse contour analysis assume about the patient?
What does preload responsiveness assess?
How does intra-thoracic pressure affect stroke volume?
What does increased LV preload lead to?
What happens to LV filling during expiration?
What is pulmonary transit time?
What indicates a patient may need more fluid?
What fluid bolus increase indicates preload responsiveness?
What pulse contour indices suggest volume responsiveness?
What conditions affect pulse contour analysis accuracy? (limitations)
What is the role of esophageal Doppler?
How is the esophageal Doppler probe positioned?
What does the esophageal Doppler measure?
What are key points of esophageal Doppler waveform analysis?
What conditions limit the accuracy of esophageal Doppler?
What indicates optimal fluid administration on the Starling curve?
What should be done if SV changes by less than 10%?
What is the origin of Enhanced Recovery After Surgery (ERAS)?
What is the aim of ERAS programs?
What are the core goals of ERAS?
What is a key note on ERAS implementation?
What is a notable guideline in ERAS?
What is the benefit of allowing clear fluids preoperatively?
What is the risk associated with gastric pH < 2.5 and volume > 25 mL?
What type of fluids are encouraged preoperatively (2 hours before)?
What are the benefits of carbohydrate-rich fluids before surgery?
What should be ensured when using epidural anesthesia?
What happens to the P50 curve during hypoxemia?




































Flashcards in this deck (202)
-
Why is it important to ensure lower extremity function with epidural anesthesia?
It facilitates early ambulation, supporting faster recovery.
-
What is Mendelson syndrome associated with in terms of gastric pH and volume?
Gastric pH < 2.5 and volume > 25 mL or 0.4 mL/kg.
-
Why is esophageal disease (e.g., varices) a relative contraindication?
Because it increases the risk of traumatic esophageal injury.
-
What is the effect of reduced left ventricular (LV) preload on stroke volume?
Reduced LV preload leads to a decrease in stroke volume.
-
What causes restricted RV filling during positive pressure inspiration?
Pulmonary vein compression and increased pleural pressure.
-
How does positive pressure inspiration affect right ventricular (RV) filling?
It restricts right ventricular (RV) filling due to pulmonary vein compression and increased pleural pressure.
-
How does positive pressure inspiration affect left ventricular (LV) filling?
It enhances left ventricular (LV) filling.
-
What traditional indicators were once used to assess fluid balance, and what has replaced them?
Traditional indicators included heart rate, MAP (mean arterial pressure), and CVP (central venous pressure). These have been replaced by dynamic measures of fluid responsiveness.
-
How does surgery affect fluid retention?
ADH (antidiuretic hormone) is released during surgery, causing fluid retention for several days.
-
Treatment for non-gap acidosis
• Sodium bicarbonate is more commonly used
• Most causes involve bicarbonate loss
-
What is the treatment for Uremia/drug-induced metabolic acidosis?
Dialysis
-
What is the caution of NaHCO3 in intracellular acidosis?
Caution: NaHCO₃ may worsen intracellular acidosis if ventilation
or perfusion is inadequate
-
Relationship Between CO₂ Production and Ventilation (calculation)
PaCO₂ = CO₂ Production ÷ Alveolar Ventilation
-
What happens to the chloride shift in the lungs?
The chloride shift reverses—Cl⁻ exits erythrocytes as CO₂ is exhaled and HCO₃⁻ re-enters the cell.
-
What is the chloride (Hamburger) shift?
The chloride shift refers to Cl⁻ entering erythrocytes to maintain electrical neutrality as bicarbonate (HCO₃⁻) exits the cell. In the lungs, the shift reverses as CO₂ is exhaled.
-
How are hydrogen ions (H⁺) and bicarbonate ions (HCO₃⁻) buffered during gas exchange in the blood?
H⁺ is buffered by hemoglobin; HCO₃⁻ is transported into plasma as a buffer.
