Save your deck before it's gone
These flashcards aren't stored yet — they'll disappear when you leave. Create a free account to keep them, and unlock everything below.
- Save this deck to your account
- Study with spaced repetition
- Export to Anki (.apkg) or PDF
- Process documents up to 100 pages
- Images extracted from your PDFs
- Sharper text extraction & a more advanced AI model
Name the major structures shown in a sagittal view of the kidney.
What are the primary learning goals regarding diuretic classes in this review?
What clinical decisions should be identified for each diuretic class?
What adverse effects must be evaluated for each diuretic class?
What should an anesthesia plan incorporate for patients taking diuretics?
How many times per day does the kidney filter the extracellular fluid volume (ECV) across the renal glomeruli?
What are the primary regulatory functions of nephrons?
What are the main anatomical segments of a nephron?
Which blood vessels are directly associated with the nephron's blood supply?
Describe the path urine takes from the nephron to the ureter.
Name the major renal vessels and structural parts shown in the kidney diagram.
What structure surrounds the glomerulus in the nephron?
What is the primary pharmacologic effect of diuretics?
By what general mechanism do most diuretics act within the nephron?
What are common clinical indications for diuretic use?
Which diuretic classes act at these nephron sites: proximal convoluted tubule, loop of Henle, distal convoluted tubule, and collecting duct?
Which diuretic classes and related agents are depicted in the nephron diagram?
Which hormone is shown in the diagram as relevant to renal water handling?
Which nephron segment is highlighted as the site of carbonic anhydrase action?
Which nephron segment is highlighted for the action of osmotic diuretics?
What general nephron features does the diagram indicate relevant to diuretic pharmacology?
Where in the nephron is carbonic anhydrase activity primarily described in the text?
What is the role of the Na+/H+ exchanger in the renal tubule as described?
Write the sequence of reactions involving bicarbonate and carbonic acid described in the text.
According to the text, which molecule crosses the tubular cell membrane during bicarbonate handling?
What happens to carbonic acid within tubular cells and how are the products handled?
What is the amount of acetazolamide per vial for injection labelled in the material?
To which drug class does acetazolamide belong?
What is the mechanism of enzyme inhibition of acetazolamide?
Which nephron segment is primarily affected by acetazolamide's diuretic action?
What reabsorptions are decreased by acetazolamide in the kidney?
Show the vial image of acetazolamide for intravenous use.
Where in the nephron does acetazolamide primarily act?
What is the mechanism of action of acetazolamide and its immediate effects on ion transport in the proximal tubule?
What are the primary clinical applications of acetazolamide (diamox)?
Which enzyme is present in the ciliary process of the eye involved in aqueous humor production?
What is the effect of inhibiting carbonic anhydrase in the ciliary process on aqueous humor and intraocular pressure (IOP)?
What major structural damage can result from buildup of aqueous humor fluid in glaucoma?
What is 'Pseudotumor cerebri' (Idiopathic Intracranial Hypertension)?
What does the mnemonic 'HEAD PRESS' summarize for Idiopathic Intracranial Hypertension?
What key diagnostic combination defines Idiopathic Intracranial Hypertension?
What are the main treatments for Idiopathic Intracranial Hypertension?
What is 'acute high-altitude illness' (AHAI) or 'acute mountain sickness' (AMS)?
What is the primary initial physiological response to hypoxia at high altitude?
Describe the ventilatory chemical sequence that can follow hypoxia at high altitude.
How can metabolic acidosis affect ventilation in high-altitude illness?
What drug is described as the cornerstone of therapy for acute high-altitude illness?
What is Acute Mountain Sickness (AMS) primarily associated with?
What cognitive or neuroimaging changes occur above 7000 m?
At what altitude do about 32% of climbers experience hallucinations?
Name some detectable psychomotor or cognitive impairments at high altitude (examples from the diagram).
What altitude equivalent are commercial aircraft typically pressurised to?
What is the pharmacokinetic property of carbonic anhydrase (CA) inhibitors regarding excretion?
How should dosing of CA inhibitors be adjusted for elderly patients and those with chronic renal impairment (CRI)?
Should CA inhibitors be used in patients with severe chronic renal impairment (CRI)?
What is the primary pharmacodynamic effect of CA inhibitors on bicarbonate and urine pH?
What type of metabolic acidosis do CA inhibitors cause and what ion change accompanies it?
What are the effects of CA inhibitors on natriuresis and potassium balance?
Is long-term administration of CA inhibitors considered a problem according to the notes?
What are common side effects of carbonic anhydrase inhibitors?
Which diuretic class is shown?
Where do loop diuretics act in the nephron?
Which transport protein is inhibited by loop diuretics?
Which ions' reabsorption is inhibited by loop diuretics?
What proportion of filtered sodium is reabsorbed in the thick ascending limb?
Is the thick ascending limb of the Loop of Henle permeable to water?
What are two main physiological effects of diuresis from loop diuretics?
What is the relative potency of loop diuretics among diuretic classes?
How does response to loop diuretics change with dose?
What is the first-line indication for loop diuretics related to fluid overload?
Are loop diuretics first-line for treating hypertension in patients with normal kidney function?
Which transporter in the thick ascending limb is inhibited by loop diuretics?
What fraction of filtered sodium is normally reabsorbed in the loop of Henle?
How do loop diuretics affect divalent cation reabsorption (Ca2+, Mg2+)?
What acid-base and potassium disturbance is associated with loop diuretics?
Why do loop diuretics cause increased K+ loss in the collecting duct?
What class of diuretic is furosemide?
How does furosemide affect cerebrospinal fluid (CSF) and intracranial pressure (ICP)?
Can alterations in the blood-brain barrier (BBB) change furosemide's effect on ICP?
In what ways can furosemide be administered for ICP reduction?
What are furosemide's oral absorption and protein binding characteristics?
What is the elimination half-life and typical dose range of furosemide?
What is the onset time of intravenous furosemide?
What is the peak effect time of furosemide?
What is the duration of action (DOA) of furosemide?
What is the elimination half-life of furosemide?
How is furosemide excreted?
What is the usual IV dose of furosemide in normal renal function and the typical range for renal insufficiency?
Is there benefit to giving more than 200 mg of furosemide IV?
What ototoxic adverse effect can occur if furosemide is administered too quickly?
Relative potency: how potent is bumetanide compared with furosemide?
Key pharmacokinetics and usual dose for bumetanide (Bumex)?
Core properties and starting dose for torsemide (Demadex)?
What is a key chemical characteristic of ethacrynic acid (Edecrin)?
How does the potency of ethacrynic acid compare to furosemide?
What is the usual dose range for ethacrynic acid?
What are the notable adverse effects of ethacrynic acid?
What are the main fluid/electrolyte and metabolic side effects of loop diuretics?
What is the 'braking phenomenon' with loop diuretics and what causes acute versus chronic tolerance?
What ototoxicity risks are associated with loop diuretics?
Do loop diuretics have cross reactivity concerns with sulfa allergy?
How do loop diuretics interact with nondepolarizing neuromuscular blocking agents (NMBAs)?
What is the primary mechanism of action of thiazide diuretics?
At which nephron segment do thiazide diuretics act?
Which major electrolyte changes do thiazide diuretics cause in urine and blood?
What are the early and sustained physiological effects of thiazide diuretics?
What is the primary antihypertensive indication for thiazide diuretics?
How are thiazide diuretics commonly used in relation to other antihypertensives?
Name two cardiovascular or fluid-overload conditions treated with thiazide diuretics.
Which renal concentrating disorder is treated with thiazide diuretics?
What is the effect of thiazide diuretics on urinary calcium and which two conditions does this support treating?
Which thiazide diuretic is the 2nd most commonly prescribed antihypertensive?
Name other common thiazide or thiazide‑like diuretics and their typical oral dose ranges.
How are thiazide diuretics absorbed when given orally?
What is the plasma protein binding characteristic of thiazide diuretics?
How are most thiazide diuretics eliminated and which one is metabolized by the liver?
What are the typical half-lives of thiazide diuretics and of chlorthalidone?
What acid-base disturbance is commonly caused by thiazide diuretics?
Which two electrolytes are decreased by thiazide diuretics?
Which electrolytes or metabolic parameters can be increased by thiazide diuretics?
How can thiazides affect blood glucose in diabetics and why might this be worse with beta blockers?
Name two cardiovascular-related adverse effects or interactions of thiazide diuretics.
Which common drug class can decrease the effectiveness of thiazide diuretics?
What toxicity risk is increased by concomitant thiazide use?
What allergy cross-reactivity concern exists with thiazide diuretics?
Name two non-electrolyte adverse effects of thiazide diuretics mentioned.
What nephron segment is the main site of action for thiazide diuretics?
Which transporter is primarily inhibited by thiazide diuretics in the DCT?
Approximately what percentage of filtered Na+ is normally reabsorbed in the distal convoluted tubule?
List the main systemic effects of thiazide diuretics noted in the diagram.
Why do thiazides cause increased K+ loss in the collecting duct?
How do thiazides increase Ca²+ reabsorption in the DCT?
Refer to the diagram illustrating thiazide mechanism in the DCT (image). What is shown affecting Na+/Cl− transport?
For a patient taking HCTZ who is having surgery, what immediate action is advised regarding the medication?
What patient status should be assessed preoperatively for someone on HCTZ?
What volume state is noted for the patient taking HCTZ in this note?
Where do potassium-sparing diuretics act in the nephron?
What are the two classes of potassium-sparing diuretics?