-
What is the normal total plasma magnesium level?
1.7–2.4 mg/dL (1.5–2.1 mEq/L)
magnesium plasma -
What percentage of total body magnesium is found in extracellular fluid?
1% (0.3% in plasma)
magnesium body -
Where is the majority of magnesium stored in the body?
Intracellularly (muscle and bone)
magnesium storage -
What does serum magnesium not reflect?
Total body magnesium stores
magnesium serum -
How does magnesium affect calcium's effects?
Counteracts calcium’s effects
magnesium calcium -
What is magnesium essential for in the body?
DNA synthesis and enzymatic reactions
magnesium biochemistry -
Why is magnesium critical for cardiac function?
It supports normal cardiac function
magnesium cardiology -
Where is most magnesium reabsorbed in the body?
In the renal tubules
magnesium renal -
What is the IV dosage for managing pre-eclampsia with magnesium?
4 g IV over 10–15 minutes, then 1 g/hr for 24 hours
magnesium preeclampsia -
What risk increases with magnesium use beyond 48 hours in pre-eclampsia?
Neonatal respiratory depression, hypotension, and lethargy (mag crosses placenta)
magnesium risks -
How does magnesium act as an opioid-sparing adjunct?
Through NMDA receptor antagonism
magnesium opioids -
What condition is magnesium used to treat related to bronchospasm?
Acute bronchospasm
magnesium bronchospasm -
What cardiac rhythm disturbances can magnesium help manage?
Symptomatic PVCs and Torsades de pointes
magnesium cardiac -
What can hypermagnesemia enhance?
Neuromuscular blockade effects (succinylcholine and nondepolarizing agents)
magnesium hypermagnesemia -
What should be considered in preeclamptic patients receiving magnesium?
Caution with emergent C-sections
magnesium preeclampsia -
What is the normal blood pH range?
7.35 – 7.45
acid-base ph -
What is acidosis defined as?
pH < 7.35
acid-base acidosis -
What is alkalosis defined as?
pH > 7.45
acid-base alkalosis -
What does the Henderson-Hasselbalch equation describe?
pH as a function of the ratio of [A⁻] to [HA]
acid-base equation -
What does pKa represent in the Henderson-Hasselbalch equation?
Negative log of the acid dissociation constant
acid-base pka -
What does [A⁻] represent in the equation?
Concentration of the conjugate base (e.g., bicarbonate HCO₃⁻)
acid-base conjugate_base -
What does [HA] represent in the equation?
Concentration of the weak acid (e.g., carbonic acid H₂CO₃)
acid-base weak_acid -
What does PaCO₂ represent in the Henderson-Hasselbalch equation?
Partial pressure of CO₂ in arterial blood
acid-base paco2 -
What is the normal bicarbonate concentration ([HCO₃⁻])?
24 mEq/L
acid-base bicarbonate -
What is the normal PaCO₂ level?
40 mmHg
acid-base paco2 -
What is the pH of blood when substituting normal values into the Henderson-Hasselbalch equation?
7.4
acid-base ph -
What does the 0.03 in the Henderson-Hasselbalch equation refer to?
Solubility coefficient of CO₂ in plasma
Specifically: It represents how much dissolved CO₂ is present in blood plasma per mmHg of PCO₂.
acid-base solubility -
What is the major by-product of aerobic metabolism?
CO₂, diffusing into capillary blood.
biology metabolism -
How is most CO₂ buffered in the blood?
A small amount dissolves in plasma.
biology blood -
What percentage of CO₂ is transported as bicarbonate?
70%
biology transport -
What percentage of CO₂ is bound to hemoglobin?
23%
biology hemoglobin -
What percentage of CO₂ is dissolved in plasma?
7%
biology plasma -
How does venous blood PvCO₂ compare to arterial blood PaCO₂?
PvCO₂ is ~5 mmHg higher than PaCO₂.
physiology blood -
What is the arterial pH?
7.40
physiology ph -
What is the venous pH?
7.36
physiology ph -
What is the Bohr effect?
Acidic environments enhance O₂ offloading from hemoglobin.
physiology bohr_effect -
What is the Haldane effect?
Acidic environments increase CO₂ binding to hemoglobin.
physiology haldane_effect -
How is CO₂ removed from the body?
Via alveolar ventilation.
physiology co2_removal -
What happens to pulmonary blood pH as CO₂ is eliminated?
It rises. This facilitates CO₂ offloading from hemoglobin.
physiology ph -
What is the CO₂ transport reaction?
H₂O + CO₂ ⇌ H₂CO₃ ⇌ H⁺ + HCO₃⁻
chemistry transport_reaction -
What enzyme is essential for the CO₂ transport reaction?
Carbonic anhydrase.
biochemistry enzymes -
Where is carbonic anhydrase found?
Inside RBCs, not in plasma.
biology carbonic_anhydrase -
What does carbonic anhydrase catalyze?
Formation of carbonic acid from H₂O and CO₂.
biochemistry catalysis -
What does carbonic acid quickly dissociate into?
H⁺ and HCO₃⁻.
chemistry dissociation -
What maintains electrical neutrality in erythrocytes?
Cl⁻ enters erythrocytes (Chloride shift).
physiology chloride_shift -
What happens to erythrocytes in venous circulation due to Cl⁻?
They swell, increasing venous hematocrit by ~3% higher than arterial hematocrit (swelling process reverses in the lungs).
physiology hematocrit -
What is the normal range for PaCO₂?
35 – 45 mmHg
physiology paco2 -
What indicates a respiratory disorder?
pH and PaCO₂ move in opposite directions.
physiology respiratory_disorder -
What indicates respiratory acidosis?
↓ pH, ↑ CO₂
physiology respiratory_acidosis -
What indicates respiratory alkalosis?
↑ pH, ↓ CO₂
physiology respiratory_alkalosis -
What is the normal range for HCO₃⁻?
22 – 26 mEq/L
physiology hco3 -
What indicates a metabolic disorder?
pH and HCO₃⁻ move in the same direction.
physiology metabolic_disorder -
What indicates metabolic acidosis?
↓ pH, ↓ HCO₃⁻
physiology metabolic_acidosis -
What indicates metabolic alkalosis?
↑ pH, ↑ HCO₃⁻
physiology metabolic_alkalosis -
What is the normal range for the anion gap?
8–12 mEq/L
physiology anion_gap -
What does the ROME mnemonic stand for?
Respiratory Opposite, Metabolic Equal.
physiology mnemonics -
What is full compensation?
pH is fully restored to normal.
physiology compensation -
What is partial compensation?
pH improves but remains outside the normal range.
physiology compensation -
What is respiratory compensation?
Rapid changes driven by ventilation. (respiratory compensation to the kidneys is slow)
physiology compensation -
What is metabolic compensation?
Slow changes due to altered H⁺ excretion by kidneys. (metabolic changes driven by changes in ventilation is fast)
physiology compensation -
What indicates a mixed disorder?
Suspect mixed if:
- PaCO₂ or HCO₃⁻ are abnormal but compensation is inadequate.
- Both PaCO₂ and HCO₃⁻ shift toward acidosis or alkalosis.
physiology mixed_disorder -
What should you check if PaO₂ is normal?
Calculate the A-a gradient to assess for a shunt.
physiology pao2 -
What is the A-a gradient used for?
To assess for a shunt and its severity.
physiology shunt -
What causes respiratory acidosis?
- Increased CO₂ production
- Decreased CO₂ elimination
- Rebreathing exhaled gases
• Occurs when alveolar ventilation cannot keep up with CO₂ production.
respiratory acidosis -
What is the treatment focus for respiratory acidosis?