What is the primary electrolyte effect of potassium-sparing diuretics?
How are potassium-sparing diuretics used clinically for hypertension?
Give an example of an aldosterone receptor blocker.
What is the primary therapeutic class name for drugs that conserve potassium?
What is the main mechanism of action of K+ sparing diuretics listed?
Name two examples of K+ sparing diuretics with their listed doses.
Are the listed K+ sparing diuretics dependent on aldosterone to work?
Which listed K+ sparing diuretic is more potent?
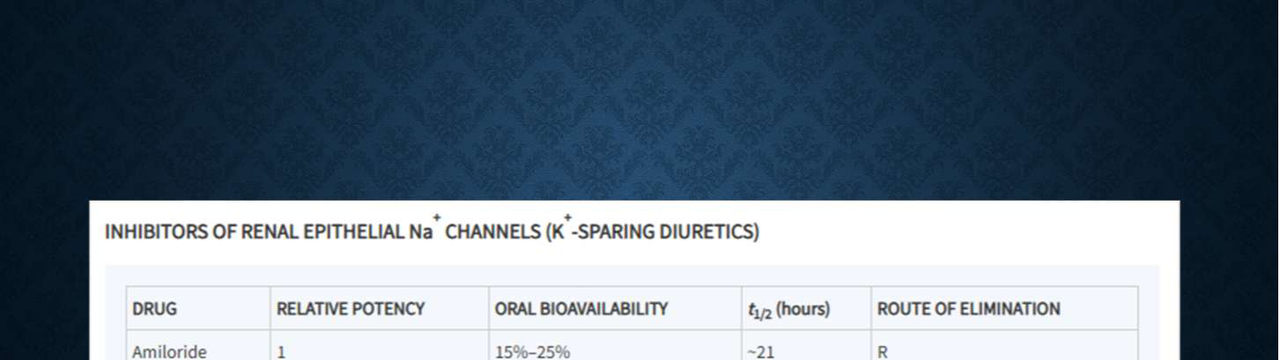
What is the mechanism/class of inhibitors of renal epithelial Na+ channels?
Which of the two drugs has higher relative potency: amiloride or triamterene?
Compare oral bioavailability, half-life, and route of elimination for amiloride versus triamterene.
What class of potassium-sparing diuretics blocks aldosterone receptors?
Name two aldosterone receptor blocker drugs and their dose ranges.
What is the primary mechanism of action of aldosterone receptor blocker diuretics?
What are two classes of K-sparing diuretics listed?
What is the primary electrolyte adverse effect of K-sparing diuretics?
Name three other side effects mentioned for K-sparing diuretics.
Which medications increase risk of adverse effects when given with K-sparing diuretics?
Which additional adverse effects are listed when K-sparing diuretics are given with ACE inhibitors or NSAIDs?
What is an osmotic diuretic?
How are osmotic diuretics handled at the glomerulus?
What are the primary sites of action for osmotic diuretics in the nephron?
Do osmotic diuretics cause greater excretion of water or electrolytes?
What does it mean that an osmotic diuretic is described as inert?
Give a common example of an osmotic diuretic.
What are the primary clinical uses of osmotic diuretics?
How do osmotic diuretics affect renal tubular fluid?
How does plasma osmolality contribute to the action of osmotic diuretics?
Name two additional pharmacologic effects of osmotic diuretics.
What is the only osmotic diuretic currently in clinical use?
Name other compounds that are osmotic agents mentioned alongside mannitol.
What is the chemical classification of mannitol?
How is mannitol metabolized in the body?
Why must mannitol be given intravenously to achieve a diuretic effect?
By what route is mannitol cleared from the body?
What are the key pharmacokinetic timing parameters of mannitol (onset, peak, duration)?
What is a main pharmacodynamic electrolyte risk of mannitol related to its diuretic effect?
What pulmonary risk does IV mannitol pose in patients with reduced ejection fraction (EF)?
What volume-related effect can prolonged mannitol use cause?
Which acid–base and electrolyte disturbance can mannitol cause?
What plasma change can occur with mannitol related to solute concentration?
What is the mechanism given for mannitol-induced plasma hyperosmolarity?
What risk does mannitol carry if the blood–brain barrier (BBB) is disrupted?
How can mannitol affect cerebral edema in the context of a disrupted BBB?
What are the main acute fractional excretion changes caused by inhibitors of carbonic anhydrase in the proximal tubule?
What are the main acute fractional excretion changes caused by osmotic diuretics (loop of Henle)?
What are the main acute fractional excretion changes caused by inhibitors of the Na+-K+-2Cl- symport (thick ascending limb)?
What are the main acute fractional excretion changes caused by inhibitors of the Na+-Cl- symport (distal convoluted tubule)?
What are the main acute fractional excretion changes caused by inhibitors of renal epithelial Na+ channels (late distal tubule, collecting duct)?
How do antagonists of mineralocorticoid receptors (late distal tubule, collecting duct) affect Na+ and K+ fractional excretion acutely?
What does the table note say about the context for the listed diuretic effects?
Which nephron segment is the main site of action for loop diuretics?
Where do thiazide diuretics mainly act in the nephron?
What is the main nephron site of action for carbonic anhydrase inhibitors?
Which diuretic class primarily acts on the collecting duct via the epithelial Na+ channel?
What is a key clinical use of loop diuretics listed in the table?
What is a primary clinical use of thiazide diuretics listed in the table?
Name the notable electrolyte-related side effect common to loop and thiazide diuretics.
What notable side effect is associated with carbonic anhydrase inhibitors?
Which diuretics are noted to cause hyperkalemia in the table?
Provide a visual summary of diuretic classes, sites, uses, and side effects.
Which nephron segment is the primary site of action for loop diuretics?
Which nephron segment is associated with K+‑sparing diuretics?
Which solute is shown as being handled in the proximal convoluted tubule (PCT) on the diagram?
Which ions are labeled as transported in the distal convoluted tubule (DCT) on the diagram?
What effect does ADH have on the collecting duct as shown in the diagram?
Name the main nephron parts illustrated in the diagram.
Which enzyme is targeted by acetazolamide as shown in the diagram?
Which transporter is targeted by thiazide diuretics according to the diagram?
Which drugs are listed in the diagram as associated with the epithelial Na+ cotransporter?
Which diuretic class is explicitly named 'Osmotic Diuretics' in the diagram?
What is the recommended perioperative action for chronic diuretics on the day of surgery (DOS)?
What preoperative assessments should be considered for patients on diuretics?
Which diuretics may be given during neurosurgical cases?
Which diuretic is often used in ophthalmology (eye) cases?
Which diuretic may be used if negative pressure pulmonary edema (NPPE) needs treatment?
Flashcards in this deck (214)
-
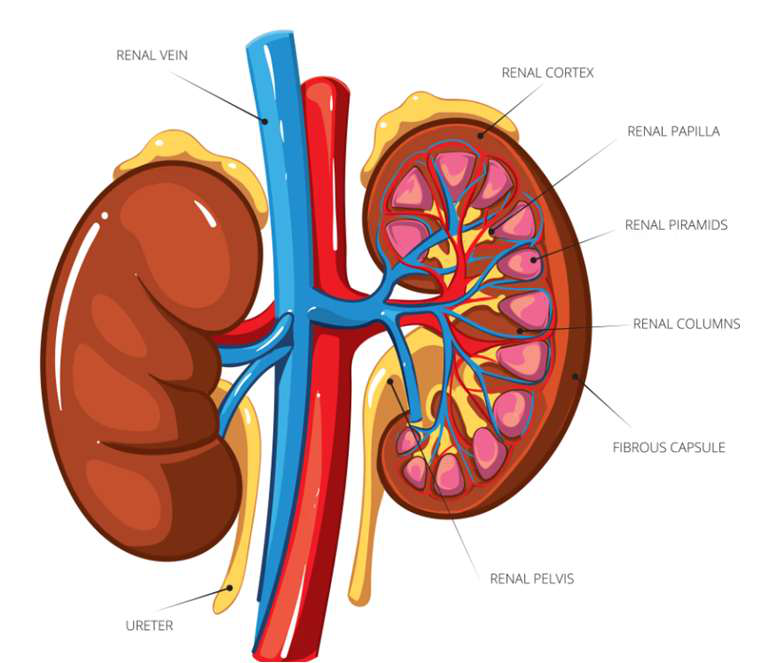
Name the major structures shown in a sagittal view of the kidney.
- Renal vein
- Renal cortex
- Renal papilla
- Renal pyramids
- Renal columns
- Fibrous capsule
- Renal pelvis
- Ureter
-
What are the primary learning goals regarding diuretic classes in this review?
- Differentiate among major diuretic classes by site, mechanism, and relative potency
-
What clinical decisions should be identified for each diuretic class?
- Clinical indications and contraindications for perioperative and chronic management
-
What adverse effects must be evaluated for each diuretic class?
- Common and clinically significant side effects, including implications for anesthesia practice
-
What should an anesthesia plan incorporate for patients taking diuretics?
- Fluid and electrolyte management, drug interactions, and physiologic response
-
How many times per day does the kidney filter the extracellular fluid volume (ECV) across the renal glomeruli?
~ 12 times/day
-
What are the primary regulatory functions of nephrons?
- Regulate bodily fluid and electrolytes
- Via secretion and reabsorption
-
What are the main anatomical segments of a nephron?
- Glomerular capsule
- Proximal convoluted tubule
- Loop of the nephron (loop of Henle)
- Distal convoluted tubule
- Collecting duct
-
Which blood vessels are directly associated with the nephron's blood supply?