Correcting the underlying cause.
treatment respiratory acidosis -
When is mechanical ventilation indicated for respiratory acidosis?
If pH < 7.20.
treatment ventilation acidosis -
What is hypercapnia?
PaCO₂ > 45 mmHg.
physiology gas_exchange -
What is hypocapnia?
PaCO₂ < 35 mmHg.
physiology gas_exchange -
How do kidneys compensate for respiratory acidosis?
- Excrete hydrogen ions (H⁺)
- Retain bicarbonate (HCO₃⁻)
- Starts within a few hours, full compensation may take a few days
compensation respiratory acidosis -
How long does full compensation for respiratory acidosis take?
Several days.
compensation respiratory acidosis -
What causes respiratory alkalosis?
Alveolar ventilation exceeds CO₂ production.
respiratory alkalosis -
What are the common causes of respiratory alkalosis?
- Iatrogenic- Mechanical ventilation (most common cause)
- Hypoxia
- Pain
- Anxiety
- Pregnancy
- Medications
- Pulmonary embolism
- Reduced mechanical dead space (removing HME or switching from mask to ETT)
causes respiratory alkalosis -
How do kidneys compensate for respiratory alkalosis?
Excrete bicarbonate (HCO₃⁻).
compensation respiratory alkalosis -
What is the primary goal in treating respiratory alkalosis?
Identify and correct the underlying cause.
treatment respiratory alkalosis -
What are the causes of metabolic acidosis?
- Build-up of nonvolatile acids
- Bicarbonate loss
- Large-volume resuscitation with normal saline
causes metabolic acidosis -
What is the Anion Gap formula?
Anion Gap = Na⁺ - (Cl⁻ + HCO₃⁻)
• Helps identify the underlying cause of metabolic acidosis
diagnostic metabolic acidosis -
What is the normal range for Anion Gap?
8–12 mEq/L.
diagnostic metabolic acidosis -
What is the difference between gap and non-gap acidosis?
- Gap Acidosis: Acid accumulation
- Non-Gap Acidosis: Bicarbonate loss or ECF dilution
types metabolic acidosis -
How does the body compensate for metabolic acidosis?
By increasing minute ventilation to eliminate CO₂.
compensation metabolic acidosis -
What is the Respiratory Compensation Rule?
PaCO₂ decreases by 1–1.5 mmHg for every 1 mEq/L drop in HCO₃⁻.
compensation metabolic acidosis -
When is sodium bicarbonate used in anion gap acidosis?
If pH < 7.2 and patient is hemodynamically unstable.
• Bicarbonate may help when acidosis impairs enzyme function
treatment metabolic acidosis -
What is the treatment for lactic acidosis?
IVF, oxygen, cardiopulmonary support.
treatment metabolic acidosis -
What is the treatment for DKA?
IVF, insulin.
treatment metabolic acidosis -
What causes metabolic alkalosis?
- Excess bicarbonate accumulation
- Loss of nonvolatile acids (e.g., gastric acid)
causes metabolic alkalosis -
How does the body compensate for metabolic alkalosis?
By retaining CO₂ through decreased ventilation.
compensation metabolic alkalosis -
How does PaCO₂ change with each 1 mEq/L rise in HCO₃⁻?
Increases by 0.5–1 mmHg for every 1 mEq/L rise in HCO₃⁻
compensation metabolic alkalosis -
What is the first step in treating metabolic alkalosis?
Address the underlying cause
treatment alkalosis -
What is acetazolamide used for in metabolic alkalosis?
Promotes renal bicarbonate excretion (carbonic anhydrase inhibitor)
treatment medication -
What role does spironolactone play in metabolic alkalosis?
Acts as a mineralocorticoid antagonist
treatment medication -
What is the treatment for severe or refractory cases of metabolic alkalosis?
Dialysis
treatment alkalosis -
What is the 4:2:1 Rule for fluid maintenance?
4 mL/kg/hr for first 10 kg of body weight, 2 mL/kg/hr for second 10 kg, 1 mL/kg/hr each kg thereafter 20 kg
for adults: body wt (kg) + 40 ml/hr
fluid_management maintenance -
How do you calculate the estimated fluid deficit?
Fasting hours × Hourly maintenance rate
fluid_management calculation -
What is the fluid replacement for very minimal trauma?
1–2 mL/kg/hr
• e.g., Orofacial surgery
fluid_management trauma -
What is the fluid replacement for minimal trauma?
2–4 mL/kg/hr
• e.g., Inguinal hernia repair
fluid_management trauma -
What is the fluid replacement for moderate trauma?
4–6 mL/kg/hr
• e.g., Major nonabdominal surgery
fluid_management trauma -
What is the fluid replacement for severe trauma?
6–8 mL/kg/hr
• e.g., Major abdominal surgery
fluid_management trauma -
What is the crystalloid replacement ratio for blood loss?
3:1 (3 mL crystalloid per 1 mL blood lost)
fluid_management blood_loss -
What is the colloid/blood replacement ratio for blood loss?
1:1 (1 mL per 1 mL blood lost)
fluid_management blood_loss -
What is the maintenance IV fluid rate for a 17 kg patient?
- 4 mL/kg/hr for the first 10 kg = 40 ml
- 2 mL/kg/hr for the second 10 kg = 14 mL
- 1 mL/kg/hr for each subsequent kg
- Answer = 54 mL/hr
fluid_management iv_rate -
What is the maintenance IV fluid rate for an 8 kg patient?
4 mL/kg/hr for the first 10 kg = 40 mlAnswer = 32 mL/hr
fluid_management iv_rate -
What is the maintenance IV fluid rate for a 120 kg patient?
Body weight (120 kg) + 40 mL
Answer = 160 mL/hr
fluid_management iv_rate -
What misconception existed about preoperative fasting?
Thought to cause dehydration, but intravascular volume remains mostly unaffected
• Patients can now drink clear fluids up to 2 hours before surgery
fluid_management misconception -
What is the issue with 'third space' fluid loss?
Minimal evidence supports its significance; may lead to excessive fluid administration
fluid_management misconception -
What is the current practice for blood loss replacement?
Guide replacement by fluid responsiveness
fluid_management blood_loss -
What was the historical approach to managing post-induction hypotension?
Managed with fluid, but often caused by vasodilation, better treated with vasopressors
fluid_management hypotension -
Why is urine output unreliable during surgery?
ADH limits urine output, making it unreliable during surgery
fluid_management urine_output -
What are the limitations of using filling pressures?
TEE is required to measure volume directly; filling pressures are surrogates
fluid_management limitations -
What is the primary goal of goal-directed fluid therapy?
Optimize oxygen delivery
fluid_management goal-directed -
What does the Frank-Starling mechanism describe?
Increased preload boosts cardiac output up to a plateau
physiology frank-starling -
What happens with excessive volume in the heart?
Overstretches sarcomeres, fewer cross bridges, leading to reduced output
physiology frank-starling -
What is the risk of both under- and over-resuscitation?
Can impair oxygen delivery
fluid_management risks -
What does reduced cross-bridges lead to?
Reduced output
physiology cardiology -
What is required to measure volume directly?
TEE (Transesophageal Echocardiography)
cardiology monitoring -
What influences filling pressure?
Ventricular compliance, Filling pressure ≠ volume
physiology cardiology -
What conditions alter compliance?
Ischemia or hypertrophy
cardiology pathology -
What does contractility reflect?
Myocardium's ability to shorten and generate force
physiology cardiology -
Is contractility dependent on preload and afterload?
No, it is independent
physiology cardiology -
What happens to output with increased contractility?
Output increases
physiology cardiology -
What happens to output with decreased contractility?
Output decreases
physiology cardiology -
What does Starling's Law state?