- Afferent arteriole
- Peritubular capillary network
- Interlobular artery
- Interlobular vein
-
Describe the path urine takes from the nephron to the ureter.
- Urine flows from collecting duct
- into minor calyx → major calyx → renal pelvis → ureter
-
Name the major renal vessels and structural parts shown in the kidney diagram.
- Renal artery
- Segmental artery
- Interlobar artery and vein
- Arcuate artery and vein
- Cortical radiate artery
- Renal vein
- Renal pyramid
- Renal column
-
What structure surrounds the glomerulus in the nephron?
- Glomerular capsule
-
What is the primary pharmacologic effect of diuretics?
Increase the rate of sodium excretion and urine volume
-
By what general mechanism do most diuretics act within the nephron?
Most work by increasing Na+ reabsorption at varying sites within the nephron
-
What are common clinical indications for diuretic use?
- Fluid retention/overload
- Hypertension
- CHF
-
Which diuretic classes act at these nephron sites: proximal convoluted tubule, loop of Henle, distal convoluted tubule, and collecting duct?
- Carbonic anhydrase inhibitors: proximal convoluted tubule
- Loop diuretics: loop of Henle
- Thiazide diuretics: distal convoluted tubule
- Potassium-sparing diuretics: collecting duct
-
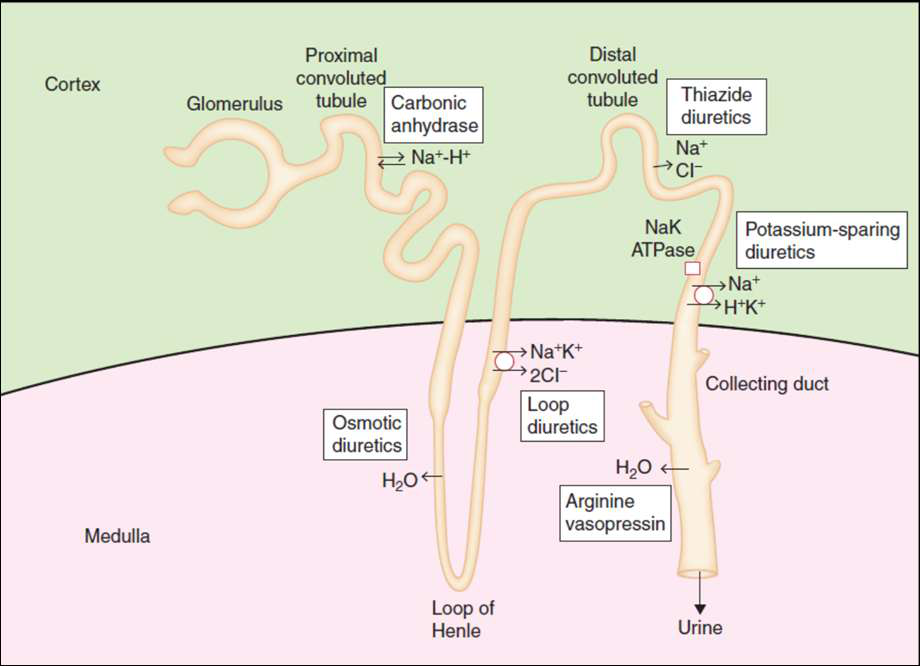
Which diuretic classes and related agents are depicted in the nephron diagram?
- Carbonic anhydrase inhibitors
- Loop diuretics
- Thiazide diuretics
- Potassium-sparing diuretics
- Osmotic diuretics
- Arginine vasopressin
-
Which hormone is shown in the diagram as relevant to renal water handling?
- Arginine vasopressin
Answer illustration:
-
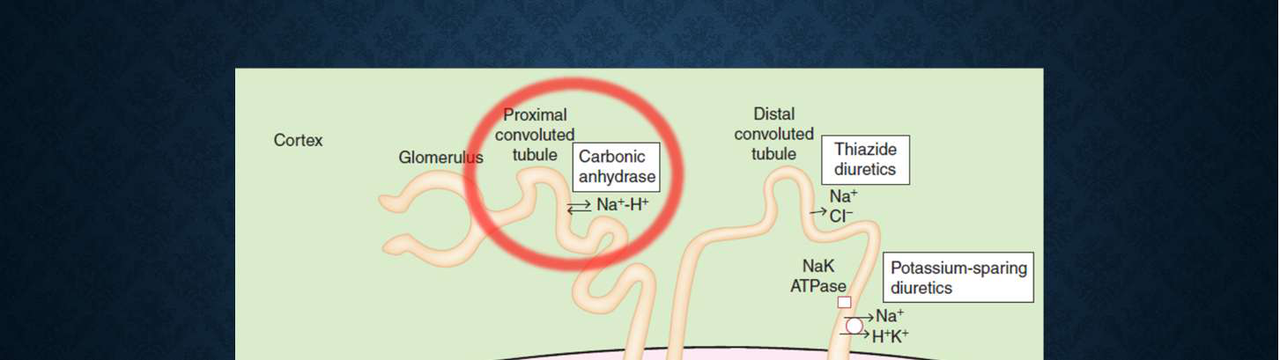
Which nephron segment is highlighted as the site of carbonic anhydrase action?
- Proximal convoluted tubule
-
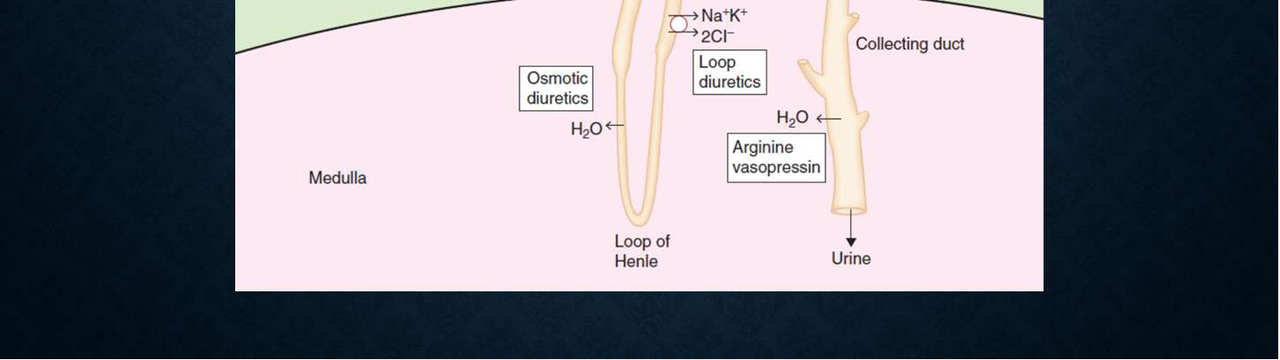
Which nephron segment is highlighted for the action of osmotic diuretics?
- Loop of Henle
-
What general nephron features does the diagram indicate relevant to diuretic pharmacology?
- Ion transport mechanisms and sites of action for various diuretic classes
-
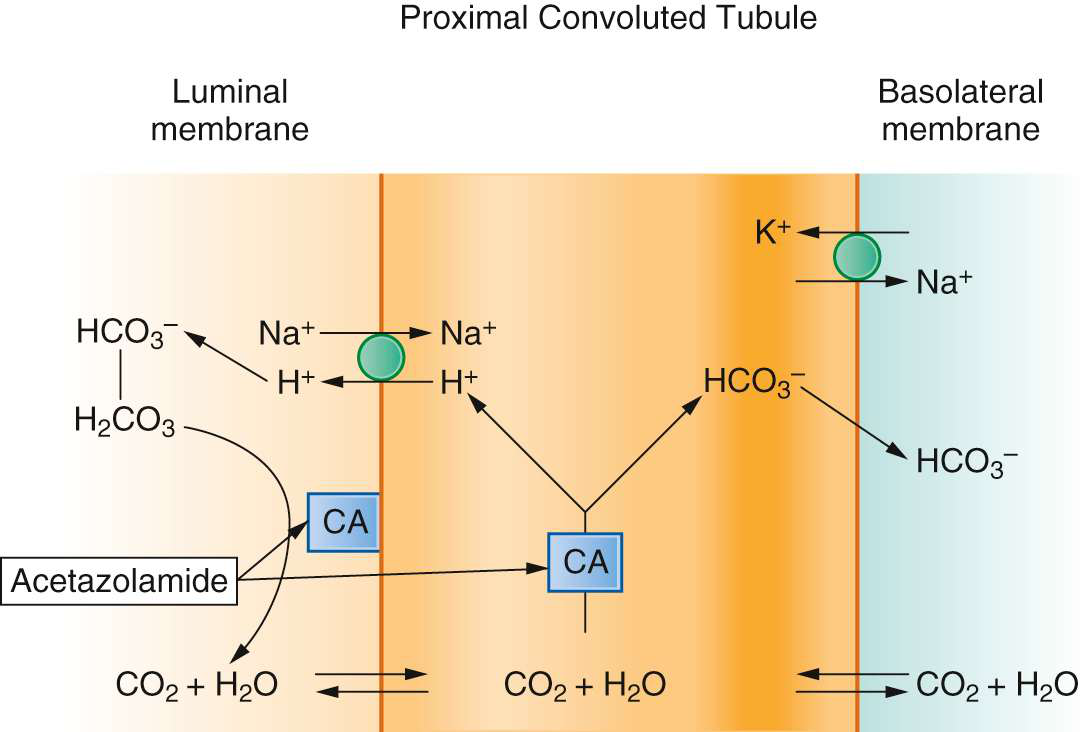
Where in the nephron is carbonic anhydrase activity primarily described in the text?
- Proximal convoluted tubule
- Collecting ducts
-
What is the role of the Na+/H+ exchanger in the renal tubule as described?
Reabsorbs Na+ and secretes H+ into the renal tubule, contributing to urine acidification.
-
Write the sequence of reactions involving bicarbonate and carbonic acid described in the text.
\(H^+ + HCO_3^- \rightleftharpoons H_2CO_3 \rightleftharpoons H_2O + CO_2\)
-
According to the text, which molecule crosses the tubular cell membrane during bicarbonate handling?
Carbon dioxide (CO2) crosses the tubular cell membrane.
-
What happens to carbonic acid within tubular cells and how are the products handled?
Carbonic acid is converted to H2O + CO2; intracellularly H+ is used by the Na+/H+ exchanger and HCO_3^- is released into the circulation.
-
What is the amount of acetazolamide per vial for injection labelled in the material?
- 500 mg
-
To which drug class does acetazolamide belong?
- Sulfonamide class
-
What is the mechanism of enzyme inhibition of acetazolamide?
- Non-competitive inhibition of carbonic anhydrase
-
Which nephron segment is primarily affected by acetazolamide's diuretic action?
- Proximal renal tubule
-
What reabsorptions are decreased by acetazolamide in the kidney?
- Sodium (Na)\n- Bicarbonate (HCO3)\n- Water (H2O)
-
Show the vial image of acetazolamide for intravenous use.
 \n- Label: Acetazolamide for injection, for intravenous use.
\n- Label: Acetazolamide for injection, for intravenous use.
-
Where in the nephron does acetazolamide primarily act?
- Proximal convoluted tubule
-
What is the mechanism of action of acetazolamide and its immediate effects on ion transport in the proximal tubule?
- Inhibits carbonic anhydrase (CA) → decreases HCO3- reabsorption, reduces H+ secretion, and reduces Na+ reabsorption
-
What are the primary clinical applications of acetazolamide (diamox)?
- Increased IOP/Glaucoma
- Idiopathic intracranial hypertension (formerly pseudotumor cerebri)
- Altitude sickness
- Edematous states
- HTN states
- Metabolic alkalosis

-
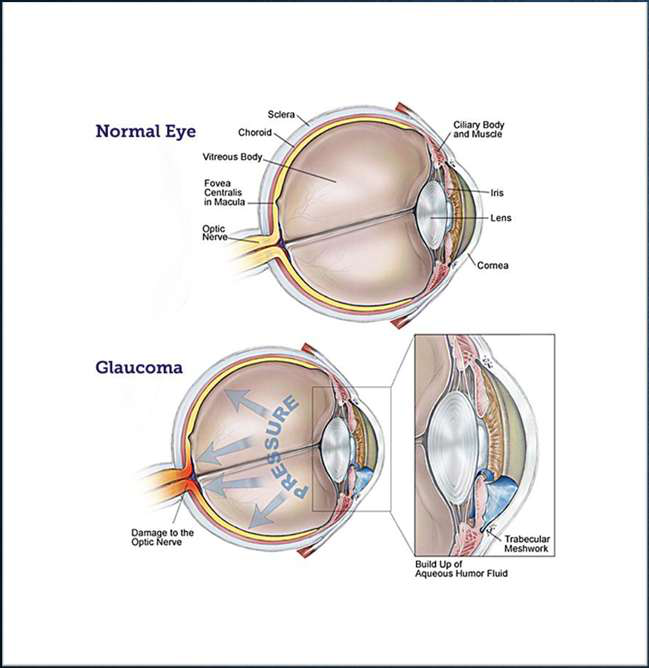
Which enzyme is present in the ciliary process of the eye involved in aqueous humor production?
- Carbonic anhydrase
-
What is the effect of inhibiting carbonic anhydrase in the ciliary process on aqueous humor and intraocular pressure (IOP)?
- Decreased aqueous humor production → Decreased IOP
-
What major structural damage can result from buildup of aqueous humor fluid in glaucoma?
- Damage to the optic nerve
-
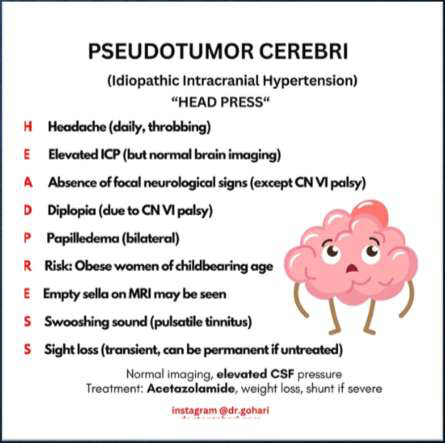
What is 'Pseudotumor cerebri' (Idiopathic Intracranial Hypertension)?
- A condition with elevated CSF pressure and normal brain imaging
-
What does the mnemonic 'HEAD PRESS' summarize for Idiopathic Intracranial Hypertension?
- Headache (daily, throbbing)
- Elevated ICP (with normal brain imaging)
- Absence of focal neurological signs (except CN VI palsy)
- Diplopia (CN VI palsy)
- Papilledema (bilateral)
- Risk: obese women of childbearing age
- Empty sella may be seen on MRI
- Swooshing sound (pulsatile tinnitus)
- Sight loss (transient or permanent)
-
What key diagnostic combination defines Idiopathic Intracranial Hypertension?
- Normal brain imaging with elevated CSF pressure
-
What are the main treatments for Idiopathic Intracranial Hypertension?
- Acetazolamide
- Weight loss
- Shunt if severe
-
What is 'acute high-altitude illness' (AHAI) or 'acute mountain sickness' (AMS)?
- Illness occurring at high altitudes due to insufficient acclimation leading to hypoxia-related symptoms
-
What is the primary initial physiological response to hypoxia at high altitude?
- Hyperventilation
-
Describe the ventilatory chemical sequence that can follow hypoxia at high altitude.
- Hypoxia → hyperventilation → respiratory alkalosis → ventilatory depression
-
How can metabolic acidosis affect ventilation in high-altitude illness?
- Metabolic acidosis can reverse hypoventilation
-
What drug is described as the cornerstone of therapy for acute high-altitude illness?
- Acetazolamide
-
What is Acute Mountain Sickness (AMS) primarily associated with?
Exposure to high altitude leading to physiological symptoms from hypobaric hypoxia
-
What cognitive or neuroimaging changes occur above 7000 m?
- MRI changes, including white matter hyperintensities
- Cortical atrophy
-
At what altitude do about 32% of climbers experience hallucinations?
Above 7500 m
-
Name some detectable psychomotor or cognitive impairments at high altitude (examples from the diagram).
- Psychomotor impairment detectable with FTT/pegboard
- Slowed complex reaction time
- Impaired learning and spatial memory
- Impaired memory retrieval
-
What altitude equivalent are commercial aircraft typically pressurised to?
An altitude equivalent of 1500–2500 m
-
What is the pharmacokinetic property of carbonic anhydrase (CA) inhibitors regarding excretion?
- CA inhibitors are given orally and are excreted unchanged
-
How should dosing of CA inhibitors be adjusted for elderly patients and those with chronic renal impairment (CRI)?
- Reduce dose in elderly and in patients with CRI
-
Should CA inhibitors be used in patients with severe chronic renal impairment (CRI)?
- Avoid CA inhibitors in patients with severe CRI
-
What is the primary pharmacodynamic effect of CA inhibitors on bicarbonate and urine pH?
- Increase excretion of HCO3- leading to alkaline urine and metabolic acidosis
-
What type of metabolic acidosis do CA inhibitors cause and what ion change accompanies it?
- Cause hyperchloremic metabolic acidosis with increased Cl- reabsorption in the loop of Henle
-
What are the effects of CA inhibitors on natriuresis and potassium balance?
- Produce modest natriuresis (up to 5% Na+ excretion) and increase distal Na+ delivery causing K+ loss
-
Is long-term administration of CA inhibitors considered a problem according to the notes?
- Long-term administration is noted as 'no problem with long-term admin'
-
What are common side effects of carbonic anhydrase inhibitors?
- Fatigue
- Decreased appetite
- Paresthesias
- Depression

-
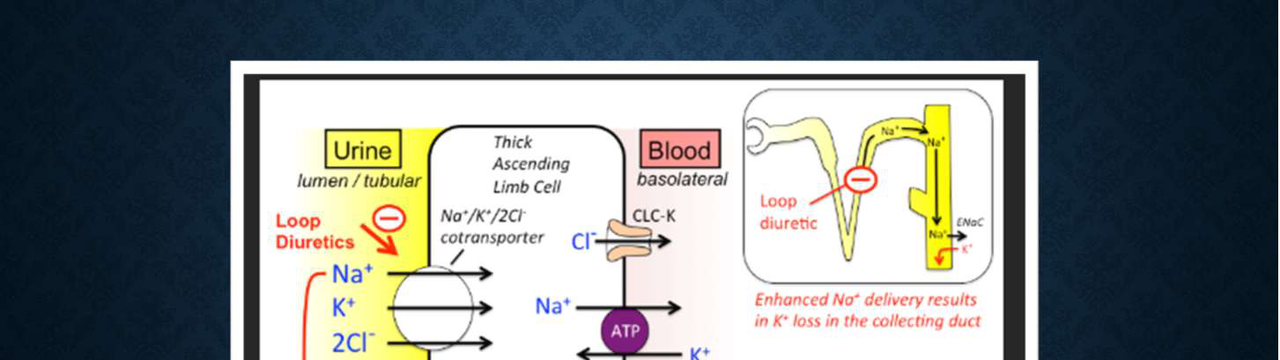
Which diuretic class is shown?