↑ Preload → ↑ Contraction force
• This is NOT the same as increasing contractility
physiology cardiology -
Is increasing preload the same as increasing contractility? (Regarding Starling's Law)
No, they are not the same
physiology cardiology -
What is the goal of Goal-Directed Fluid Management?
Optimize patient’s position on the Starling Curve
management cardiology -
What do small fluid boluses help assess?
Preload dependence vs. independence (200–250 mL)
management cardiology -
What can fluid status do during surgery?
Shift rapidly
surgery monitoring -
What are dynamic indicators of preload responsiveness?
Pulse contour analysis, Esophageal Doppler
monitoring cardiology -
What can a small bolus do in patients with poor cardiac function?
Shift from preload independence, lead to pulmonary edema
management cardiology -
What do patients on the lower part of the Starling curve experience?
Respond to fluid with increased sarcomere stretch
physiology cardiology -
What does enhanced stretch lead to?
More cross-bridge formation → greater cardiac output
• These patients are considered "volume responsive"
physiology cardiology -
What is the state of patients who are volume responsive?
Preload dependence, suitable candidates for fluid resuscitation
management cardiology -
What does the plateau region of the Starling curve indicate?
Optimal volume status
physiology cardiology -
What happens if more fluid is given during preload independence?
Unlikely to enhance cardiac output or oxygen delivery, excess fluid may be harmful, pushing the patient further along the curve and worsening outcomes
management cardiology -
What are the consequences of excessive preload?
Reduced myocardial efficiency, risk of pulmonary edema and congestive heart failure
pathology cardiology -
What is the blue zone on the Starling curve?
- Preload dependence, patient is volume responsive
- Additional fluid increases sarcomere stretch → ↑ cardiac output
- Suitable for volume resuscitation
 physiology cardiology
physiology cardiology -
What is the green zone on the Starling curve?
- Preload independence, optimal volume status
- Additional fluid does not improve hemodynamics
- Risk of harm if more fluid is given
physiology cardiology -
What is the pink zone on the Starling curve?
- Fluid overload, excess preload impairs myocardial function
- ↑ Risk of pulmonary edema and congestive heart failure
pathology cardiology -
What does advanced monitoring enhance?
Assessment of fluid responsiveness, oxygen delivery, microcirculatory flow
monitoring technology -
What do most monitoring devices use for calculations?
Arterial or SpO₂ waveforms
monitoring technology -
What is pulse pressure variation derived from?
The arterial waveform
monitoring cardiology -
What does pulse pressure variation measure?
Max and min pulse pressure across the respiratory cycle
Calculates the percentage change → used to guide fluid management
monitoring cardiology -
What does pulse contour analysis assess?
Changes in stroke volume during the respiratory cycle
monitoring cardiology -
What does pulse contour analysis assume about the patient?
Patient is on positive pressure ventilation (PPV)
monitoring cardiology -
What does preload responsiveness assess?
Changes in stroke volume during the respiratory cycle
physiology hemodynamics -
How does intra-thoracic pressure affect stroke volume?
It changes stroke volume during positive pressure ventilation
physiology hemodynamics -
What does increased LV preload lead to?
Increased stroke volume via the Frank-Starling mechanism
physiology cardiology -
What happens to LV filling during expiration?
LV filling decreases due to reduced RV preload from prior cardiac cycles
physiology cardiology -
What is pulmonary transit time?
Delay in LV filling due to previous cardiac cycles
(Left ventricular (LV) filling decreases due to reduced right ventricular (RV) preload from prior cardiac cycles)
physiology cardiology -
What indicates a patient may need more fluid?