Loop diuretics
-
Where do loop diuretics act in the nephron?
- Medullary portion of the thick ascending limb of the Loop of Henle
-
Which transport protein is inhibited by loop diuretics?
- Na-K-2Cl transport protein
-
Which ions' reabsorption is inhibited by loop diuretics?
- Na+, K+, and Cl-
-
What proportion of filtered sodium is reabsorbed in the thick ascending limb?
- 20–30% of filtered Na+
-
Is the thick ascending limb of the Loop of Henle permeable to water?
- No — it is impermeable to H2O
-
What are two main physiological effects of diuresis from loop diuretics?
- Reduced intravascular volume
- Peripheral vasodilation

-
What is the relative potency of loop diuretics among diuretic classes?
- Loop diuretics are the most potent class of diuretics
-
How does response to loop diuretics change with dose?
- They have a dose-dependent response
-
What is the first-line indication for loop diuretics related to fluid overload?
- First-line therapy for heart failure-related fluid overload
-
Are loop diuretics first-line for treating hypertension in patients with normal kidney function?
- No; they are not first-line for hypertension with normal kidney function
-
Which transporter in the thick ascending limb is inhibited by loop diuretics?
- Na+/K+/2Cl cotransporter (NKCC2)
-
What fraction of filtered sodium is normally reabsorbed in the loop of Henle?
- 25% of filtered Na
-
How do loop diuretics affect divalent cation reabsorption (Ca2+, Mg2+)?
- Increase Ca2+ and Mg2+ loss
-
What acid-base and potassium disturbance is associated with loop diuretics?
- Hypokalemic metabolic alkalosis
-
Why do loop diuretics cause increased K+ loss in the collecting duct?
- Enhanced distal Na delivery results in K+ loss in the collecting duct
-
What class of diuretic is furosemide?
- Loop diuretic
-
How does furosemide affect cerebrospinal fluid (CSF) and intracranial pressure (ICP)?
- Reduces CSF production and ICP
-
Can alterations in the blood-brain barrier (BBB) change furosemide's effect on ICP?
- No; BBB alterations do not affect furosemide's effects on ICP
-
In what ways can furosemide be administered for ICP reduction?
- Single dose or in combination with mannitol
-
What are furosemide's oral absorption and protein binding characteristics?
- Oral absorption ~50%
- Protein binding 90% (albumin)
-
What is the elimination half-life and typical dose range of furosemide?
- Elimination half-life 1–2 hours (short duration)
- Dose 20–200 mg
-
What is the onset time of intravenous furosemide?
- Onset: 5–10 minutes
-
What is the peak effect time of furosemide?
- Peak: 30 minutes
-
What is the duration of action (DOA) of furosemide?
- DOA: 2–6 hours
-
What is the elimination half-life of furosemide?
- Elimination half-life: 1–2 hours
-
How is furosemide excreted?
- Excretion:
- 50–60% via glomerular filtration and tubular secretion
- 40–50% conjugated to glucuronide
-
What is the usual IV dose of furosemide in normal renal function and the typical range for renal insufficiency?
- Normal renal function: 20 mg
- Renal insufficiency: increased dose required, typically 160–200 mg
-
Is there benefit to giving more than 200 mg of furosemide IV?
- > 200 mg: no additional benefit
-
What ototoxic adverse effect can occur if furosemide is administered too quickly?
- Adverse effect: tinnitus if given too fast
-
Relative potency: how potent is bumetanide compared with furosemide?
- ~40× potency compared with furosemide
-
Key pharmacokinetics and usual dose for bumetanide (Bumex)?
- Bioavailability: 80–90% (PO)
- Routes: PO, IV, IM
- Metabolism: Mostly liver
- Dose: 0.5–2 mg
-
Core properties and starting dose for torsemide (Demadex)?
- Potency: ~3× furosemide
- Metabolism: Mostly liver
- Duration: Longer DOA; ½-life 3–4 hours (once-daily dosing)
- Dose (start): 10–20 mg

-
What is a key chemical characteristic of ethacrynic acid (Edecrin)?
- Non-sulfonamide
-
How does the potency of ethacrynic acid compare to furosemide?
- 70% potency of furosemide
-
What is the usual dose range for ethacrynic acid?
- 25-100 mg
-
What are the notable adverse effects of ethacrynic acid?
- Notable risk for ototoxicity
- Nausea
-
What are the main fluid/electrolyte and metabolic side effects of loop diuretics?
- Hypokalemia
- Hypovolemia
- Hyponatremia
- Hypomagnesemia
- Hyperglycemia
-
What is the 'braking phenomenon' with loop diuretics and what causes acute versus chronic tolerance?
- Braking phenomenon: acute or chronic tolerance to diuretic effects
- Acute cause: activation of the RAS
- Chronic cause: hypertrophy of the renal tubule
-
What ototoxicity risks are associated with loop diuretics?
- Ototoxicity occurs with all loop diuretics
- Can be transient or permanent
- Ethacrynic acid is noted in association with ototoxicity
-
Do loop diuretics have cross reactivity concerns with sulfa allergy?
- Yes — cross reactivity in patients with sulfa allergy
-
How do loop diuretics interact with nondepolarizing neuromuscular blocking agents (NMBAs)?
- Loop diuretics potentiate nondepolarizing NMBAs
-
What is the primary mechanism of action of thiazide diuretics?
- Inhibit the Na-Cl cotransporter in the renal tubule
-
At which nephron segment do thiazide diuretics act?
- Early distal convoluted tubule
-
Which major electrolyte changes do thiazide diuretics cause in urine and blood?
- Increase urinary excretion: Na+, Cl-, K+
- Increase renal reabsorption: Ca++
-
What are the early and sustained physiological effects of thiazide diuretics?
- Early: decrease ECF volume and cardiac output
- Sustained: vasodilatation developing over weeks
-
What is the primary antihypertensive indication for thiazide diuretics?
- Essential hypertension
-
How are thiazide diuretics commonly used in relation to other antihypertensives?
- Often given with other antihypertensives
-
Name two cardiovascular or fluid-overload conditions treated with thiazide diuretics.
- Edema
- Congestive heart failure (CHF)
-
Which renal concentrating disorder is treated with thiazide diuretics?
- Diabetes insipidus (DI)
-
What is the effect of thiazide diuretics on urinary calcium and which two conditions does this support treating?
- Reduce urinary Ca++ excretion
- Used for hypocalcemia
- Used for osteoporosis
-
Which thiazide diuretic is the 2nd most commonly prescribed antihypertensive?
- Hydrochlorothiazide (HCTZ)
-
Name other common thiazide or thiazide‑like diuretics and their typical oral dose ranges.
- Hydrochlorothiazide (HCTZ): 12.5–50 mg
- Chlorthalidone: 12.5–50 mg
- Indapamide: 1.25–5 mg
- Metolazone: 1.25–5 mg
-
How are thiazide diuretics absorbed when given orally?
- Readily absorbed
-
What is the plasma protein binding characteristic of thiazide diuretics?
- Highly protein bound
-
How are most thiazide diuretics eliminated and which one is metabolized by the liver?
- Most eliminated unchanged
- Indapamide is metabolized by the liver
-
What are the typical half-lives of thiazide diuretics and of chlorthalidone?
- Thiazides: 8–12 hours
- Chlorthalidone: 50–60 hours
-
What acid-base disturbance is commonly caused by thiazide diuretics?
- Hypokalemic, hypochloremic metabolic alkalosis
-
Which two electrolytes are decreased by thiazide diuretics?
- Potassium (hypokalemia)
- Magnesium (hypomagnesemia)
-
Which electrolytes or metabolic parameters can be increased by thiazide diuretics?
- Calcium (hypercalcemia)
- Uric acid (hyperuricemia)
-
How can thiazides affect blood glucose in diabetics and why might this be worse with beta blockers?
- Can cause hyperglycemia in diabetics, possibly from decreased insulin release; effect may be greater in patients taking beta blockers
-
Name two cardiovascular-related adverse effects or interactions of thiazide diuretics.
- Dysrhythmias
- Can potentiate nondepolarizing neuromuscular blockers (NMBAs)
-
Which common drug class can decrease the effectiveness of thiazide diuretics?
- NSAIDs
-
What toxicity risk is increased by concomitant thiazide use?
- Potential for lithium toxicity
-
What allergy cross-reactivity concern exists with thiazide diuretics?
- Cross reactivity in patients with sulfa allergy
-
Name two non-electrolyte adverse effects of thiazide diuretics mentioned.
- Hyperlipidemia
- Sexual dysfunction
-
What nephron segment is the main site of action for thiazide diuretics?
The distal convoluted tubule (DCT)
-
Which transporter is primarily inhibited by thiazide diuretics in the DCT?
- Na+/Cl− cotransporter (NCC)
-
Approximately what percentage of filtered Na+ is normally reabsorbed in the distal convoluted tubule?
About 10% of filtered Na+ is reabsorbed in the DCT
-
List the main systemic effects of thiazide diuretics noted in the diagram.
- Loss of Na & Water
- Hypokalemic metabolic alkalosis
- Increased Ca²+ reabsorption
-
Why do thiazides cause increased K+ loss in the collecting duct?
Enhanced distal Na+ delivery increases Na+ reabsorption in the collecting duct, causing K+ loss
-
How do thiazides increase Ca²+ reabsorption in the DCT?
- Lower intracellular Na+ facilitates Ca²+ reabsorption via apical TRPV5 and basolateral Na+/Ca²+ exchange
-
Refer to the diagram illustrating thiazide mechanism in the DCT (image). What is shown affecting Na+/Cl− transport?
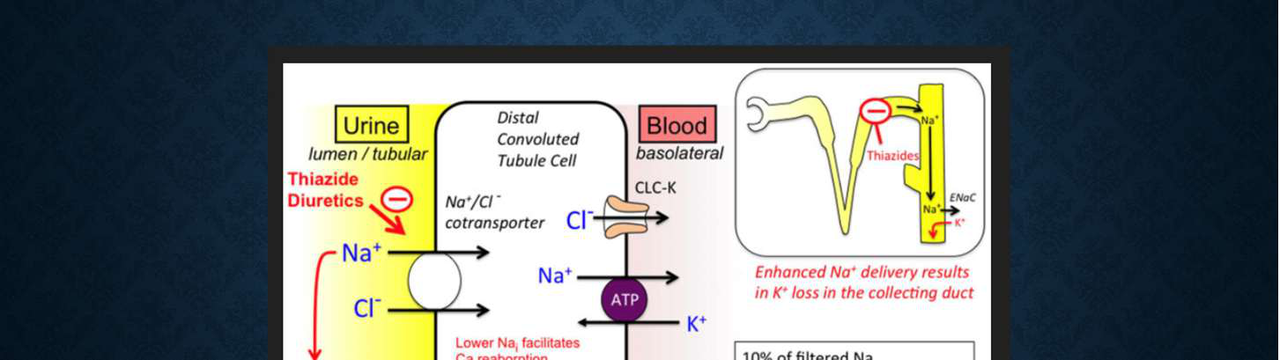 - Thiazide inhibition of the Na+/Cl− cotransporter (NCC)
- Thiazide inhibition of the Na+/Cl− cotransporter (NCC) -
For a patient taking HCTZ who is having surgery, what immediate action is advised regarding the medication?
- Hold the dose
-
What patient status should be assessed preoperatively for someone on HCTZ?
- Intravascular fluid volume status
-
What volume state is noted for the patient taking HCTZ in this note?
- Volume contracted
-
Where do potassium-sparing diuretics act in the nephron?
- Late distal tubule (Late DT)
- Collecting ducts
-
What are the two classes of potassium-sparing diuretics?
- Pteridine analogues
- Aldosterone receptor blockers
-
What is the primary electrolyte effect of potassium-sparing diuretics?
They decrease Na+ absorption without increased K+ secretion, sparing potassium.
-
How are potassium-sparing diuretics used clinically for hypertension?
They are not used as single treatment for hypertension; used in combination with loop or thiazide diuretics.
-
Give an example of an aldosterone receptor blocker.
- Spironolactone (Aldactone)

-
What is the primary therapeutic class name for drugs that conserve potassium?
- K+ sparing diuretics
-
What is the main mechanism of action of K+ sparing diuretics listed?
- Block renal epithelial Na+ channels
-
Name two examples of K+ sparing diuretics with their listed doses.
- Amiloride 5–10 mg
- Triamterene 50–150 mg
-
Are the listed K+ sparing diuretics dependent on aldosterone to work?
- Independent of Aldosterone
-
Which listed K+ sparing diuretic is more potent?
- Amiloride > Triamterene
-
What is the mechanism/class of inhibitors of renal epithelial Na+ channels?
- K+-sparing diuretics
- Mechanism: Inhibition of renal epithelial Na+ channels
-
Which of the two drugs has higher relative potency: amiloride or triamterene?
- Amiloride: relative potency 1
- Triamterene: relative potency 0.1
-
Compare oral bioavailability, half-life, and route of elimination for amiloride versus triamterene.
- Amiloride: oral bioavailability 15%–25%, t<sub>1/2</sub> ~21 h, route renal excretion (R)
- Triamterene: oral bioavailability ~50%, t<sub>1/2</sub> ~4 h, route metabolism to active metabolite, urinary excretion (M)
-
What class of potassium-sparing diuretics blocks aldosterone receptors?
Aldosterone receptor blockers (potassium-sparing diuretics).
-
Name two aldosterone receptor blocker drugs and their dose ranges.
- Spironolactone: 12.5–100 mg
- Eplerenone: 25–50 mg
-
What is the primary mechanism of action of aldosterone receptor blocker diuretics?
They prevent synthesis and activation of the aldosterone-dependent Na-K-ATPase pump.
-
What are two classes of K-sparing diuretics listed?
- Pteridine analogues
- Aldosterone antagonists
-
What is the primary electrolyte adverse effect of K-sparing diuretics?
- Hyperkalemia
-
Name three other side effects mentioned for K-sparing diuretics.
- Metabolic acidosis
- GI disturbances
- Nephrolithiasis
-
Which medications increase risk of adverse effects when given with K-sparing diuretics?
- ACE inhibitors
- NSAIDs
-
Which additional adverse effects are listed when K-sparing diuretics are given with ACE inhibitors or NSAIDs?
- Metabolic acidosis
- GI disturbances
- Libido changes (impotence)
- Gynecomastia
-
What is an osmotic diuretic?
An inert substance that is filtered freely at the glomerulus and promotes diuresis.
-
How are osmotic diuretics handled at the glomerulus?
They are filtered freely at the glomerulus.
-
What are the primary sites of action for osmotic diuretics in the nephron?
- Loop of Henle
- Proximal tubules
-
Do osmotic diuretics cause greater excretion of water or electrolytes?
Water excreted > electrolytes
-
What does it mean that an osmotic diuretic is described as inert?
It does not undergo metabolism.
-
Give a common example of an osmotic diuretic.
- Mannitol

-
What are the primary clinical uses of osmotic diuretics?
- Increased intracranial pressure in TBI
- Reducing cerebral edema & brain mass in neurosurgery
- Glaucoma
-
How do osmotic diuretics affect renal tubular fluid?
- Increase renal tubular fluid osmolality
-
How does plasma osmolality contribute to the action of osmotic diuretics?
- Increased plasma osmolality draws fluid from the extracellular space (ECF) into the intravascular compartment
-
Name two additional pharmacologic effects of osmotic diuretics.
- Osmotic diuresis
- Scavenging of O2 free radicals
-
What is the only osmotic diuretic currently in clinical use?
- Mannitol
-
Name other compounds that are osmotic agents mentioned alongside mannitol.
- Urea
- Isosorbide
- Glycerin
-
What is the chemical classification of mannitol?
- Six-carbon sugar alcohol
-
How is mannitol metabolized in the body?
- It undergoes no metabolism
-
Why must mannitol be given intravenously to achieve a diuretic effect?
- It is not absorbed in the GIT; IV administration is required for diuresis
-
By what route is mannitol cleared from the body?
- Clearance occurs only by glomerular filtration
-
What are the key pharmacokinetic timing parameters of mannitol (onset, peak, duration)?
- Onset: 10–15 min
- Peak: 40–45 min
- Duration of action: 6 hours
-
What is a main pharmacodynamic electrolyte risk of mannitol related to its diuretic effect?
- Potential hypernatremia from water diuresis
-
What pulmonary risk does IV mannitol pose in patients with reduced ejection fraction (EF)?
- Pulmonary edema (due to initial IV volume expansion)
-
What volume-related effect can prolonged mannitol use cause?
- Hypovolemia
-
Which acid–base and electrolyte disturbance can mannitol cause?
- Hypokalemic, hypochloremic alkalosis
-
What plasma change can occur with mannitol related to solute concentration?
- Plasma hyperosmolarity
-
What is the mechanism given for mannitol-induced plasma hyperosmolarity?
- Excessive Na+ and water excretion
-
What risk does mannitol carry if the blood–brain barrier (BBB) is disrupted?
- Rebound intracranial hypertension
-
How can mannitol affect cerebral edema in the context of a disrupted BBB?
- It can worsen cerebral edema
-
What are the main acute fractional excretion changes caused by inhibitors of carbonic anhydrase in the proximal tubule?
- Na+: ++
- K+: +
- HCO3-: +
-
What are the main acute fractional excretion changes caused by osmotic diuretics (loop of Henle)?
- Na+: +
- K+: ++
- Mg2+: +
- Cl-: +
- HCO3-: +
- H2PO4-: +
-
What are the main acute fractional excretion changes caused by inhibitors of the Na+-K+-2Cl- symport (thick ascending limb)?
- Na+: ++
- Ca2+: ++
- Mg2+: +
- Cl-: ++
- HCO3-: +
- H2PO4-: +
-
What are the main acute fractional excretion changes caused by inhibitors of the Na+-Cl- symport (distal convoluted tubule)?
- Na+: +
- K+: +
- Ca2+: +
- Mg2+: +
- Cl-: +
- HCO3-: +
- H2PO4-: +
-
What are the main acute fractional excretion changes caused by inhibitors of renal epithelial Na+ channels (late distal tubule, collecting duct)?
- Na+: +
- K+: -
- Other anions/cations: NC
-
How do antagonists of mineralocorticoid receptors (late distal tubule, collecting duct) affect Na+ and K+ fractional excretion acutely?
- Na+: +
- K+: -
-
What does the table note say about the context for the listed diuretic effects?
- Effects (except uric acid) are for acute diuretic use in the absence of significant volume depletion, which would trigger complex adjustments.