Greater stroke volume variation during the respiratory cycle, caused by changes in intrathoracic pressure affecting RV filling
physiology hemodynamics -
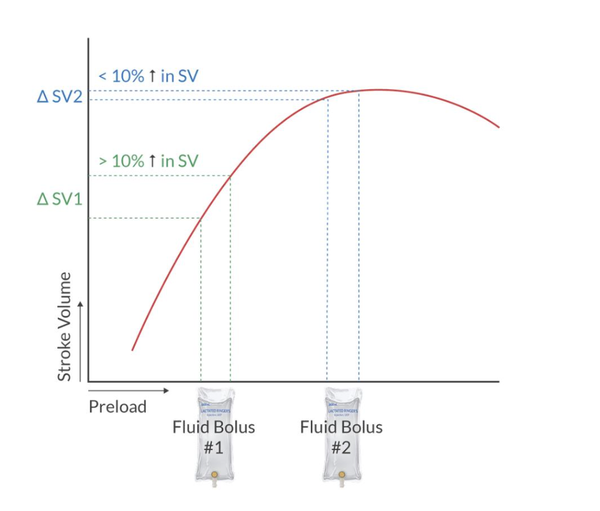
What fluid bolus increase indicates preload responsiveness?
200–250 mL increases stroke volume (SV) > 10%
physiology hemodynamics -
What pulse contour indices suggest volume responsiveness?
PVI, SVV, SPV, PPV suggest volume responsiveness when: Values greater than 13–15%
physiology hemodynamics -
What conditions affect pulse contour analysis accuracy? (limitations)
Spontaneous breathing, low tidal volumes, PEEP, open chest procedures, RV dysfunction, cardiac dysrhythmias
physiology hemodynamics -
What is the role of esophageal Doppler?
Point-of-care hemodynamic assessment, less invasive tool for fluid management
physiology hemodynamics -
How is the esophageal Doppler probe positioned?
Insert ~35 cm from incisors, aligns with T5–T6 or third sternocostal junction
physiology hemodynamics -
What does the esophageal Doppler measure?
Blood flow velocity and aortic diameter
physiology hemodynamics -
What are key points of esophageal Doppler waveform analysis?
Includes examples of waveform changes and interventions
physiology hemodynamics -
What conditions limit the accuracy of esophageal Doppler?
Aortic stenosis, insufficiency, thoracic aortic disease, aortic cross-clamping, CPB, pregnancy
physiology hemodynamics -
What indicates optimal fluid administration on the Starling curve?
SV increases by more than 10% after fluid bolus
 physiology hemodynamics
physiology hemodynamics -
What should be done if SV changes by less than 10%?
Consider other measures like vasoactive drugs
physiology hemodynamics -
What is the origin of Enhanced Recovery After Surgery (ERAS)?
Originally developed for colon surgery
surgery eras -
What is the aim of ERAS programs?
To improve postsurgical outcomes through standardized perioperative care
surgery eras -
What are the core goals of ERAS?
- Reduce physiological stress of surgery
- Limit fluid shifts
- Support nutritional recovery
- Enhance pain control
- Promote patient education
surgery eras -
What is a key note on ERAS implementation?
Protocols vary by institution, but core elements are widely shared
surgery eras -
What is a notable guideline in ERAS?
Allowing clear fluids up to 2 hours before surgery
surgery eras -
What is the benefit of allowing clear fluids preoperatively?
- Improves hemodynamic stability (↓ risk of intraoperative hypotension)
- Lowers gastric volume and raises gastric pH
- Decreases risk of Mendelson syndrome
surgery eras -
What is the risk associated with gastric pH < 2.5 and volume > 25 mL?
Risk of Mendelson syndrome
surgery eras -
What type of fluids are encouraged preoperatively (2 hours before)?
Carbohydrate-rich fluids (e.g., Gatorade)
surgery eras -
What are the benefits of carbohydrate-rich fluids before surgery?
Helps maintain glucose and insulin levels, blunts stress response, provides same benefits as clear fluids
surgery eras -
What should be ensured when using epidural anesthesia?
Lower extremity function must be intact
surgery anesthesia -
What happens to the P50 curve during hypoxemia?
Shifts to the right, releases more O₂ to tissues
physiology oxygen -
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-