-
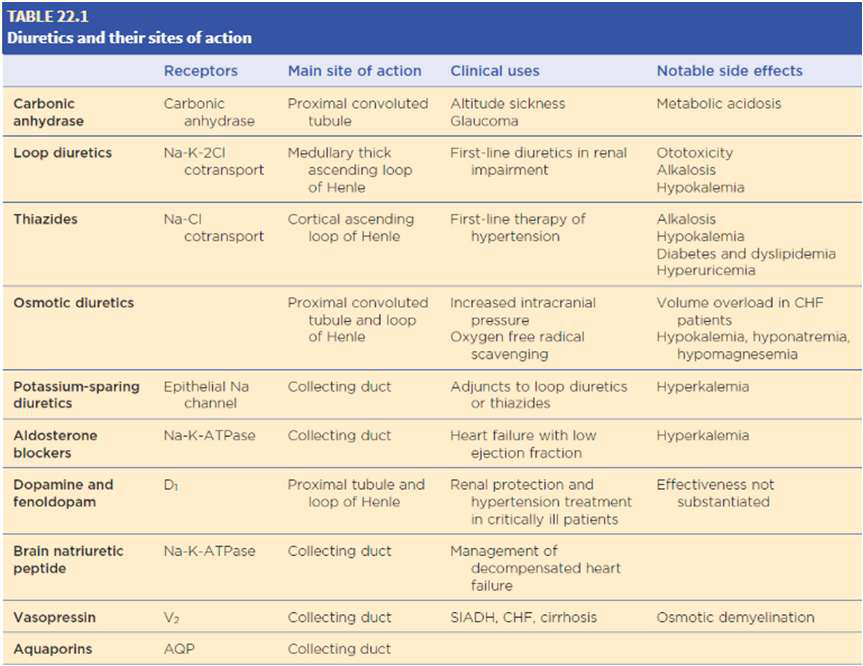
Which nephron segment is the main site of action for loop diuretics?
Medullary thick ascending loop of Henle
-
Where do thiazide diuretics mainly act in the nephron?
Cortical ascending loop of Henle
-
What is the main nephron site of action for carbonic anhydrase inhibitors?
Proximal convoluted tubule
-
Which diuretic class primarily acts on the collecting duct via the epithelial Na+ channel?
Potassium-sparing diuretics
-
What is a key clinical use of loop diuretics listed in the table?
First-line diuretics in renal impairment
-
What is a primary clinical use of thiazide diuretics listed in the table?
First-line therapy of hypertension
-
Name the notable electrolyte-related side effect common to loop and thiazide diuretics.
Hypokalemia
-
What notable side effect is associated with carbonic anhydrase inhibitors?
Metabolic acidosis
-
Which diuretics are noted to cause hyperkalemia in the table?
Aldosterone blockers and potassium-sparing diuretics
-
Provide a visual summary of diuretic classes, sites, uses, and side effects.
- See table image summarizing classes, sites, clinical uses, and notable side effects:
-
Which nephron segment is the primary site of action for loop diuretics?
Thick ascending limb (Loop of Henle)
-
Which nephron segment is associated with K+‑sparing diuretics?
Collecting duct (principal cells)
-
Which solute is shown as being handled in the proximal convoluted tubule (PCT) on the diagram?
NaHCO3 (sodium bicarbonate)
-
Which ions are labeled as transported in the distal convoluted tubule (DCT) on the diagram?
Na+ and Cl-
-
What effect does ADH have on the collecting duct as shown in the diagram?
Increases water (H2O) reabsorption
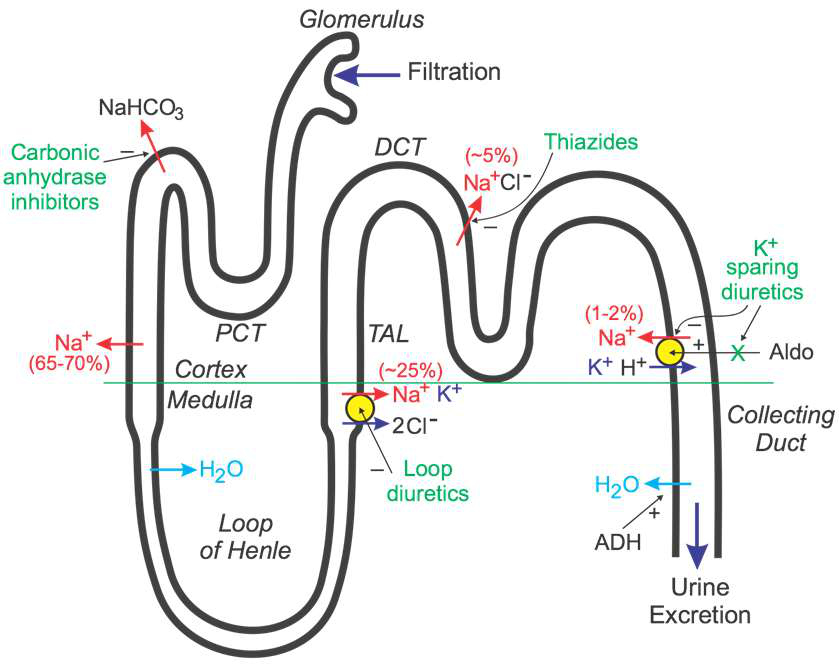
-
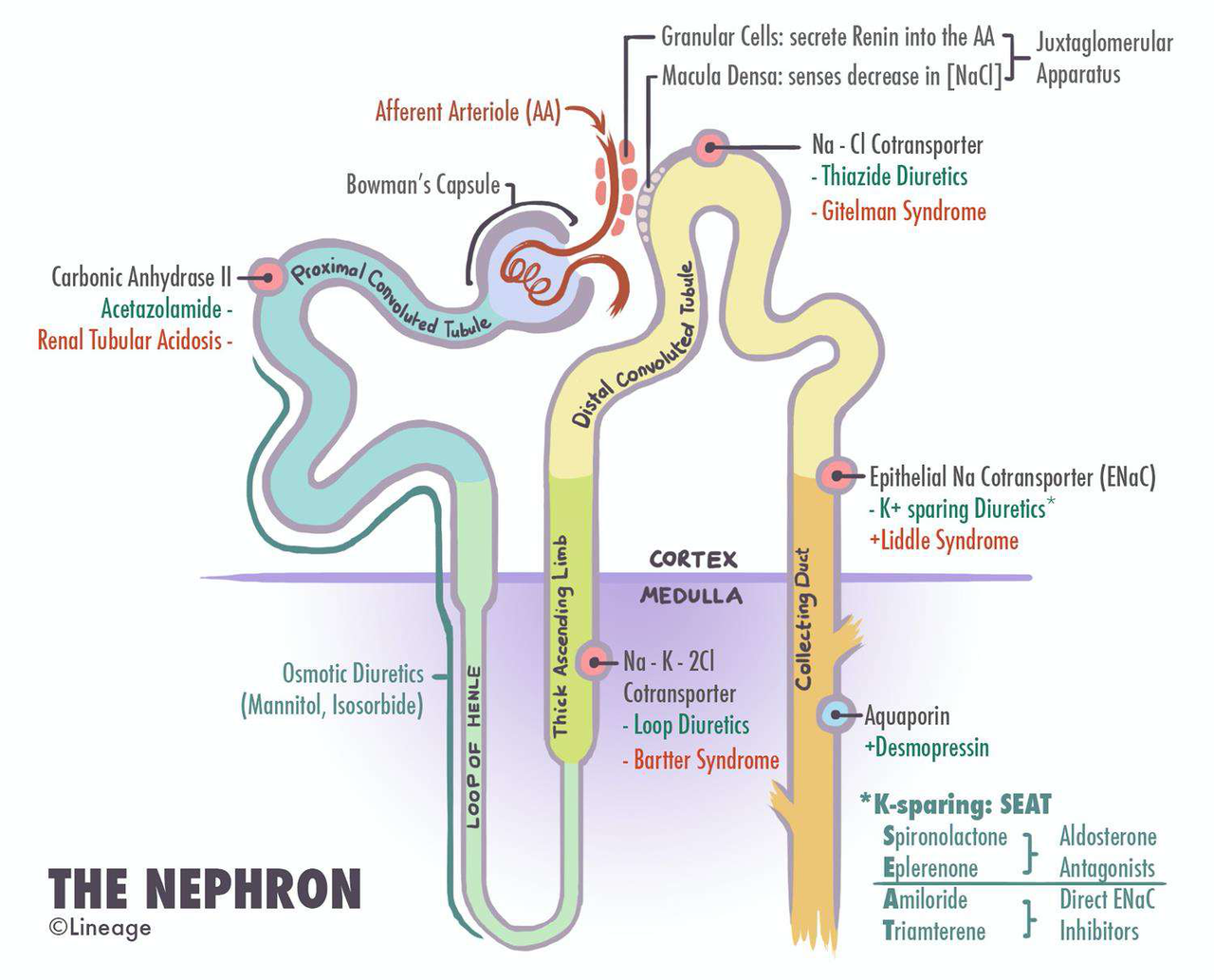
Name the main nephron parts illustrated in the diagram.
- Afferent Arteriole
- Bowman's Capsule
- Proximal Convoluted Tubule (PCT)
- Loop of Henle
- Distal Convoluted Tubule (DCT)
- Collecting Duct
-
Which enzyme is targeted by acetazolamide as shown in the diagram?
- Carbonic Anhydrase II
-
Which transporter is targeted by thiazide diuretics according to the diagram?
- Na-Cl cotransporter
-
Which drugs are listed in the diagram as associated with the epithelial Na+ cotransporter?
- Spironolactone
- Eplerenone
- Amiloride
- Triamterene
-
Which diuretic class is explicitly named 'Osmotic Diuretics' in the diagram?
- Osmotic Diuretics
-
What is the recommended perioperative action for chronic diuretics on the day of surgery (DOS)?
- Hold diuretics on the day of surgery (DOS).
-
What preoperative assessments should be considered for patients on diuretics?
- Review recent lab work, acid-base status, and volume status.
-
Which diuretics may be given during neurosurgical cases?
- Mannitol
- Lasix (furosemide)
-
Which diuretic is often used in ophthalmology (eye) cases?
- Acetazolamide
-
Which diuretic may be used if negative pressure pulmonary edema (NPPE) needs treatment?
- Lasix (furosemide)
Overview
- Diuretics increase urinary sodium excretion and urine volume by inhibiting specific transporters along the nephron.
- Major clinical uses: fluid overload, hypertension, heart failure, edema, and specific indications (e.g., glaucoma, altitude sickness, raised intracranial pressure).
Kidney & Nephron (quick reference)
Alt: Sagittal kidney view with major structures.
- The nephron segments and major transporters determine where each diuretic acts.
Alt: Nephron diagram showing diuretic class action sites.
Classification & Key actions (concise table)
| Class | Main site | Primary effect | Clinical highlight |
|---|---|---|---|
| Carbonic anhydrase inhibitors | Proximal tubule | ↑HCO3- excretion, mild natriuresis | Altitude sickness, glaucoma, IIH |
| Loop diuretics | Thick ascending limb (TAL) | Potent Na+ loss; inhibit NKCC2 | Most potent; acute pulmonary edema |
| Thiazides | Early distal convoluted tubule (DCT) | ↓NaCl reabsorption; ↑Ca2+ reabsorption | First-line HTN therapy |
| K+-sparing (ENaC blockers / aldosterone antagonists) | Late DCT / collecting duct | Reduce Na+ reabsorption without K+ loss | Use with loops/thiazides to spare K+ |
| Osmotic diuretics | PCT & loop | Water diuresis > electrolyte loss | Mannitol for increased ICP/brain edema |
Carbonic Anhydrase Inhibitors (e.g., Acetazolamide)
- Mechanism: Noncompetitive inhibition of carbonic anhydrase in proximal tubule and collecting ducts → ↓HCO3- reabsorption, alkaline urine, metabolic hyperchloremic acidosis.
- Effect size: Modest natriuresis (≈ up to 5% filtered Na+).
- Indications: Acute mountain sickness, glaucoma (↓aqueous humor), idiopathic intracranial hypertension (pseudotumor cerebri), some metabolic alkalosis states.
- PK/PD notes: Oral drug largely excreted unchanged; reduce dose with renal impairment; avoid in severe CRI.
- Adverse effects: Fatigue, paresthesias, metabolic acidosis, hypokalemia (due to distal K+ loss).
- Anesthesia considerations: Often held day of surgery; consider acid-base and volume status; acetazolamide sometimes seen preop for eye cases or IIH.
Loop Diuretics (e.g., Furosemide, Bumetanide, Torsemide, Ethacrynic acid)
- Mechanism: Inhibit Na+-K+-2Cl- cotransporter (NKCC2) in TAL → loss of Na+, K+, Cl- and increased Ca2+/Mg2+ excretion.
- Physiology: TAL normally reabsorbs about \(20\%-30\%\) of filtered Na+; inhibition causes powerful natriuresis and diuresis.
- Potency & examples: Most potent diuretics. Bumetanide ≈ 40× furosemide potency; torsemide longer duration; ethacrynic acid is non-sulfonamide (use if sulfa allergy) but has higher ototoxicity risk.
- PK highlights (furosemide): Onset IV 5–10 min; peak ≈30 min; DOA 2–6 h; half-life ~1–2 h; bioavailability ≈50% PO; highly protein bound.
- Indications: Acute pulmonary edema, heart failure with fluid overload, refractory edema, sometimes to lower ICP (adjunct).
- Adverse effects: Hypokalemia, hyponatremia, hypomagnesemia, metabolic alkalosis, ototoxicity (esp. with aminoglycosides or ethacrynic acid), hypotension, volume depletion.
- Drug interactions: NSAIDs blunt effect; aminoglycosides increase ototoxicity; digoxin toxicity risk with hypokalemia; potentiation of nondepolarizing neuromuscular blockers.
- Anesthesia considerations: Hold chronic diuretics DOS; check electrolytes & intravascular volume; be ready to manage hypovolemia and dysrhythmias; note interactions with NMBAs.
Thiazide Diuretics (e.g., HCTZ, Chlorthalidone, Indapamide, Metolazone)
- Mechanism: Inhibit Na+-Cl- cotransporter (NCC) in early DCT → ↑Na+ and Cl- excretion, reduce urinary Ca2+ excretion (↑Ca2+ reabsorption).
- Physiology: DCT normally handles ≈ \(10\%\) of filtered Na+; thiazides cause mild-moderate natriuresis but have chronic vasodilatory effects for BP reduction.
- Indications: First-line for essential hypertension, mild edema, nephrogenic diabetes insipidus (low doses reduce polyuria), reduce urinary Ca2+ (benefit in kidney stones/osteoporosis).
- PK notes: Orally absorbed; chlorthalidone has a long half-life (≈50–60 h).
- Adverse effects: Hypokalemic, hypochloremic metabolic alkalosis; hyperglycemia; hyperuricemia; hypercalcemia; hypomagnesemia; dyslipidemia; can potentiate NMBAs.
- Anesthesia considerations: Hold day of surgery; evaluate volume status and electrolytes; watch glucose and uric acid in susceptible patients.
Potassium-sparing Diuretics
- Two subtypes:
- ENaC blockers (amiloride, triamterene): Directly block epithelial Na+ channels in collecting duct; reduce Na+ reabsorption and K+ excretion.
- Aldosterone antagonists (spironolactone, eplerenone): Block mineralocorticoid receptor → reduce synthesis/activation of Na+-K+ pump; useful in hyperaldosteronism and heart failure.
- Indications: Adjunct to loop/thiazide to prevent hypokalemia; spironolactone for heart failure and hyperaldosteronism.
- Adverse effects: Hyperkalemia (especially with ACE inhibitors, ARBs, NSAIDs), metabolic acidosis, GI upset; spironolactone may cause gynecomastia/sexual side effects; eplerenone is more selective (less endocrine effects).
- Anesthesia considerations: Check K+ preop; avoid perioperative hyperkalemia risk with ACE inhibitors/ARB overlap.
Osmotic Diuretics (Mannitol)
- Mechanism: Freely filtered inert osmole that increases tubular fluid osmolality → water diuresis > electrolyte loss.
- Uses: Reduce intracranial pressure and cerebral edema (acute TBI, neurosurgery), acute renal protection in some settings, and to decrease intraocular pressure.
- PK: IV only; onset 10–15 min, peak 40–45 min, duration ≈ 6 h; eliminated by glomerular filtration.
- Adverse effects & cautions: Initial intravascular volume expansion (can precipitate pulmonary edema in heart failure), subsequent hypovolemia with continued diuresis, hypernatremia, plasma hyperosmolarity, risk of rebound intracranial hypertension if blood–brain barrier is disrupted.
- Anesthesia considerations: Use cautiously in low EF patients; monitor hemodynamics and serum osmolality; mannitol often given intraop in neurosurgical cases.
Electrolyte & Acid-Base Patterns (practical)
- Loops & thiazides: typically cause hypokalemia and metabolic alkalosis.
- Carbonic anhydrase inhibitors: cause metabolic acidosis with alkaline urine.
- Potassium-sparing/aldosterone antagonists: risk hyperkalemia and metabolic acidosis.
- Osmotics: risk hypernatremia (water loss) and transient volume changes.
Perioperative Practical Points
- General: Hold most diuretics on day of surgery (DOS) unless directed otherwise; assess recent labs, volume status, and electrolytes.
- When diuretics may be given periop: Mannitol or furosemide may be administered intraop for neurosurgical indications or acute pulmonary edema (NPPE).
- Electrolyte monitoring: Check K+, Na+, Mg2+, glucose, and acid–base status preop; correct significant abnormalities.
- Drug interactions to note: NSAIDs reduce diuretic efficacy; hypokalemia increases risk of digoxin toxicity and arrhythmias; diuretics can potentiate nondepolarizing neuromuscular blockers.
Quick clinical tips
- If patient takes HCTZ and is having surgery: hold the dose DOS and evaluate intravascular volume—they may be volume-contracted.
- For severe loop-diuretic resistance consider combination therapy (loop + thiazide/metolazone) under supervision.
- Be cautious combining ACE inhibitors/ARBs with K+-sparing agents.
High-yield summary (one-line reminders)
- Loops: most potent → careful with electrolytes and ototoxicity.
- Thiazides: HTN first-line, watch glucose/uric acid and K+.
- CA inhibitors: altitude, glaucoma, IIH, cause metabolic acidosis.
- K+-sparing: prevent hypokalemia but risk hyperkalemia.
- Mannitol: reduce ICP, but watch for volume shifts and rebound edema.
References / further reading
- Stoelting's Pharmacology & Physiology in Anesthetic Practice, Ch. 22: Diuretics.
- Goodman & Gilman: Drugs affecting renal excretory function (selected sections).